4636
Diffusion-weighted MRI-based Virtual Elastography for the Assessment of Liver Fibrosis1Lanzhou University Second Hospital, Lanzhou, China, 2Siemens Healthcare, Shanghai, China
Synopsis
Keywords: Liver, Diffusion/other diffusion imaging techniques
Motivation: Liver biopsy is considered the reference standard for liver fibrosis quantification, however, noninvasive techniques are the emerging focus in this field. Elasticity values based on Diffusion-weighted (DW) MRI–based virtual elastography has been confirmed of a highly correlation with MR elastography.
Goal(s): Assess the usefulness of DW MRI-based virtual MR elastography in the evaluation of fibrosis.
Approach: We compared the diagnostic performance of elasticity values based on virtual MR elastography(μDiff), US elastography (Fibroscan) and serum markers for identifying significant liver fibrosis.
Results: μDiff were significantly different between non-significant and significant fibrosis, and slightly accurate than Fibroscan for depiction of significant fibrosis.
Impact: Diffusion-weighted MRI–based virtual elastography was confirmed with good agreement with shear modulus measured at MR elastography. Our study found that virtual modulus were significantly different between non-significant and significant liver fibrosis and appeared to preoperative prediction of liver fibrosis.
Introduction and purpose
Liver fibrosis (LF) was viewed as a reversible process if optimal management is started timely. While liver biopsy is the gold standard for assessing LF, it has limitations, including sampling errors, the risk of complications due to its invasiveness. Some studies showed MR elastography was as accurate as liver biopsy for noninvasive LF staging, however, the method is costly and requires complex mechanical setup. Recently, a Diffusion-weighted (DW) MRI–based virtual elastography model at 3.0T was proposed can be converted quantitatively into shear modulus for noninvasive liver staging, and Diffusion-based shear modulus shows good agreement with shear modulus measured at MR elastography. However, the main limitation of the study was the lack of pathologic validation[1,2]. Thus, the purpose of our study was to validate this DW MRI at 1.5T approach to evaluate the diagnostic performance for fibrosis staging. Ultrasound elastography (FibroScan) and serum fibrosis markers were also assessed.Materials and Methods
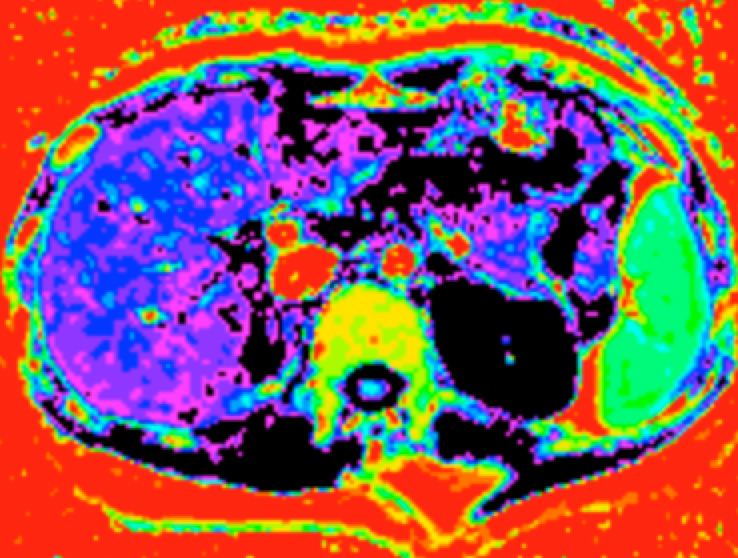
Forty-five participants underwent DWI using twelve b values (0, 50, 100, 150, 200, 400, 600, 800, 1000, 1200, 1500, 2000 s/mm2) at 1.5 T magnetic resonance (Aera, Siemens Healthcare, Erlangen, Germany). DWI was acquired using a single-shot echo-planar imaging sequence in the axial orientation. The detailed parameters were as follows: TR/TE =6800/58ms, FOV=304×380mm2, scan matrix=108×134, slice thickness=6mm. Shifted apparent diffusion coefficient (sADC) was calculated from DWI and converted to DWI–based virtual shear modulus (μDiff) (Figure 1). The sADC was calculated as follows: sADC (mm2 /sec)= ln(S200/S1500 ) /1300, S200 is the DWI signal with b value of 200 sec/mm2, and S1500 is the DWI signal with a b value of 1500 sec/mm2. μDiff was then calculated as follows: μDiff (kPa)=αsADC(mm2/sec)+β. The values for α and β were -12740 and 14.0 respectively[1,2]. Shear modulus measured by μDiff was obtained in each patient from regions of interest (ROI). ROIs were manually drawn to include only the liver parenchyma on each axial image in right lobe of the DWI–based virtual shear modulus map, by excluding visible vessels, focal lesions and artifacts. The degree of fibrosis was assessed according to the Scheuer scoring systems. Based on their fibrosis stage, all participants were reclassified as non-significant LF (S0-1) and significant LF (≥S2). The Kruskal–Wallis test evaluated the distribution of μDiff, Fibroscan, APRI, and FIB-4 among the LF stages. μDiff and Fibroscan. Receiver operating characteristic (ROC) curve analysis was used to assess the discriminative capacities of DWI–based virtual shear modulus, Fibroscan and serum markers for identifying significant LF. Areas under the ROC curve (AUCs) were compared using the DeLong test.Results
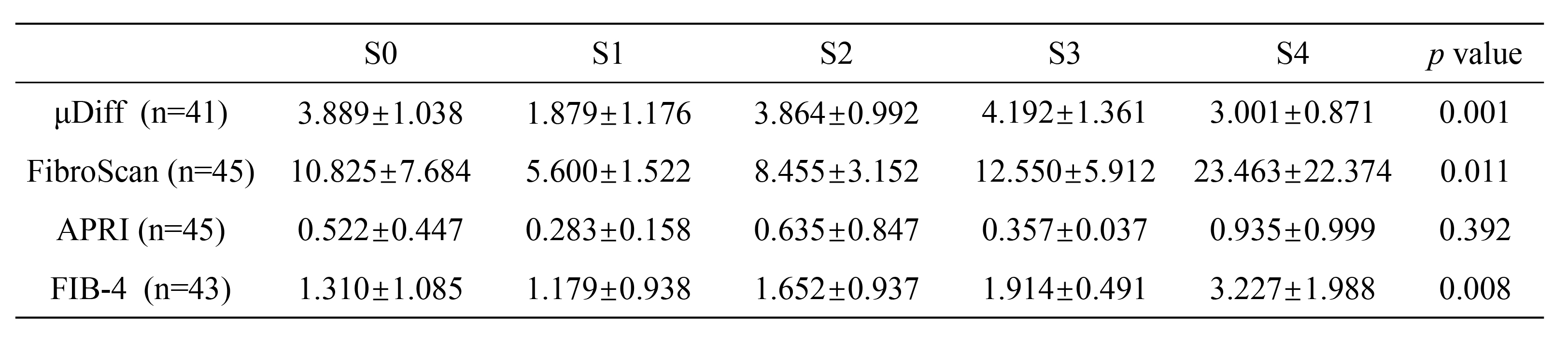
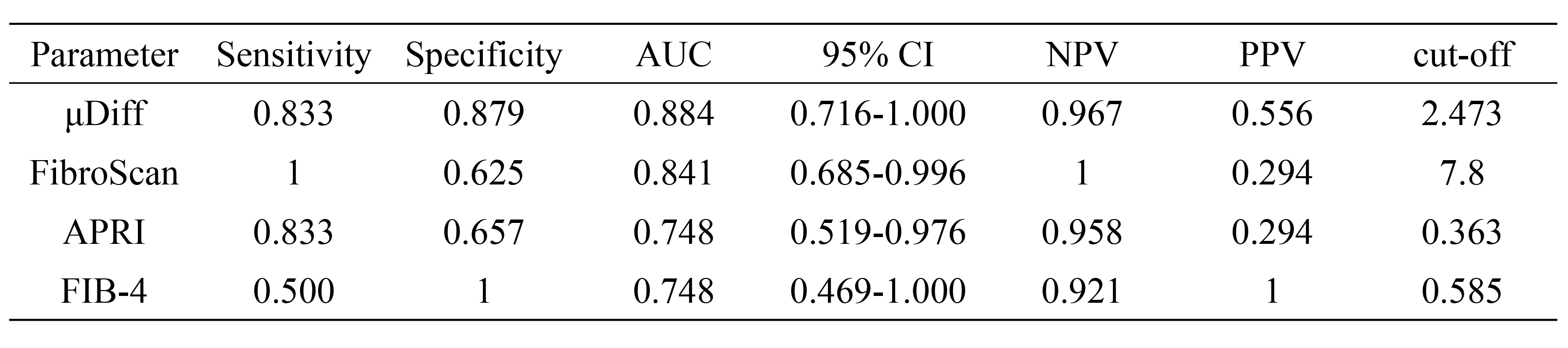
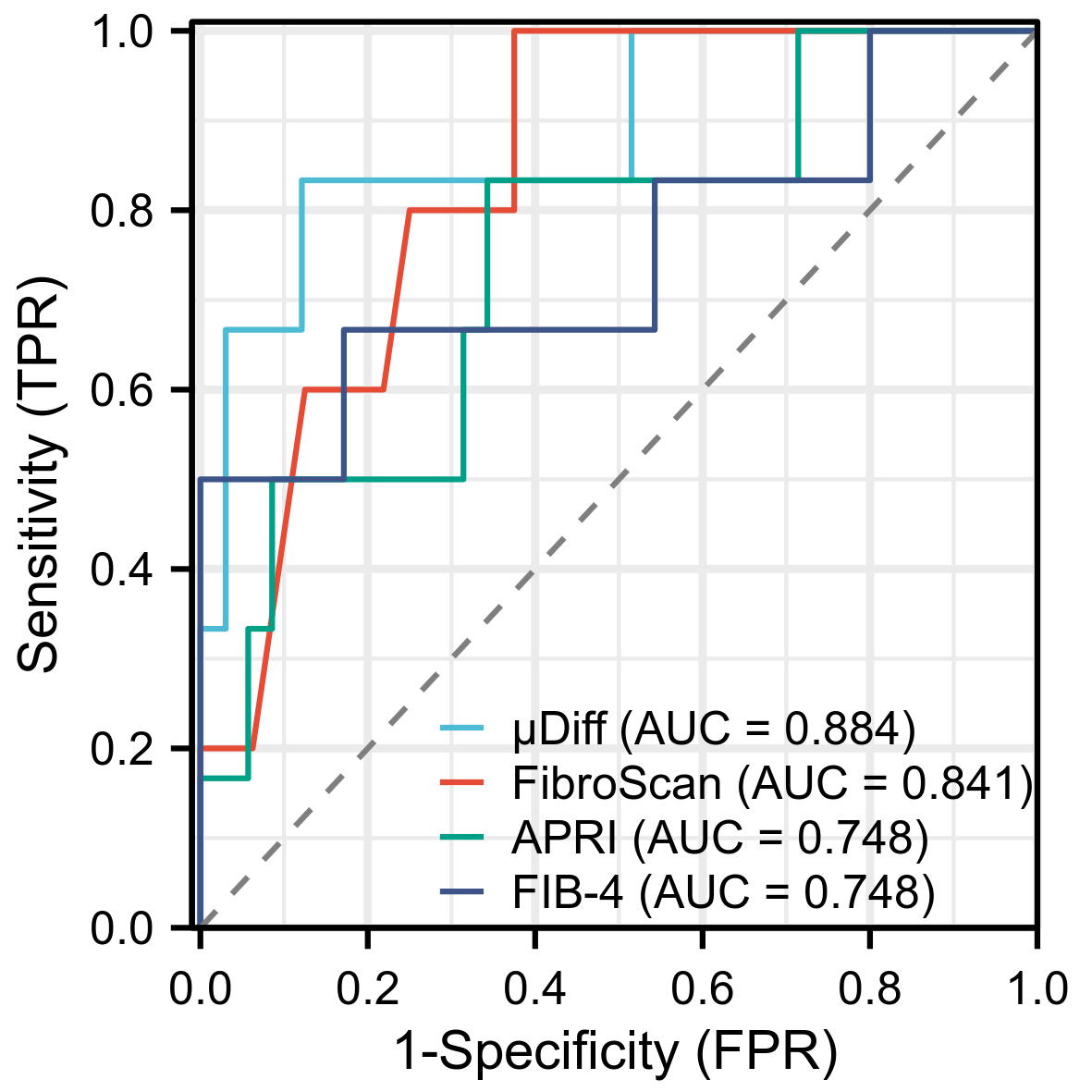
The μDiff, Fibroscan, APRI, and FIB-4 distributions for the patients in the various fibrosis stages are shown in Table 1. DWI–based virtual shear modulus showed no correlation with Fibroscan. The best cutoffs to discriminate between non-significant LF (S0-1) and significant LF (≥S2), were μDiff (2.473 kPa), FibroScan (7.8 kPa), APRI (0.363), FIB-4 (0.585). For the differentiation between non-significant and significant LF, DWI–based virtual shear modulus (AUC 0.884) showed slightly better results with AUCs as follows: Fibroscan, 0.841 (p =0.71); APRI, 0.748 (p =0.35) and FIB-4, 0.748 (p =0.41). The corresponding AUCs, sensitivity, and specificity are detailed in Table 2. Comparison of ROC curves are shown in Figure 2.Discussion
We assessed the efficacy of DW MRI–based virtual elastography at 1.5T for the evaluation of the severity of LF. In our study, we found that the DW MRI–based virtual shear modulus performed well in the diagnosis of patients with significant LF, indicates that the use of higher b values increases sensitivity to non-Gaussian diffusion and, hence, effects of tissue microstructure, and tissue water diffusivity and tissue elasticity has strong correlation [3,4]. However, DWI–based virtual shear modulus showed no correlation with Fibroscan and was no difference in different stages of LF in our study. It is possible that shear modulus may not be in the same location in the liver as the FibroScan and liver biopsy, due to the fact that the shear modulus measured by μDiff in our study was measured locally as a single axial slice. In addition, the uneven distribution of participants with different stages of fibrosis will potential bias the results. Further studies with large clinical trials are recommended to confirm the superiority of DW MRI-based virtual elastography in the assessment of liver fibrosis.Conclusion
In conclusion, the estimation of the DW MRI-based virtual elastography shows potential noninvasive tool for evaluation of liver fibrosis without the need for any mechanical vibration.Acknowledgements
No acknowledgement found.References
[1] Le Bihan D, Ichikawa S, Motosugi U. Diffusion and Intravoxel Incoherent Mo- tion MR Imaging-based Virtual Elastography: A Hypothesis-generating Study in the Liver. Radiology 2017;285(2):609–619.
[2] Kromrey ML, Le Bihan D, Ichikawa S, Motosugi U. Diffusion-weighted MRI-based Virtual Elastography for the Assessment of Liver Fibrosis. Radiology. 2020;295(1):127-135.
[3] Obara M, Kwon J, Yoneyama M, Ueda Y, Cauteren MV. Technical Advancements in Abdominal Diffusion-weighted Imaging. Magn Reson Med Sci. 2023;22(2):191-208.
[4] Ota T, Hori M, Le Bihan D, Fukui H, Onishi H, Nakamoto A, Tsuboyama T, Tatsumi M, Ogawa K, Tomiyama N. Diffusion-Based Virtual MR Elastography of the Liver: Can It Be Extended beyond Liver Fibrosis? J Clin Med. 2021;10(19):4553.
Figures