4628
Identification of Early-stage Renal Abnormalities by Magnetic Resonance Imaging in Chronic Heart Failure Patients: A Preliminary Study1China-Japan Union Hospital of Jilin University, Changchun, China, 2MR Research Collaboration, Siemens Healthineers, Beijing, China, 3MR Application Predevelopment, Siemens Healthineers AG, Erlangen, Germany
Synopsis
Keywords: Kidney, Kidney
Motivation: The prevalence of impaired renal function is high in chronic heart failure (HF). However, renal abnormalities are faced with difficulties in early diagnosis.
Goal(s): Identification of preclinical pathophysiological changes of kidney by multiparametric MRI in chronic HF patients.
Approach: Chronic HF with eGFR>60 ml/min/1.73 m2 and healthy volunteers underwent multiparametric MRI. RBF, T1 relaxation time, T2 relaxation time, R2*, and ADC values of renal cortex were measured and compared between the patients and controls.
Results: Chronic HF group demonstrated higher R2* values (p=0.043) and lower RBF values (p<0.01) than control group. The other three parameter values showed no statistically significant difference between groups.
Impact: In this preliminary study, we revealed that even with preserved estimated glomerular filtration rate (eGFR), patients with chronic heart failure demonstrated subclinical pathophysiological, including decreased perfusion and hypoxia. The association could be a potential target for diagnosis and protective treatment.
Introduction
Renal dysfunction frequently coexists with chronic heart failure (HF) [1, 2] and it stands as a strong predictor of adverse clinical outcomes in patients with chronic HF [3,4]. Currently, the diagnosis of renal dysfunction relies on the estimated glomerular filtration rate(eGFR) level. However, kidneys process substantial functional reserve, allowing eGFR to remain a normal range before half the kidney function is lost. This challenge underscores the need of early kidney dysfunction detection of. Kidney MR imaging has scarcely been studied in the context of chronic HF, despite its potential to offer insights into preclinical pathophysiological changes of renal dysfunction non-invasively at early phase of chronic HF. The multiparametric renal MRI protocol, including ASL, R2* mapping, T1 mapping, T2 mapping, and DWI can provide quantitative information of perfusion, tissue oxygenation, interstitial fibrosis, edema, and diffusion without radiation or potential risks of contrast agents. Hence, in this study we aimed to assess early-stage renal abnormalities by multiparametric MRI in chronic HF patients with preserved renal function.Methods
16 individuals participated in this study, including 8 chronic HF patients with preserved renal function (eGFR>60 ml/min/1.73 m2), and 8 age- and gender-matched healthy volunteers. Patients with primary kidney disease were excluded. All 16 participants underwent renal MRI, which included the following sequences: T2WI with fat saturation, R2* mapping, T1 mapping, T2 mapping, research sequence kidney ASL and non-pTX Zoomed DWI with two b vaules(0,800s/mm2)on two 3T systems (MAGNETOM Spectra and Skyra, Siemens Healthineers, Erlangen, Germany). The detail scanning parameters are listed in table 1. To calculate parameter values, regions of interest (ROI) were manually drawn over the renal cortex by radiologist with 6 years of experience in kidney MR imaging with an area of 1–7 pixels. Specifically, ROIs were delineated in the upper pole, middle pole, and lower pole at the maximum coronal level images of the left and right kidney. And the average of the left and right kidney parameter values (including renal cortex perfusion values -renal blood follow (RBF), T1 relaxation time, T2 relaxation time, R2*, and ADC values) were used for further calculations. Statistical analyses were performed using SPSS/PC (version 22.0, IBM SPSS Statistics, USA). A statistical significance level of p<0.05 was used. Continuous variables were compared using analysis of variance (ANOVA). Paired continuous variables (left and right sided measurements) were compared using a t-test for paired samples.Results
All five MRI parameters were similar between left and right kidneys for the overall population (p=0.064, 0.714, 0.159, 0.671, 0.064) (Table 2). In patients with chronic HF, renal cortex RBF values were decreased compared to healthy volunteers (153.9±39.4 ml/100 g/min vs. 311.9±61.8 ml/100 g/min; p<0.01), and renal R2* were increased compared to healthy volunteers’ (21.5±3.0 s-1 vs. 17.9±3.4 s-1; p=0.043) (Figure1, 2). There are no significant differences of T1 relaxation time (1616.4±78.3 ms vs. 1571.0±161.8 ms, p=0.486), T2 relaxation time (45.0±1.9 ms vs. 47.8±3.4 ms, p=0.061), and ADC values (1253.3±49.4 mm2/s vs. 1269.1±77.2 mm2/s, p=0.634) between chronic HF patients and the controls (Table 3)(Figure 3).Discussion
In this preliminary study, we undertook a comprehensive evaluation of renal tissue parameters, including perfusion, tissue oxygenation, interstitial fibrosis, edema, and diffusion, to assess the preclinical pathophysiological changes of kidneys in chronic HF patients. Notably, our findings indicated that early-stage renal abnormalities are present in these patients even before conventional serum biomarkers of kidney dysfunction exhibit abnormalities. Compared with healthy controls, a decreased RBF value and an increased R2* value has been observed both in chronic HF patients. These results indicate that renal hypoperfusion and hypoxia occur at an early stage in chronic HF patients, even in the absence of evident serum biomarkers of the kidney abnormalities. Previous study suggested renal T1 relaxation time to be only prolonged in HF patients with impaired renal function [5]. In our study, we found no difference in T1 relaxation time, T2 relaxation time, and ADC values between healthy volunteers and HF patients with preserved renal function. This suggested significant chronic reno-parenchymal damage such as fibrosis has not occurred in HF patients with preserved renal function.Conclusion
Our study revealed that even with no clinical symptoms and preserved eGFR, patients with chronic HF demonstrated early-stage renal abnormalities, including decreased renal tissue perfusion and hypoxia. These findings indicate a potential value of MR in detecting subclinical changes of kidneys in chronic HF patients with preserved renal function.Acknowledgements
No acknowledgement found.References
[1] Adams KF Jr, Fonarow GC, Emerman CL, LeJemtel TH, Costanzo MR, Abraham WT (2005) Characteristics and outcomes of patients hospitalized for heart failure in the United States: rationale, design, and preliminary observations from the first 100,000 cases in the Acute Decompensated Heart Failure National Registry (ADHERE). Am Heart J 149:209–216
[2] McAlister FA, Ezekowitz J, Tonelli M, Armstrong PW (2004) Renal insufficiency and heart failure: prognostic and therapeutic implications from a prospective cohort study. Circulation 109:1004–1009 [3] Smilde TD, Hillege HL, Voors AA, Dunselman PH, Van Veldhuisen DJ (2004) Prognostic importance of renal function in patients with early heart failure and mild left ventricular dysfunction. Am J Cardiol 94:240–243
[4] Breidthardt T, Socrates T, Noveanu M, Klima T, Heinisch C, Reichlin T et al (2011) Effect and clinical prediction of worsening renal function in acute decompensated heart failure. Am J Cardiol 107: 730–735 [5] Breidthardt T, Cox EF, Squire L, Odudu A, Omar NF, Eldehni,MT et al (2015) The pathophysiology of the chronic cardiorenal syndrome: a magnetic resonance imaging study.Eur Radiol 25:1684-91
Figures
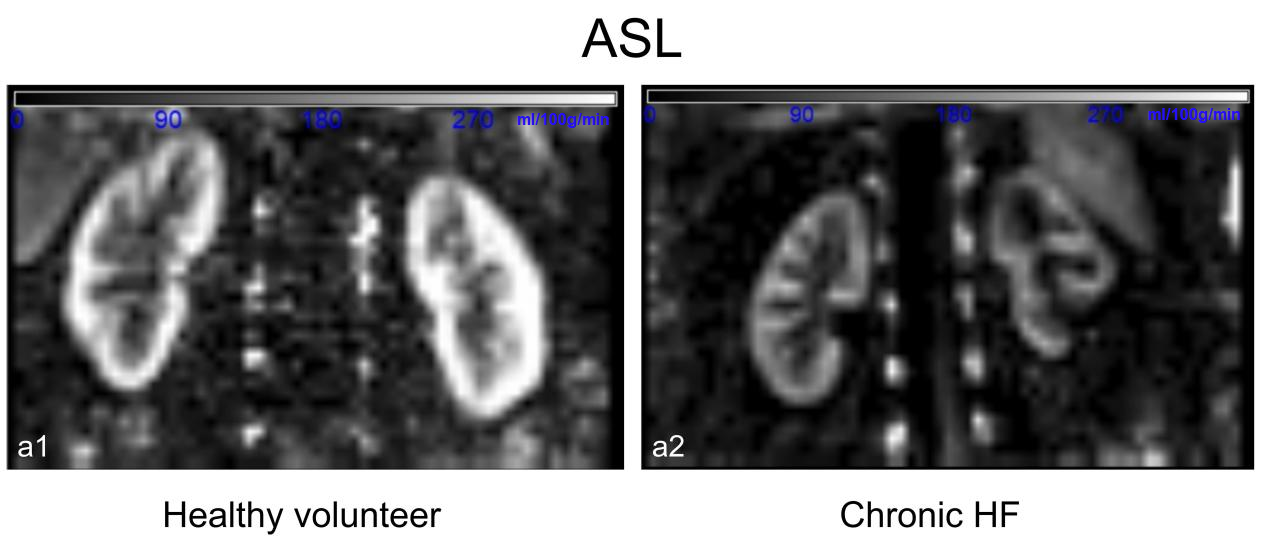
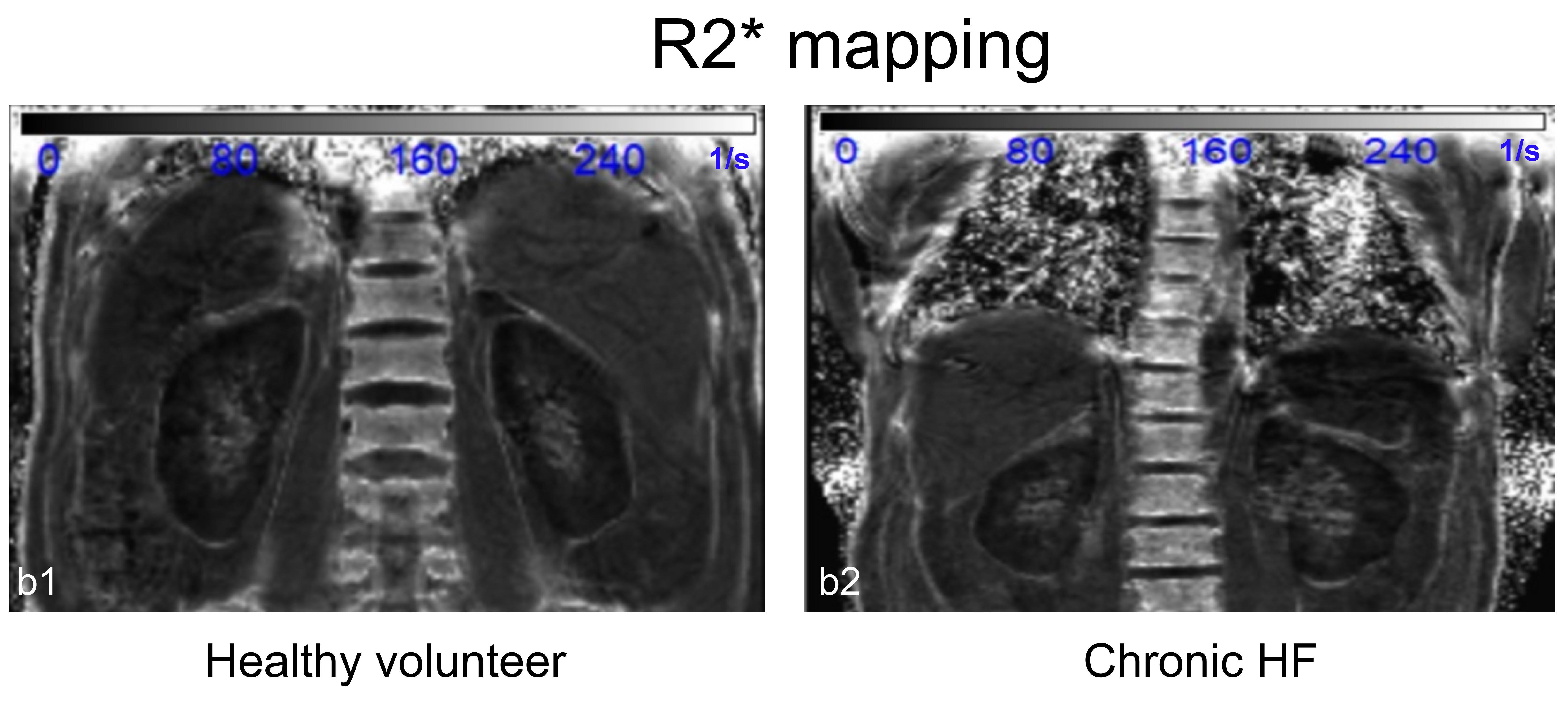
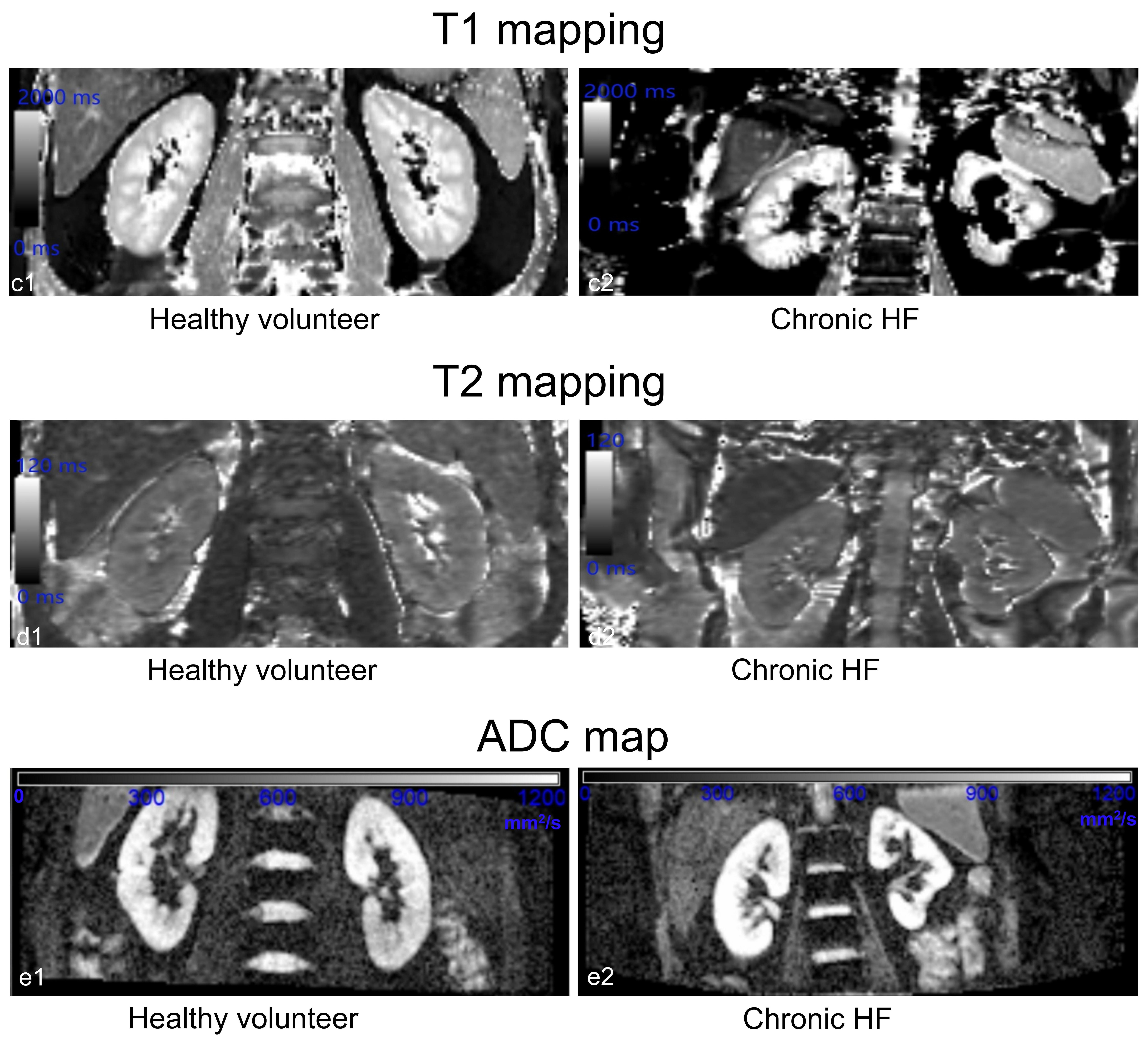
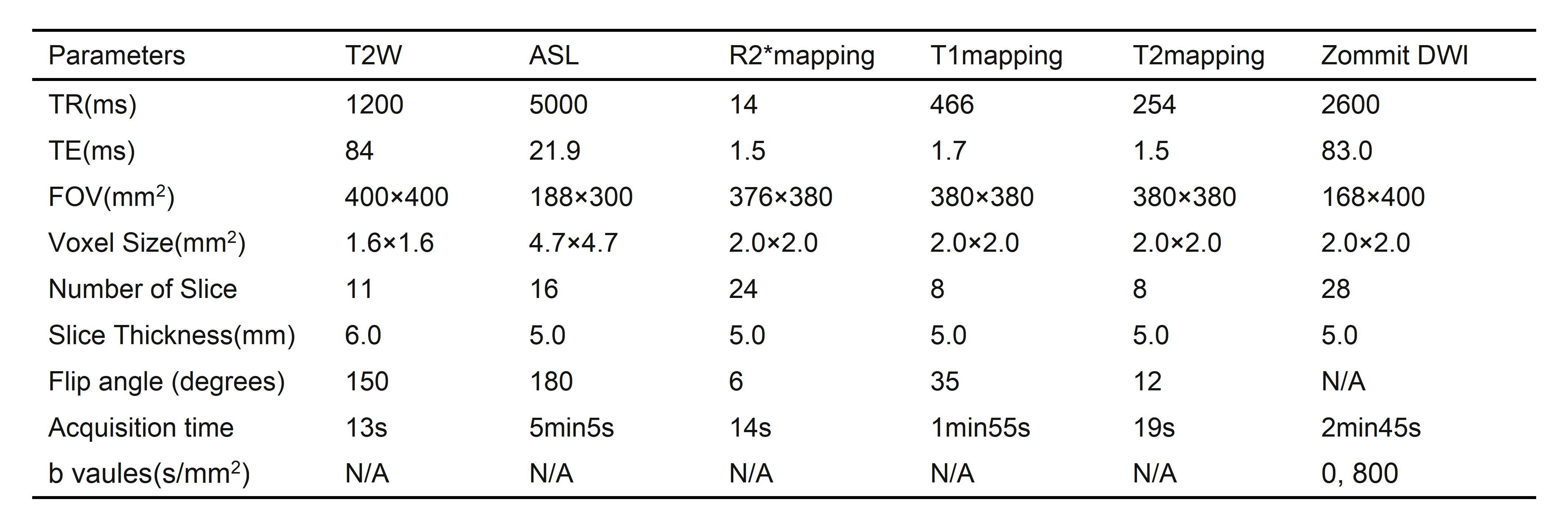
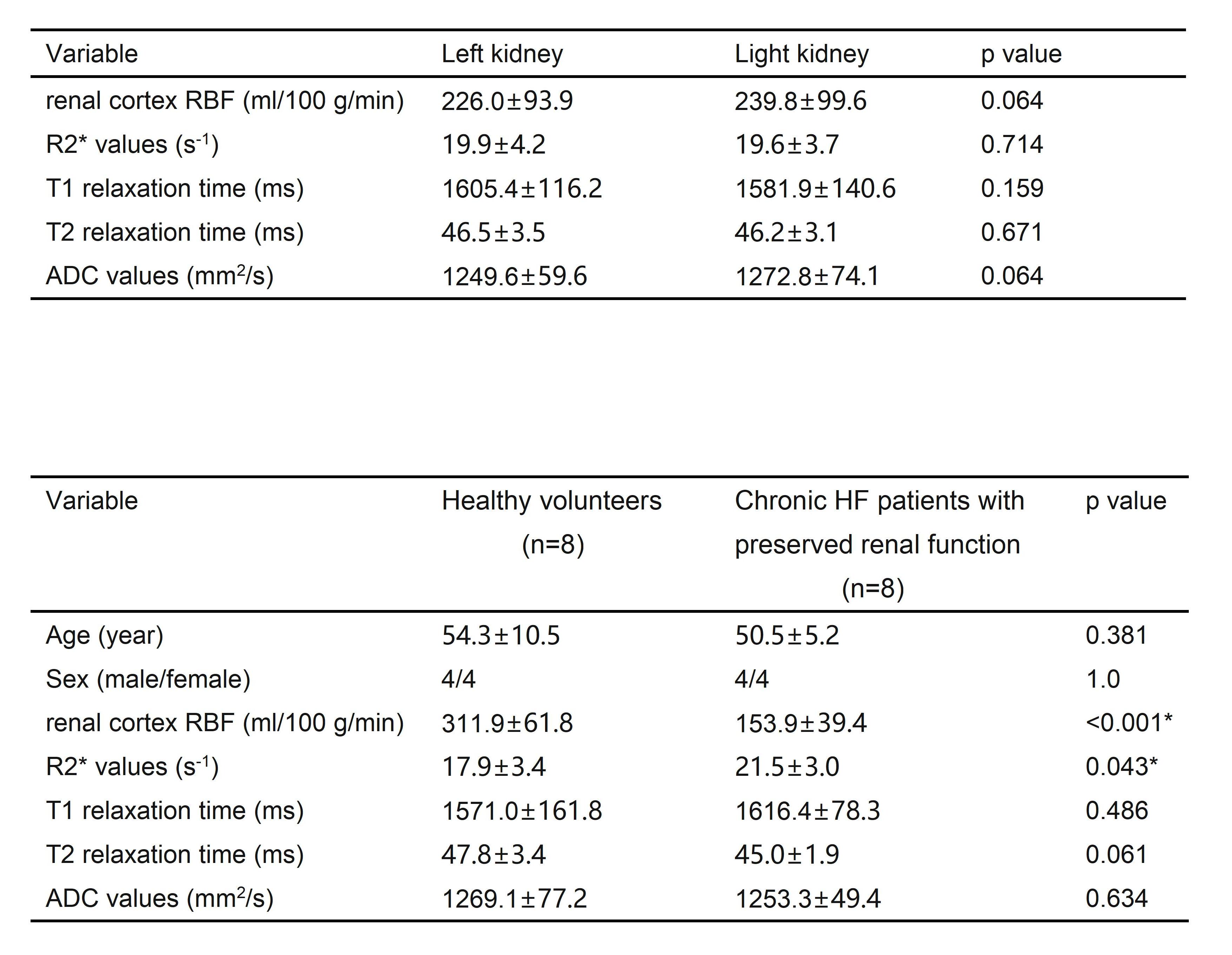
Table 2 Comparison of parameter values between left and right kidneys for the overall population
Table 3 Comparison of clinical characteristics and MRI parameter values between HF patients and controls