4646
Feasibility study of 4-dimensional free-breathing dynamic contrast-enhanced MRI for liver quantitative perfusion at 3T on oncology patients1Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China, 2Philips Healthcare, Wuhan, China
Synopsis
Keywords: Motion Correction, Liver, Perfusion
Motivation: The requirements for multiple breath-holds would cause motion artifacts, which may impair the accurate evaluation of lesion properties in dynamic perfusion scans.
Goal(s): To evaluate the clinical feasibility of free-breathing dynamic liver MR perfusion(FBP) compared with breath-holding dynamic perfusion(BHP) method.
Approach: A case-control study of 58 oncology patients were collected. The image quality, intervolume motion effect and diagnostic confidence were compared between the two groups.
Results: Four-dimensional free-breathing dynamic liver MR perfusion (4D-FBP) could provide comparable image quality but significantly fewer motions than routine method, making 4D-FBP an attractive alternative to existing breath-holding techniques in clinical dynamic liver MR scans.
Impact: Free-breathing dynamic liver MR perfusion provides significantly improved intervolume motion and comparable image quality in comparison to the routine breath-holding method, which may promote the clinical translation of liver quantitative perfusion.
Background and purpose
MR liver perfusion could provide quantitative functional information for the assessment of focal liver lesions but requires multiple breath-holds in order to avoid breathing motion artifacts, which remains problematic for the elderly and patients with difficulties with stable breath-holds, and causes confusions to accurate evaluation to lesion performances in MR liver perfusion scans. Recently a prototype free-breathing dynamic liver MR perfusion(4D-FBP) applying motion-compensated variable density radial acquisition and high-pass filtering reconstruction (1) has been reported to have great potential as an alternative to the conventional breath-holding dynamic perfusion method (BHP). But, the direct comparison with BHP has not been reported. Therefore, this study aimed to evaluate the clinical feasibility of FBP compared with BHP method, which was a Dixon-based contrast-enhanced dynamic T1WI sequence used as the routine method for liver dynamic scan.Methods
The Medical Ethics Committee of Tongji Medical College, Huazhong University of Science and Technology. Participants were informed of the MR procedures and written informed consent was obtained before contrast-enhanced liver MR perfusion examination.All examinations were performed on a 3.0T MR scanner (Ingenia 3.0, Philips Healthcare, Best, the Netherlands) with an abdominal 16-channel array coil. The detailed parameters were listed as following of 4D-FBP and BHP sequences: TR, 3.4 and 3.7ms; TE,1.36 and 1.13ms; slice thickness, 4 and 6mm; flip anlge, 15°and 10°; dynamic phases, 61 and 35; total scan time, 366 and 350 seconds; 4D-FBP with free-breathing mode, and BHP requires breath-holding. A total of 28 oncology patients (23 men, 5 women; mean age, 52.0±11.8 years) with confirmed liver malignancies were prospectively enrolled to undergo a 4D-FBP scan as a free-breathing group, and 30 oncology patients (17 men, 13 women; mean age, 56.3±10.2 years) who had clinically received routine BHP were retrospectively selected randomly as the control group. Exclusion criteria were contraindications for contrast-enhanced MRI (adverse reactions to the contrast agent, claustrophobia, pregnancy in women, severe dyspnea, continuous cough, inability to establish intravenous access, or acute or chronic severe renal impairment with eGFR<30 mL/min/1.73 m2).
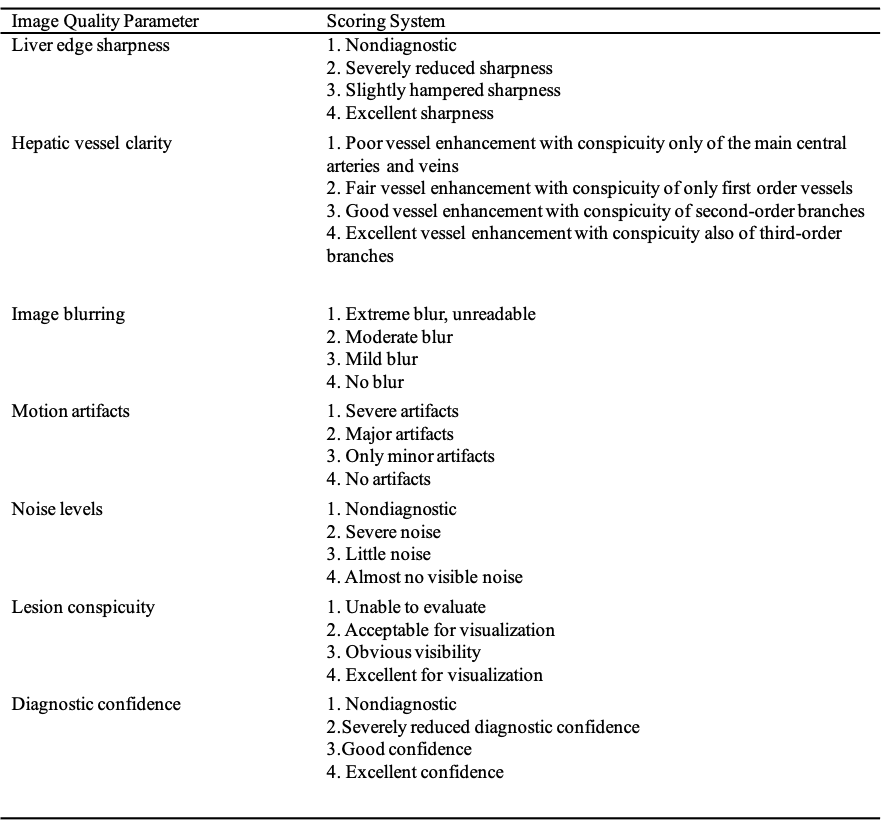
For qualitative evaluation, the image quality analysis was performed by two radiologists in consensus on a 4-point Likert scale (4= excellent,1=poor, Table 1): liver edge sharpness, hepatic vessel clarity, image blurring, motion artifacts, noise level, lesion conspicuity and diagnostic confidence(2), which based on images on 4 phases datasets (early arterial~, late arterial ~, portal venous ~ and delayed ~). The contrast-to-noise ratio (CNR) in the right lobe in the delayed phase was calculated and compared for the two groups. In addition, the intervolume motion effect for the two groups semi-quantification was calculated by using the FSL MCFLIRT tool (https://fsl.fmrib.ox.ac.uk/fsl/fslwiki/MCFLIRT), which estimated rotations and translations for each 3D volume relative to the first image in the total dynamical scan. The larger the parameters of rotation and translation, the more severe the intervolume motion. Wilcoxon signed-rank test was used for statistical analyses.
Results
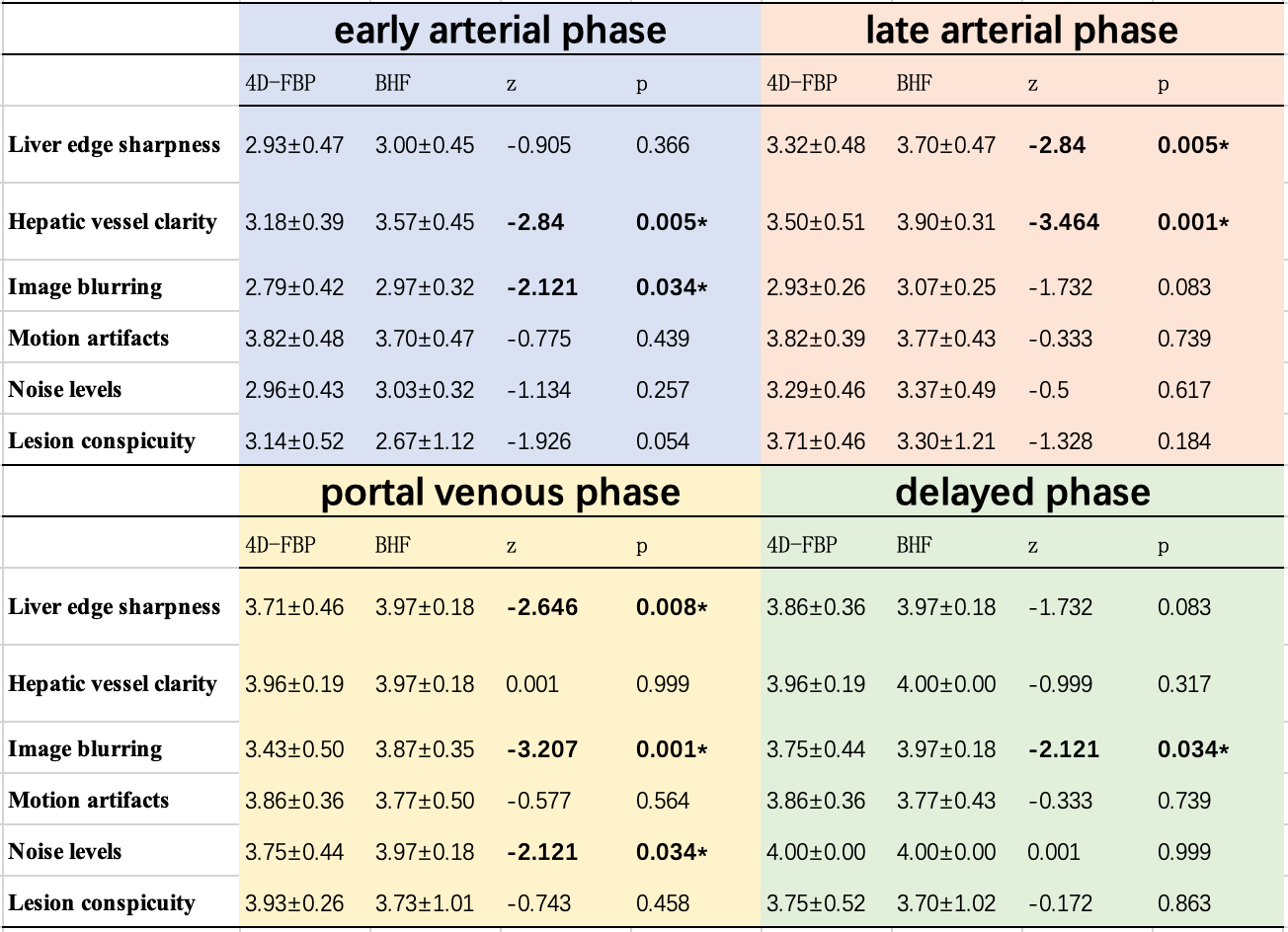
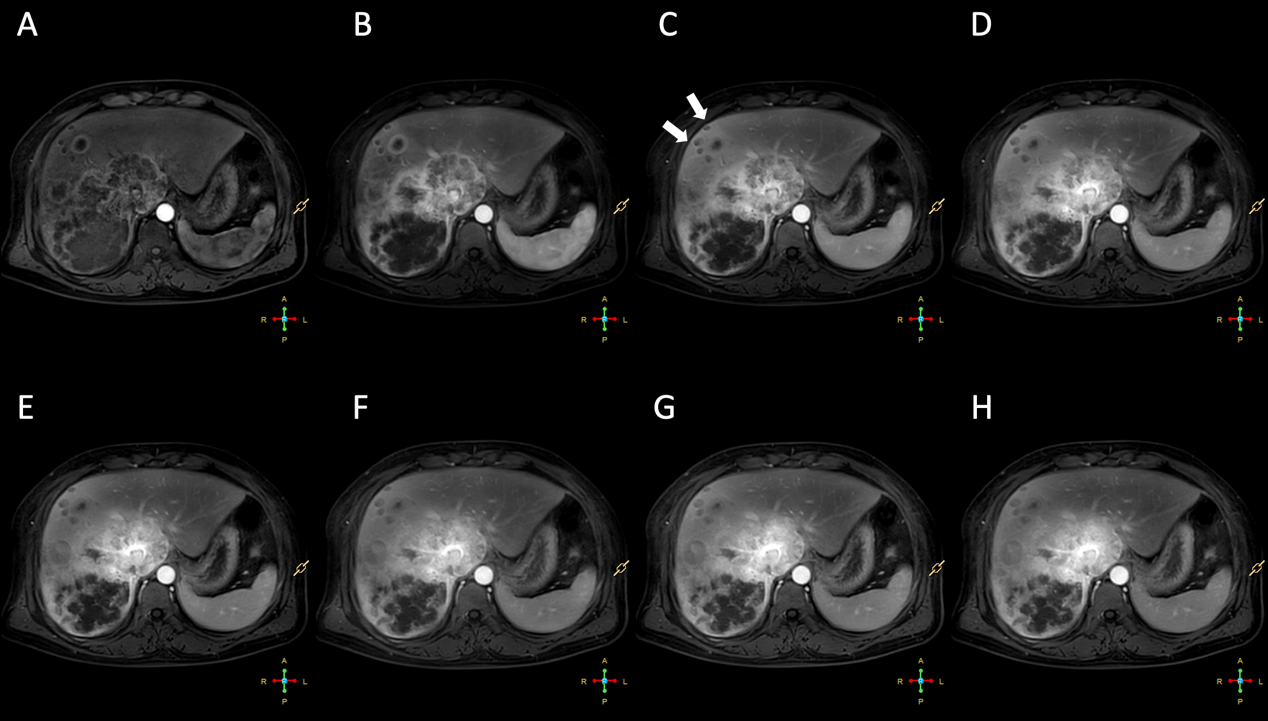
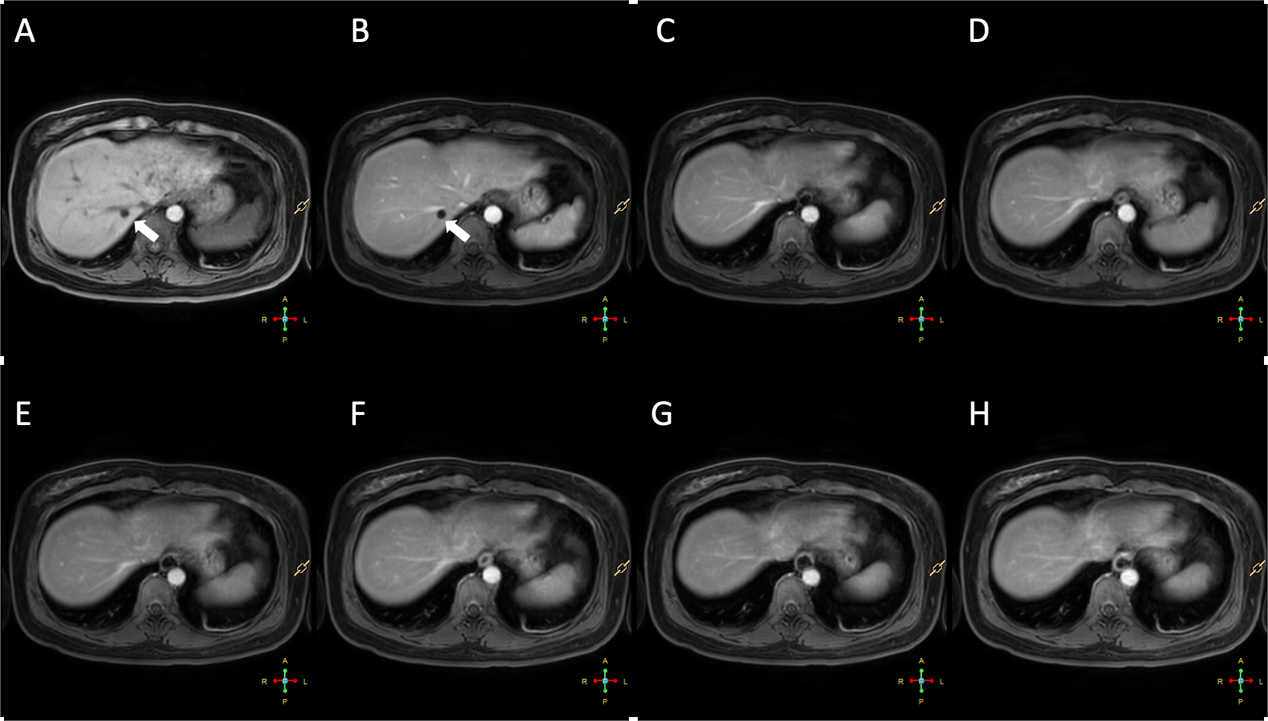
All the patients successfully finished the dynamic perfusion scans without any allergies or uncomfortable. In the 4D-FBP group, all 28 oncology patients were dignosed with malignant liver tumors, including hepatocellular carcinoma (n=23), cholangiocarcinoma (n=4) and hepatic metastatic tumor (n=1), while in the BHP group, total 30 patients were diagnosed with hepatic metastatic tumor(n=8), hepatocellular carcinoma(n=5), cholangiocarcinoma (n=3), hemangioma and cysts(n=9) and normal liver(n=5).1. Qualitative assessment: There is no significant difference in diagnostic confidence between the two groups (z=-1.242. p=0.214). As shown in Table 2, 4D-FBP method exhibited significant reductions of hepatic vascular clarity and image blurring using the 4D-FBP method in early arterial phase, liver margin sharpness and hepatic vascular clarity in late arterial phase, liver margin sharpness, image blur level, and image noise level in portal phase, and image blur level in delayed phase, respectively, when compared with BHP method. There is no significant difference in other parameters between the two groups with p>0.05.
2. Semi-quantitative assessment: 4D-FBP method displayed significant lower motion compared to BHP for rotation evaluation (0.003±0.002 vs.0.018±0.020, z=-4.122, p<0.001), and for transition (0.862±0.661 vs. 7.398±6.976, z=-4.486, p<0.001) (Figure1,2).
Conclusion
4D-FBP MRI outperforms traditional BHP MRI with greatly improved intervolume motion without the need to hold breath, which would benefit image quality with less motion artifact for liver lesions. It would be particularly useful for elderly and/or severely ill patients with impaired breath-hold capabilities liker in oncology patients and promote the clinical translation of MRI liver perfusion.Acknowledgements
We thank all participants for their help and support in our study.References
1. Endler CH-J, Kukuk GM, Peeters JM, et al. Dynamic Liver Magnetic Resonance Imaging During Free Breathing: A Feasibility Study With a Motion Compensated Variable Density Radial Acquisition and a Viewsharing High-Pass Filtering Reconstruction. Invest Radiol. 2022;57(7):470–477. doi: 10.1097/RLI.0000000000000859.
2. Afat S, Wessling D, Afat C, et al. Analysis of a Deep Learning-Based Superresolution Algorithm Tailored to Partial Fourier Gradient Echo Sequences of the Abdomen at 1.5 T: Reduction of Breath-Hold Time and Improvement of Image Quality. Invest Radiol. 2022;57(3):157–162. doi: 10.1097/RLI.0000000000000825.
Figures