4640
MR SIGNATURE MATCHING (MRSIGMA) WITH ADAPTIVE MOTION LEARNING FOR ROBUST REAL-TIME 4D MRI ON A 1.5T MR-LINAC1Medical Physics, Memorial Sloan Kettering Cancer Center, New York, NY, United States, 2Radiology, Memorial Sloan Kettering Cancer Center, New York, NY, United States
Synopsis
Keywords: Motion Correction, Radiotherapy
Motivation: Real-time 4D MRI on the MR-Linac is still sensitive to respiratory motion baseline drifts.
Goal(s): To further develop MRSIGMA for real-time adaptation to out-of-range anatomical changes during signature matching.
Approach: The motion dictionary was continuously updated using a sliding window of stack-of-stars data and fast motion-resolved Movienet reconstruction. MRSIGMA with adaptive motion learning was implemented in real-time using an external computer connected to the MR-Linac and tested on a programmable 4D phantom and a patient with pancreatic cancer.
Results: The adaptive motion learning approach was able to update the dictionary after 2 sliding window periods, which improved robustness of real-time volumetric motion tracking.
Impact: MRSIGMA with adaptive learning would enable real-time volumetric motion tracking robust to respiratory motion baseline drifts and other anatomical changes on the MR-Linac for improved monitoring and adaptation of radiotherapy of tumors affected by respiratory motion.
INTRODUCTION
MR Signature Matching (MRSIGMA) enables real-time 4D MRI with a total imaging latency below 300ms to monitor and adapt radiotherapy of tumors affected by respiratory motion on a MR-Linac system[1, 2, 3]. MRSIGMA first learns a motion dictionary with motion images and signatures, and then uses the dictionary to perform fast signature-only acquisition and matching to minimize latency. However, respiratory motion baseline drifts or other anatomical changes outside motion learning range result in matching errors or unmatched signatures[4, 5]. This work develops a new version of MRSIGMA, to continuously adapt the motion dictionary during signature matching. Adaptive MRSIGMA technique is tested on a programmable 4D phantom and a patient with pancreatic cancer.METHODS
Adaptive motion learning: Data acquisition was performed using a T1-weighted 3D stack-of-stars k-space acquisition with partial-Fourier along kz, and SPIR fat suppression. Conventional motion learning step was performed with 1,344 golden angles and scan time of 3:45mins. To adapt the dictionary, a sliding window of 1,344 angles was used to concatenate the last 1,264 angles and 80 newly acquired angles (Figure 1). For each dataset of 1,344 angles, a motion signal was estimated using PCA of z-projections obtained after applying an inverse FFT to central kx-ky position and sum-of-squares coil combination. The amplitude of respiratory motion signal was binned into motion states and the acquired data were sorted accordingly. To maximize reconstruction speed, the deep learning 4D reconstruction technique Movienet[6] was employed.Adaptive signature matching: After each angle was acquired, motion signature was computed by applying an inverse FFT to central kx-ky position and sum-of-squares coil combination to form a z-projection. The 3D motion state in the motion dictionary whose signature presents highest correlation with the new signature is selected as output. Signature matching was performed using the updated motion dictionary.
Real-time implementation: Raw data were sent to an external computer with 2 NVIDIA A-40 GPU cards connected to the same network as MR-Linac. Adaptive motion learning and signature matching were performed in parallel.
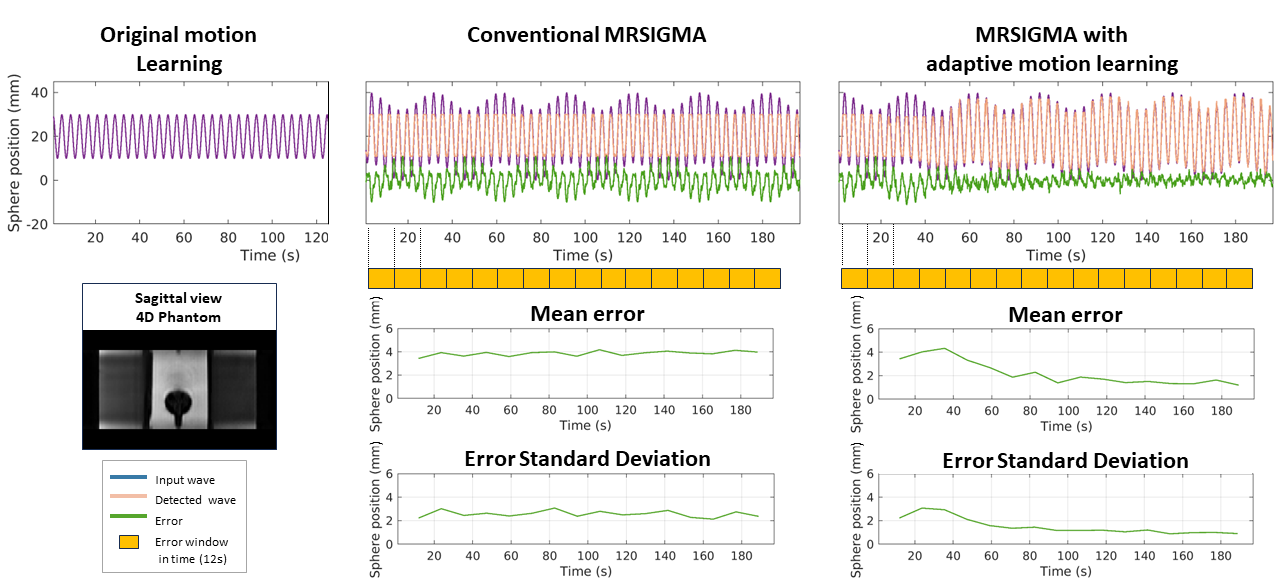
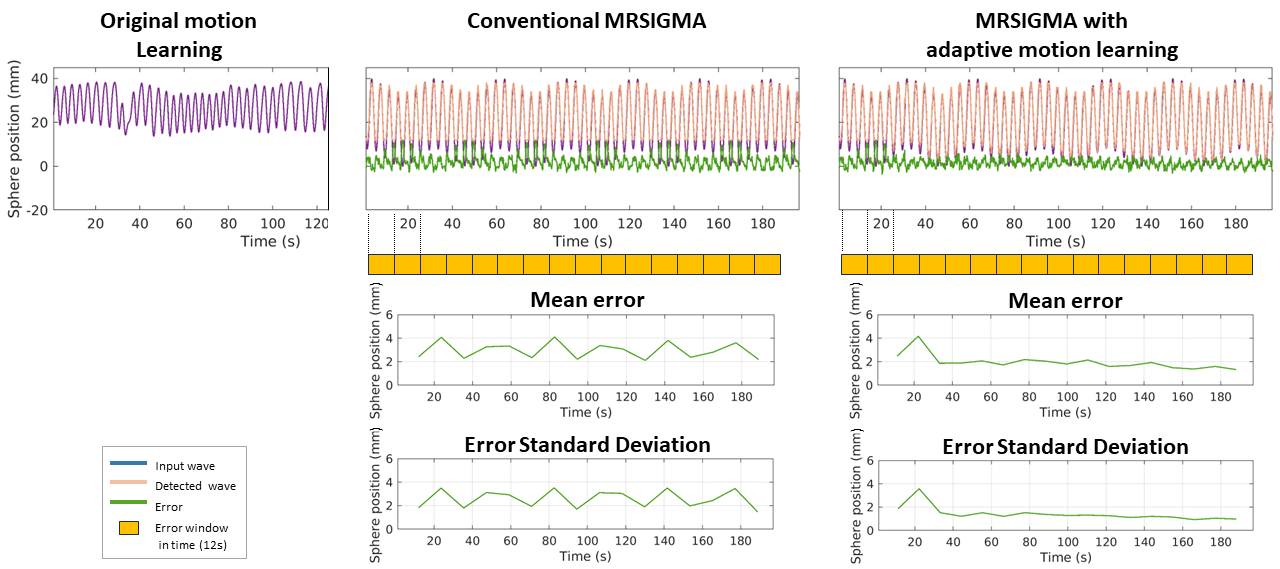
4D Phantom experiments: A programmable 4D phantom (Quasar) with different input motion for motion learning and signature matching was employed. Data acquisition was performed with 2mm isotropic resolution. First experiment used a sinusoidal input motion with 20mm amplitude for motion learning and a sum of two sinusoidal functions with 40mm amplitude and different frequencies to include a baseline drift of 10mm every 30 seconds for signature matching. Second experiment used a patient respiratory motion signal as input for motion learning and the sum of two sinusoids for signature matching. The patient motion signal range was 15-40mm, so adaptive version of MRSIGMA would have to cover the lower 0-15mm motion range. The central position of the moving sphere was used to track phantom motion. Mean value and standard deviation of the error between the input motion and estimated phantom motion were computed for each update period of 80 time points (adaptation window).
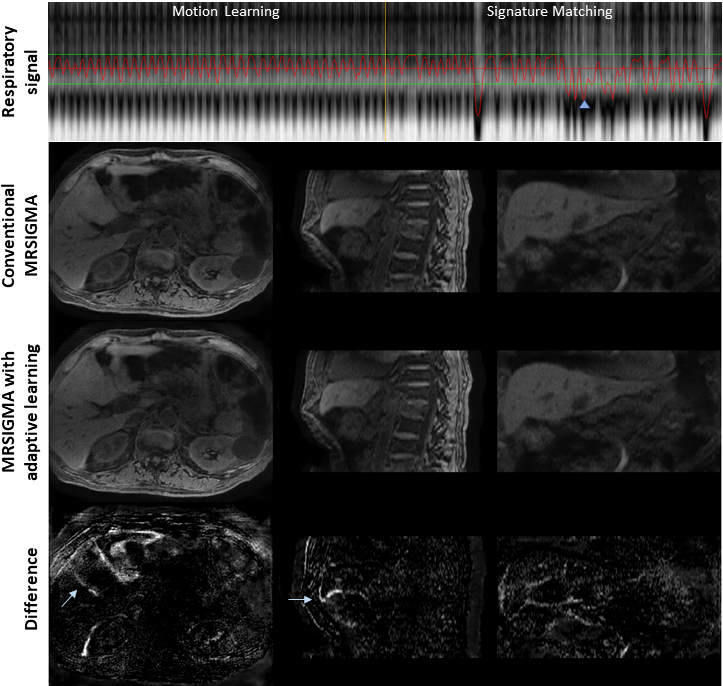
In-vivo experiment: MRSIGMA adaptive motion learning was compared against conventional MRSIGMA on a patient with pancreatic cancer. Free-breathing acquisition was performed with a resolution of 1.5x1.5x4mm and real-time images at a time point with a displacement outside the learned motion were evaluated.
RESULTS
The total imaging latency of MRSIGMA was less than 200ms. The total time to adapt the dictionary was about 20 seconds, including 13 seconds for acquisition of 80 angles, 3-4 seconds of motion signal estimation and data sorting, and 3-4 seconds of Movienet reconstruction. MRSIGMA with adaptive learning improved the results of original MRSIGMA and was able to adapt to new motion patterns in phantom with an error of 3±2mm in first experiment and 1.9±1.5mm in second experiment (Figure 2-3). The adaptive learning approach was also able to adapt to in-vivo changes not covered during initial motion learning period. Figure 4 shows an example of adaptation to a more inspiratory position of the liver.DISCUSSION
Flexibility of the golden-angle radial acquisition to sort data in a quasi-arbitrary way and fast deep learning motion-resolved reconstruction using Movienet enabled to continuously adapt the motion dictionary in real-time during signature matching. Future work will be focused on improving acquisition and computational performance of adaptation approach to reduce the time to compute the new motion dictionary.CONCLUSION
MRSIGMA with adaptive motion learning allows continuous adaptation of the motion dictionary every 20 seconds to consider potential changes during signature matching such as respiratory motion drifts. This work is a step forward to real-time monitoring and adaptation of radiotherapy using a MR-Linac system in organs affected by respiratory motion.Acknowledgements
The work was supported by NIH Grant R01CA255661.References
1. Feng, L., N. Tyagi, and R.J.M.r.i.m. Otazo, MRSIGMA: Magnetic Resonance SIGnature MAtching for real‐time volumetric imaging. 2020. 84(3): p. 1280-1292.
2. Kim, N., et al., MR SIGnature MAtching (MRSIGMA) with retrospective self-evaluation for real-time volumetric motion imaging. 2021. 66(21): p. 215009.
3. Wu, C., et al., Real-time 4D MRI using MR signature matching (MRSIGMA) on a 1.5 T MR-Linac system. 2023. 68(18): p. 185015.
4. Quirk, S., N. Becker, and W.J.J.o.A.C.M.P. Smith, External respiratory motion analysis and statistics for patients and volunteers. 2013. 14(2): p. 90-101.
5. Yasue, K., et al., Quantitative analysis of the intra-beam respiratory motion with baseline drift for respiratory-gating lung stereotactic body radiation therapy. 2022. 63(1): p. 137-147.
6. Murray, V., et al., Movienet: Deep space–time‐coil reconstruction network without k‐space data consistency for fast motion‐resolved 4D MRI. 2023.
Figures
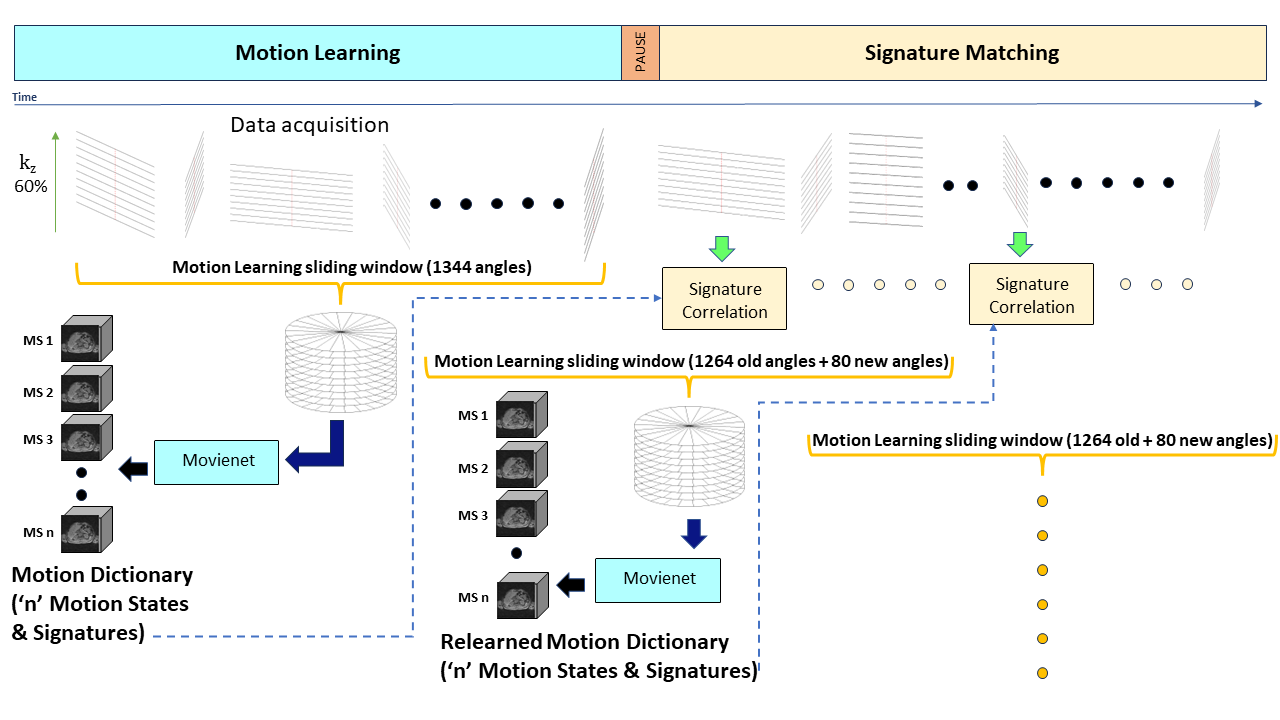
Figure 1: MRSIGMA with adaptive motion learning. Instead of computing the motion dictionary only once before signature matching, the motion dictionary was continuously updated during signature matching for every 80 time points (or angles) to adapt for respiratory motion baseline drifts and other anatomical changes during signature matching. A motion learning sliding window of 1,344 angles of stack-of-stars acquisition was reconstructed using deep learning-based Movienet to generate the motion dictionary in parallel to signature matching.