4649
Effect of respiratory motion on gated torso MRI in an upright 0.5 T scanner with seated and standing subjects1University of Nottingham, Nottingham, United Kingdom
Synopsis
Keywords: Motion Correction, Motion Correction, Torso, Optical Tracking, Upright
Motivation: The study focuses on the development of a MoCo technique for torso MRI in upright scanner.
Goal(s): Respiratory gated MRI acquisition was achieved by tracking respiratory-related torso motion under the rigid-body assumption.
Approach: Optical tracking of torso motion was used to trigger the MRI acquisition at the beginning of each exhalation period.
Results: Respiratory gating reduces motion induced artefacts in MRI of seated subjects, but was not able to eliminate motion effects in MRI of standing subjects. In its future development it would be paired with retrospective motion correction technique
Impact: The aim is to improve MR image quality on an 0.5T upright scanner where body motion is mostly unconstrained. It would particularly improve image quality in patients who are not supine, so increasing patient comfort and reducing the scanning time.
Introduction
Open MRI scanner improves patients comfort and allows the study of physiology in natural poses. The upright position imposes limited constraints on body motion compared to conventional, supine MRI which tends to limit motion1. Upright body MRI presents several challenges: increased bulk-body motion2, the effects of respiratory motion and motion of the internal organs1.To prevent motion artefacts, we need to simultaneously monitoring both gross motion3 and respiratory-related motion. We have previously shown that respiratory motion can be tracked in the standing and seated positions using optical markers placed on the upper body2. However, motion parameters need to be combined appropriately to produce a robust respiratory signal.
Aim: to test an improved2 algorithm to detect respiratory movement in upright MRI from a motion tracking system and to determine the extent of residual bulk movement once the effects of respiration have been overcome by triggering.
Methods
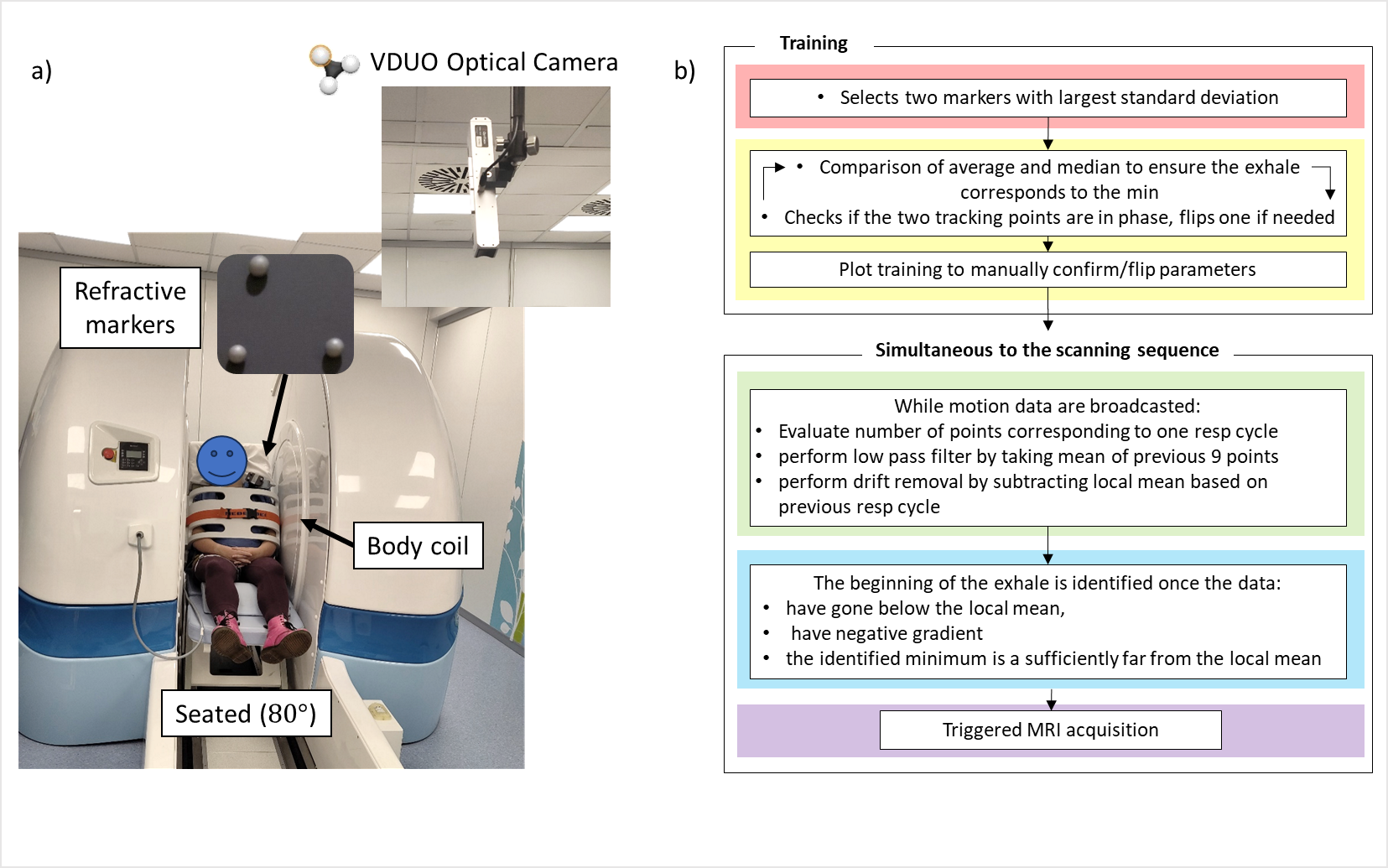
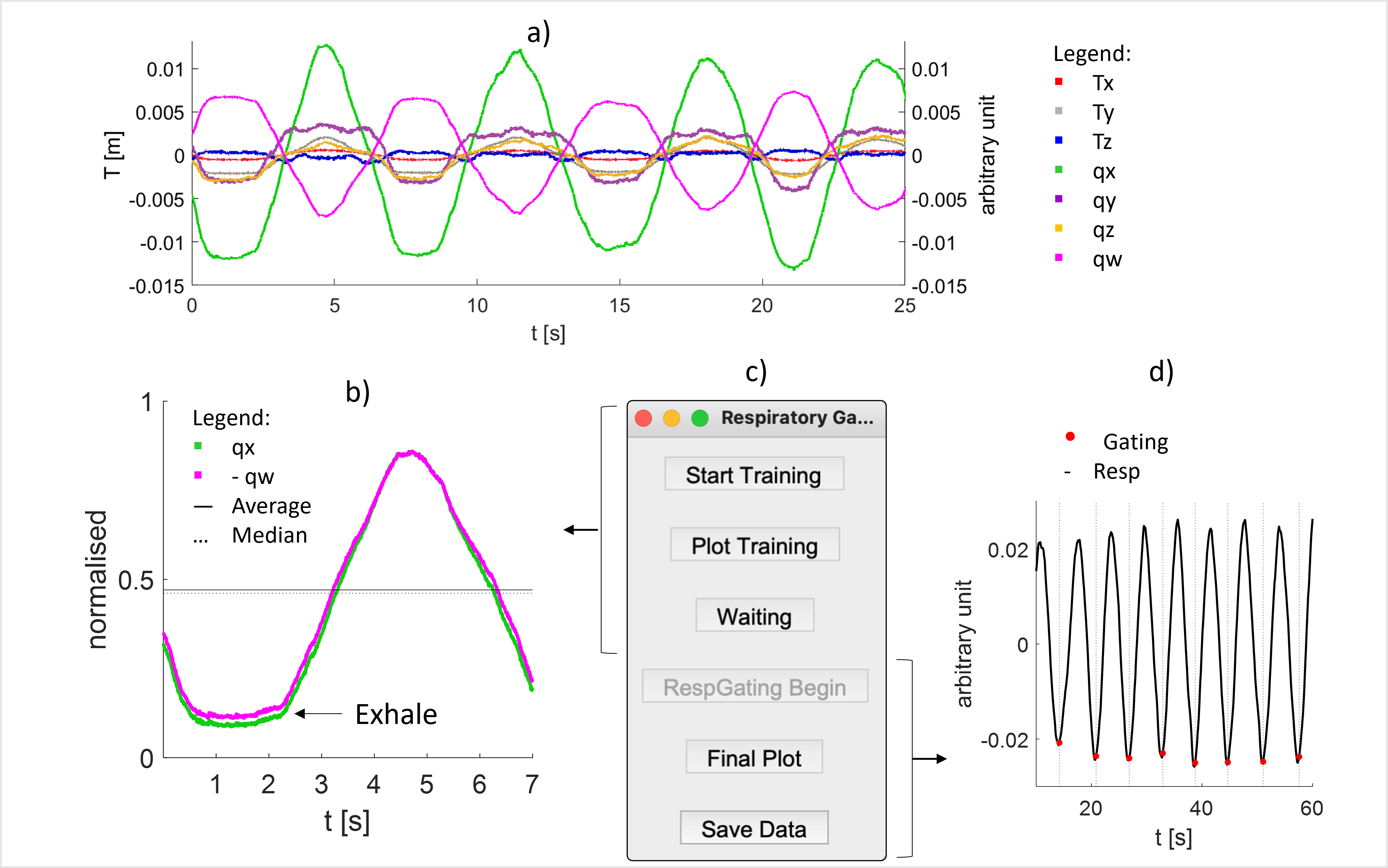
Imaging was performed in an Open 0.5T Paramed scanner. Motion in the reference system of the scanner was monitored using VDUO-Optitrack camera system.Algorithm development: 30s of motion tracking data was previously acquired from 20 subjects seated and standing in the scanner during free breathing2. This was used to develop an automatic triggering algorithm. The two motion parameters (from the 7 included in the translations and quaternion) with the largest standard deviation over two respiratory cycles were selected. These signals were normalised and superimposed, and one was inverted if they were out of phase. The mean and median were compared to determine whether the expiration plateau was near minimum. If not both signals were inverted. This signal conditioning is then checked by the scanner operator (Figure 1.b).
Motion data acquired during MRI acquisition is initially conditioned as above. After half a respiratory cycle, the start of the next exhalation was identified on smoothed and de-trended motion parameters when the data (i) dropped below the local mean over two cycles, (ii) had a negative gradient (iii) had a difference in amplitude from the local mean that is greater than the difference between the running minimum and local mean. The pipeline4 was integrated into an open access python-based GUI (Figure 2).
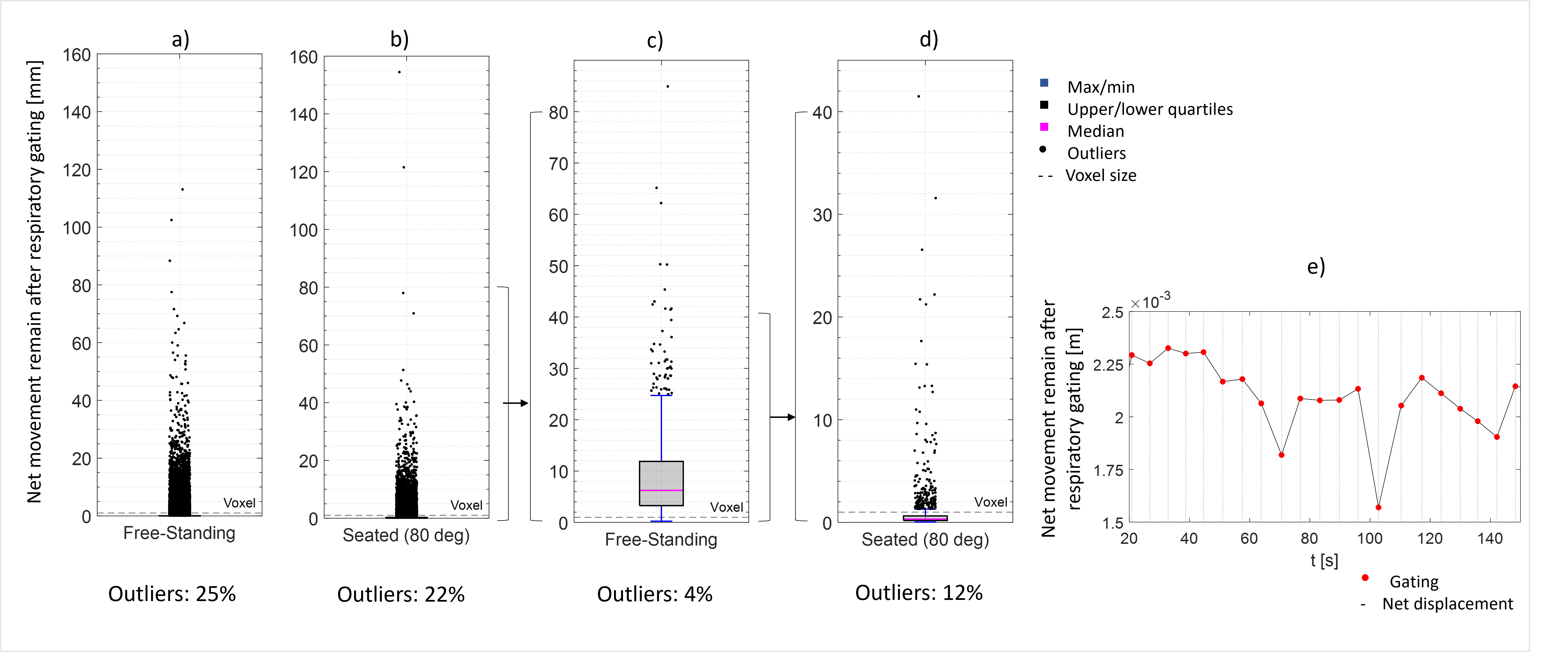
Residual motion after triggering: Nine subjects were also monitored for 10 minutes to investigate the amount of bulk movement that would remain after triggering. The pipeline was used to retrospectively trigger this motion data and the norm of the net torso displacement between trigger points was calculated (Figure3) and compared to the norm for the untriggered data.
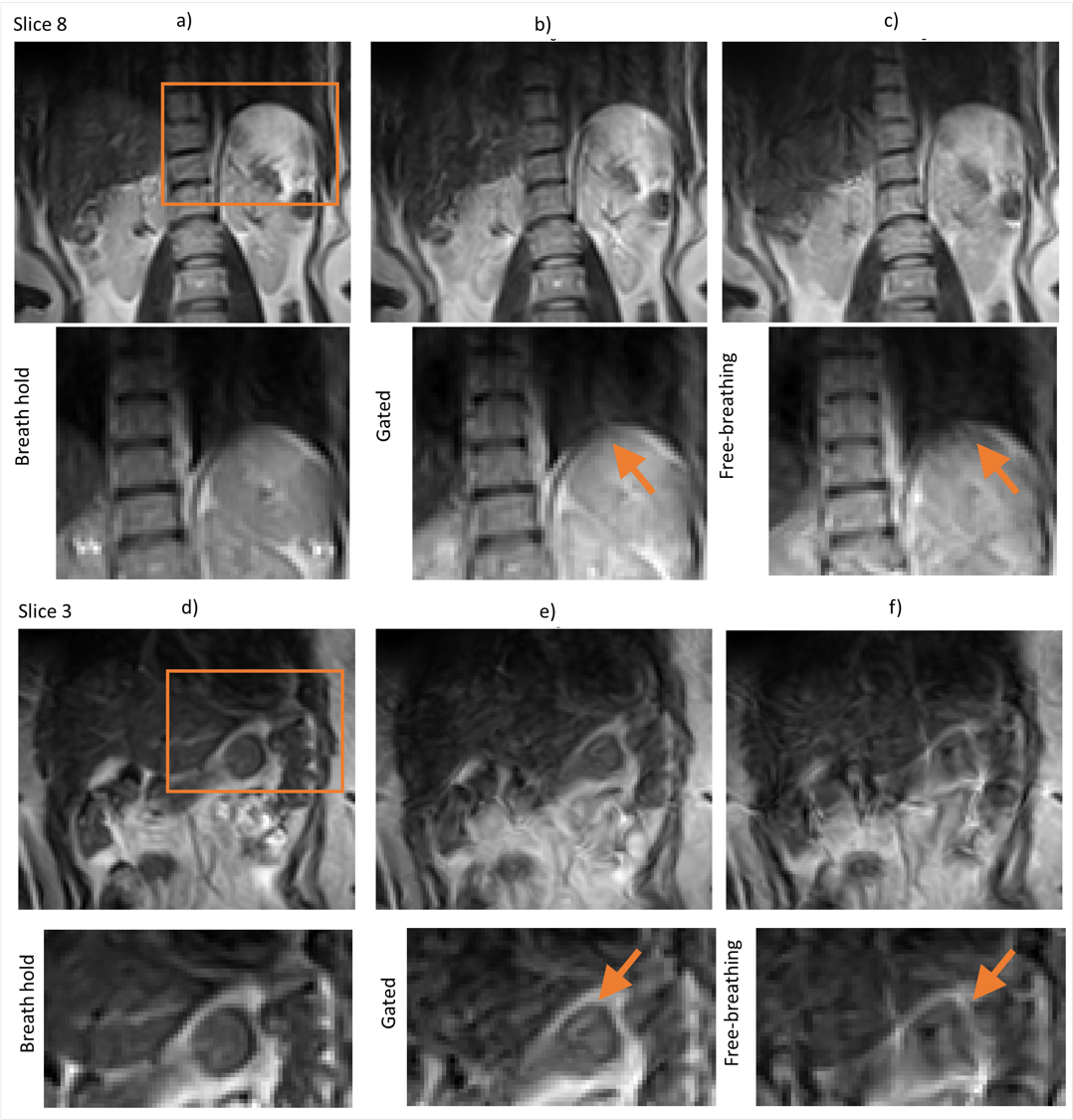
Triggered imaging: The algorithm was tested on one seated subject, reproducing a previous study2 with an improved algorithm. Gated, non-gated breath-hold and free-breathing scans of the abdomen were acquired, using a Fast-Spin echo sequence, FOV=35x35cm, 116x116 matrix, TE/TR=102ms/3192ms, TSE factor 19, echo spacing 12.9ms, 12 slices (thickness=10mm, gap=2mm). The nominal scan time was 26s plus 6s preparation; the gated scan took about 1minute to acquire. Motion was tracked using refractive markers on the left shoulder2 (Figure 1.a). The free breathing and gated images were registered to the breath-hold scan using FNIRT in FSL5, with default parameters and spline interpolation to remove bulk motion to allow better comparison.
Results
Algorithm development: Over the 10 minute data set, the exhalation points were successfully identified in the seated position in 96% of the cases averaged over all subjects, compared to 82% previously6.Residual motion after triggering: Figure 3.a-d shows the norm of the translation vector over the 10 minute data sets, for the full data set and the retrospectively triggered dataset. For standing data (Figure 3.a, Figure 3.b) motion generally exceeds the voxel size even after triggering indicating the need for full motion correction. However, for seated data (Figure 3.c, Figure3.d) the general motion was less than the voxel size, although there were more outliers which would also degrade image quality.
Triggered imaging: Figure 4 show triggered, breath-hold and free-breathing scans, Figure 3.e shows residual motion. The intra-scan motion is visible during free-breathing particularly at edges (arrows).
Discussion
The algorithm was robust when used on retrospectively acquired motion data and improved the quality of single shot FSE scans (by acquiring during the more stationary expiratory phase). Gated motion was less scattered than ungated motion as expected but the results indicate that bulk motion correction will be required for standing imaging. This system can be used for simultaneous prospective or retrospective motion correction and triggering.Conclusion
Respiratory triggering can be implemented in combination with motion monitoring and implemented in a user-friendly fashion.Acknowledgements
I’d like to thank my research group for the amazing team working done to achieve these results.References
1. Andre van der Kouwe, Jalal B. Andre, “Motion Correction in MR, Correction of Position, Motion, and Dynamic Field Changes”, 1st Edition, 2022, ISBN: 9780128244609
2. Laura Bortolotti, Isabel Clennell, Amy Bradbury, Olivier Mougin, Paul Glover, Richard Bowtell, and Penny Gowland, (2023) “Evaluation of body motion at various patient position in a 0.5 T Upright scanner”, ISMRM 2023
3. Laura Bortolotti, Olivier Mougin, Paul Glover, Richard Bowtell, and Penny Gowland, (2023) “Optical camera calibration to implement various marker-based motion correction techniques in open geometry 0.5 T upright scanner”, ISMRM 2023
4. https://github.com/LauraBortolotti/RespGating
5. FSL https://fsl.fmrib.ox.ac.uk/fsl/fslwiki/FNIRT/UserGuide
6. Bortolotti L, Clennell I, Mougin O, Glower P, Bowtell R, Gowland P, “Using Body Motion Tracking Data at Various Patient Position to Implement Respiration Gating in a 0.5 T Paramed ASG Upright Scanner” MoCo workshop Proffered Papers - Poster 4 at "ISMRM Workshop on Motion Detection & Correction"
7. BART https://mrirecon.github.io/bart/
8. Marques J P, Simonis F F, Webb A G. Low-field MRI: An MR physics perspective. J Magn Reson Imaging. 2019;49:1528-1542. https://doi.org/10.1002/jmri.26637
9. Zaitsev M, Maclaren J, Herbst M. Motion artifacts in MRI: A complex problem with many partial solutions. J Magn Reson Imaging. 2015;42(4):887-901. (https://doi.org/10.1002/jmri.24850 )
10. Safavi S, Arthofer C, Cooper A, Harkin J, Prayle A, Sovani M, Bolton C, Gowland P, Hall I. Using an upright MRI system to assess the impact of posture on diaphragm morphology. European Respiratory Journal. 2019;54(63):PA3165, DOI: 10.1183/13993003.congress-2019.PA3165
11. Cao, J.J., Wang, Y., Schapiro, W., McLaughlin, J., Cheng, J., Passick, M., Ngai, N., Marcus, P. and Reichek, N. (2011), “Effects of respiratory cycle and body position on quantitative pulmonary perfusion by MRI”. J. Magn. Reson. Imaging, 34: 225-230. https://doi.org/10.1002/jmri.22527
Figures