4645
3D High SNR Cardiac MRI via Motion-Corrected Averaging of Multi-Heartbeat Acquisitions1Wuhan National Laboratory for Optoelectronics, Huazhong University of Science and Technology, Wuhan, China, 2Physical Sciences Platform, Sunnybrook Research Institute, University of Toronto, Toronto, ON, Canada, 3Department of Medical Biophysics, University of Toronto, Toronto, ON, Canada
Synopsis
Keywords: Motion Correction, Motion Correction
Motivation: 3D high-SNR cardiac MRI may be achieved by acquiring undersampled images with low SNR during multiple heartbeats and averaging these volumes after motion correction.
Goal(s): To generate 3D high SNR cardiac MRI from free-breathing multi-heartbeat undersampled acquisitions.
Approach: We proposed an algorithm that implemented deep-learning based undersampled image reconstruction and deformable motion correction to generate high SNR 3D MRI.
Results: For 11 subjects, our approach demonstrated effectiveness in respiratory and cardiac motion correction and generated 3D MR images with SNR 1.7x higher than single heartbeat acquisition and 1.4x higher than that without motion correction.
Impact: The proposed approach provides a way for respiratory and cardiac motion correction and enables 3D MRI with high SNR that is required for a wide range of clinical applications.
INTRODUCTION
3D high SNR imaging is vital for various applications of cardiac MRI (CMR) for management of cardiovascular disease. However, rapid acquisition of 3D CMR is challenging due to respiratory and cardiac motion. These issues may be addressed by repeatedly acquired undersampled data in multiple heartbeats during free-breathing. Reconstruction of undersampled 3D images and correction for respiratory and cardiac motion are required as a first step. In this study, we proposed an approach for motion-corrected averaging for 3D high SNR CMR through segmented free-breathing 3D acquisition, building on related work by Kellman and colleagues1.METHODS
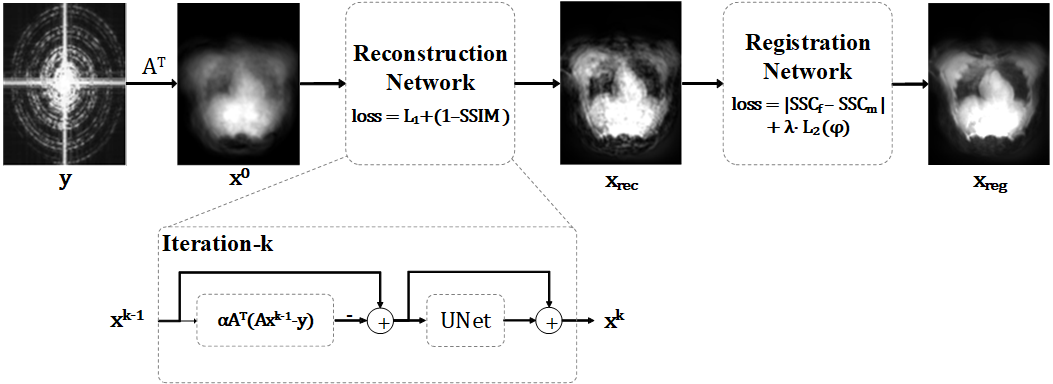
Subjects and MRI: Eleven healthy volunteers were enrolled in this study. MRI was performed at 1.5T (MR450w, GE Healthcare, USA) using a 32-channel coil array. Free-breathing 3D cones images were acquired with an undersampling factor of 12 for each heartbeat for approximately two minutes2; data from the first 20 heartbeats were used here. For each subject, all the k-space data was used for coil sensitivity map estimation, which was performed as part of the l1-ESPIRiT algorithm to reconstruct "ground-truth" (GT) images for each heartbeat3,4. The 11 subjects were randomly divided into three groups of 4, 4, and 3 subjects each with 20 images for three-fold cross validation5.Deep learning-based 3D CMR reconstruction and cardiac motion correction: Figure 1 shows the proposed algorithm for 3D high SNR cardiac imaging via a multi-heartbeat acquisition. This approach consists of 3D undersampled image reconstruction, deformable motion correction (MoCo), and averaging. Here, we employed an unrolled deep-learning (DL) network6 that implemented gradient descent as in conventional MR reconstruction algorithms and U-net based regularization. A combination of L1 loss and structural similarity index metric (SSIM) loss was used for network training.
The reconstructed images were carried to a registration network for deformable motion correction (MoCo) by registering the moving images from the 2nd to the 20th heartbeats to the fixed image in the first heartbeat7. Self-similarity context (SSC) was calculated for the input images and entered the registration network to estimate the diffeomorphic deformation field8,9. L1 norm of the differences in SSC for the fixed and warped moving images was used as the training loss. The fixed image and the warped moving images were averaged to generate the final fusion image, dubbed motion-corrected average (MoCo-avg). In addition, the DL-reconstructed images were directly averaged without motion-correction (non-MoCo-avg) to isolate the effect of MoCo for high SNR imaging.
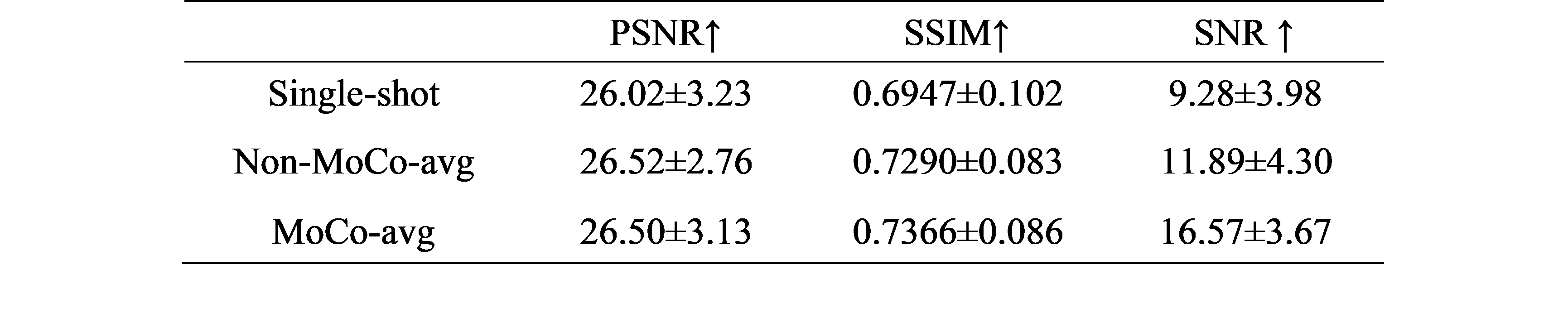
Evaluation metrics: Registration performance was evaluated using PSNR and SSIM between the fixed and moving images pre- and post-MoCo. The quality of the images generated by MoCo-avg, non-MoCo-avg, and undersampled DL reconstruction of the first heartbeat (single-shot) was determined using SNR and PSNR with respect to the GT from the first heartbeat.
RESULTS
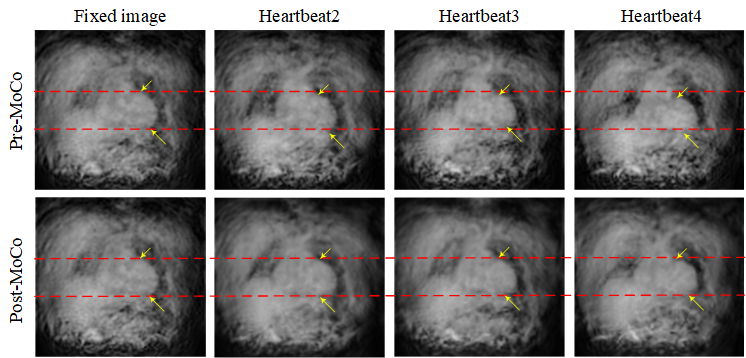
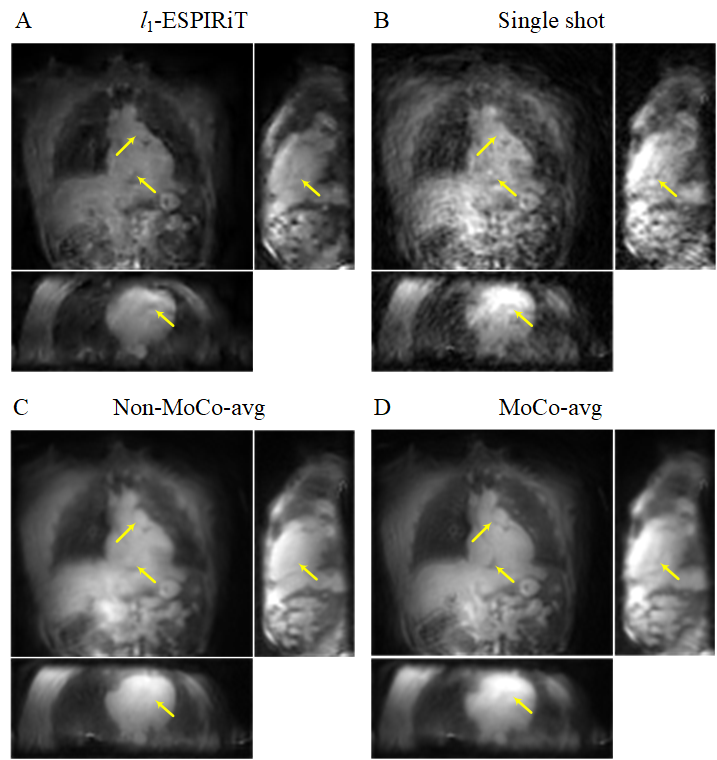
Figure 2 shows that the registration module improved the alignment of the three moving images and the fixed image. As shown in Table 1, MoCo required 23 ms to register a pair of images, and yielded substantially improved PSNR of 33.01±2.9, SSIM of 0.8506±0.0506 with 0.0252% folding of the deformation field for the three-fold validation. Figure 3 depicts the GT, single-shot, and fused images provided by non-MoCo-avg and MoCo-avg. Table 2 shows that MoCo-avg yielded a mean SNR of 16.57, substantially greater than single-shot (SNR=9.28) and non-MoCo-avg (SNR=11.89). The PSNR and SSIM were somewhat similar for the three methods.DISCUSSION
The substantial improvements in PSNR and SSIM between the fixed and moving images pre- and post- motion correction suggest the effectiveness of the registration module in correcting the non-rigid respiratory motion between heartbeats. Compared with single-shot imaging, MoCo-avg yielded 1.8x higher SNR, which is lower than the theoretical factor of 4.5 by averaging the 20 registered images. This may stem from the redundancy in information between individual heartbeats introduced in the DL reconstruction. The similarity in PSNR and SSIM for single-shot, non-MoCo-avg, and MoCo-avg may be caused by the sub-optimal quality of the GT from the first heartbeat.CONCLUSIONS
The proposed approach is effective in correcting the physiological motion between highly undersampled MR images from different heartbeats and provides a way to generate 3D MR images with high SNR that is required for a wide range of clinical applications.Acknowledgements
Calder D. Sheagren, Jaykumar H. Patel, and Graham A. Wright acknowledge research grants from Canadian Institutes of Health Research, GE Healthcare and Vista AI as well as non-monetary research support from Siemens Healthineers.References
1. P Kellman, A C Larson, L Y Hsu, et al. Motion‐corrected free‐breathing delayed enhancement imaging of myocardial infarction. Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine. 2005;53(1):194-200.2. N O Addy, R R Ingle, H H Wu, et al. High‐resolution variable‐density 3D cones coronary MRA. Magnetic resonance in medicine. 2015;74(3):614-621.
3. M Uecker, P Lai, M J Murphy, et al. ESPIRiT—an eigenvalue approach to autocalibrating parallel MRI: where SENSE meets GRAPPA. Magnetic resonance in medicine. 2014;71(3):990-1001.
4. M Uecker, F Ong, J I Tamir, et al. Berkeley advanced reconstruction toolbox. Proc. Intl. Soc. Mag. Reson. Med. 2015;23(2486).
5. D M Hawkins, S C BasakD Mills. Assessing model fit by cross-validation. Journal of chemical information and computer sciences. 2003;43(2):579-586.
6. M O Malavé, C A Baron, S P Koundinyan, et al. Reconstruction of undersampled 3D non‐Cartesian image‐based navigators for coronary MRA using an unrolled deep learning model. Magnetic resonance in medicine. 2020;84(2):800-812.
7. G Balakrishnan, A Zhao, M R Sabuncu, et al. VoxelMorph: A Learning Framework for Deformable Medical Image Registration. IEEE Trans Med Imaging. 2019;38(8):1788-1800.
8. M P Heinrich, M Jenkinson, B W Papież, et al. Towards realtime multimodal fusion for image-guided interventions using self-similarities. Medical Image Computing and Computer-Assisted Intervention–MICCAI 2013: 16th International Conference, Nagoya, Japan, September 22-26, 2013, Proceedings, Part I 16. 2013;187-194.
9. A V Dalca, G Balakrishnan, J Guttag, et al. Unsupervised learning of probabilistic diffeomorphic registration for images and surfaces. Medical image analysis. 2019;57:226-236.
Figures