4623
Effects of Kidney Perfusion levels on Renal Stiffness and Fluidity measured with Tomoelastography in an MRI-compatible ex-vivo model1University Medical Center Groningen, Groningen, Netherlands, 2University Hospital Charitè, Berlin, Germany
Synopsis
Keywords: Kidney, Elastography
Motivation: Tomoelastography allows for early detection of changes in the renal stiffness of various kidney pathologies. However, variations in tissue perfusion can have a strong impact on the assessment of renal stiffness.
Goal(s): To characterize the effect of tissue perfusion on renal stiffness and tissue fluidity.
Approach: Five ex vivo porcine kidneys were separately perfused in an MRI-compatible normothermic machine perfusion setup and simultaneously examined by Tomoelastography.
Results: Our results show a strong positive correlation between increasing tissue perfusion and stiffness in the cortex and medulla of ex vivo porcine kidneys being observed after readily one minute of altered tissue perfusion.
Impact: Stiffness is an essential factor in diagnosing renal fibrosis. When the renal vasculature is highly perfused, it can mimic increased stiffness associated with renal fibrosis. Our study emphasizes the strong dependency of renal stiffness and fluidity on perfusion.
Introduction
Tomoelastography is a recently introduced quantitative MRI technique allowing the assessment of the mechanical properties of organs such as stiffness and fluiditiy(1). Previous studies demonstrated the diagnostic accuracy of tomoelastography to quantify renal stiffness in different cohorts(2–4). Despite these promising results, growing evidence indicates the influence of perfusion on tissue stiffness in addition to fibrosis(5–9).In this study, we aimed to examine to which extent blood pressure and blood flow influences the stiffness and fluidity in the cortex and medulla of ex-vivo porcine kidneys. To address this question, we assessed the shear wave speed (c) and phase angle of the shear modulus (φ) in five ex vivo porcine kidneys which were separately perfused in an MRI-compatible normothermic machine perfusion (NMP) circuit with altered blood pressure and blood flow.
Methods
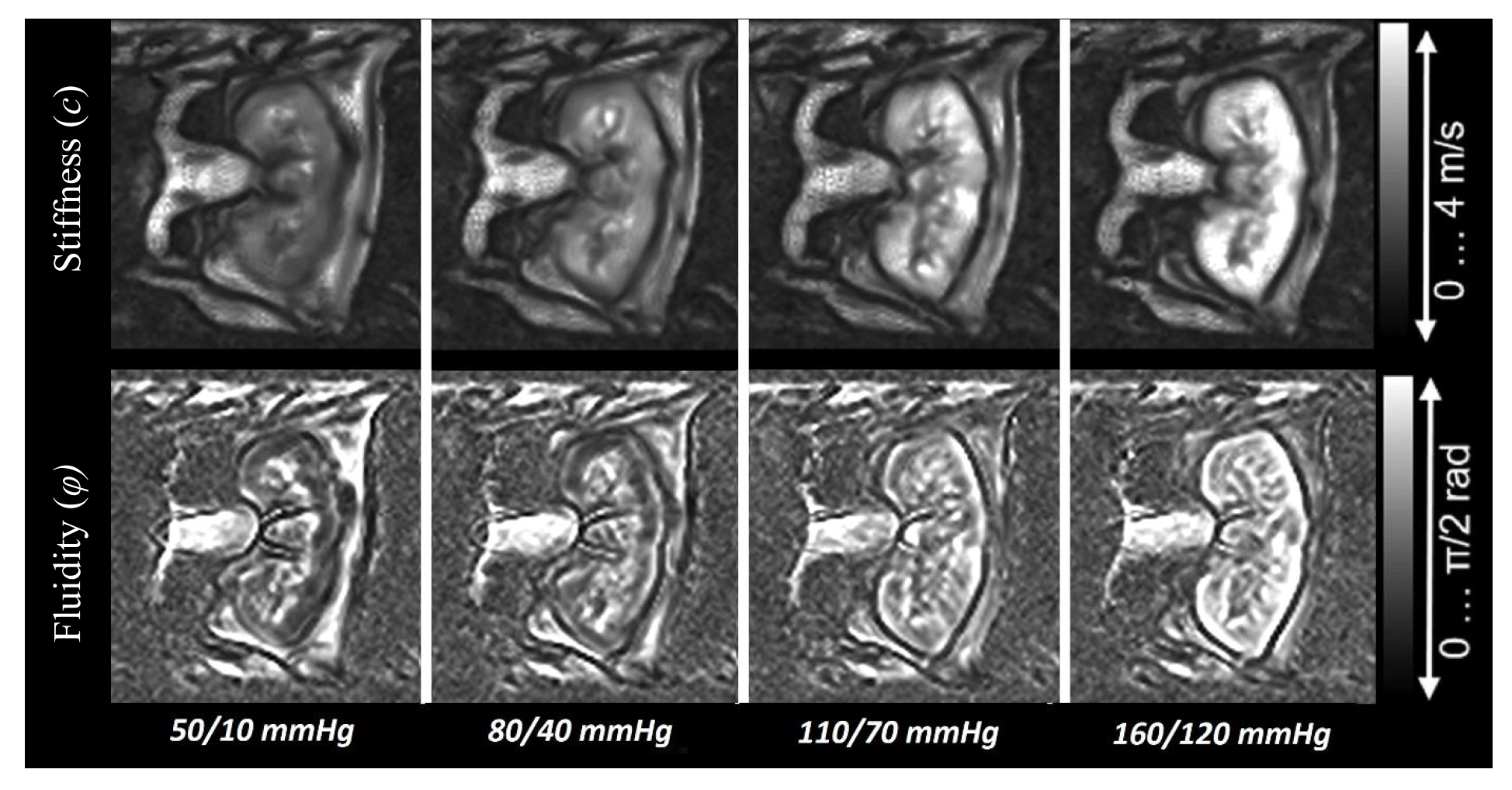
Five ex-vivo porcine kidneys were separately perfused in an MRI-compatible NMP circuit and examined by tomoelastography at four driving frequencies, ranging from 40 – 70 Hz. Adjusted blood pressure was in the range of 50/10 – 160/120 mmHg with a pause of one minute in between to adapt to the change in tissue perfusion. Resultant renal flow rates were externally measured on the arterial line with an ultrasonic flow sensor.All examinations were performed on a 3 T MRI system using a 20-channel phased-array head coil. Eight wave-phase offsets were recorded for each of the three motion directions. In total, 19 coronal slices with 2mm isotropic resolution covering the entire ex vivo kidney were acquired in four minutes. Other tomoelastography parameters were: TR = 2260 ms; TE = 69 ms; FOV of 256 × 256 mm². Tomoelastography data were post-processed using publicly available multifrequency dual elasto-visco inversion programs, more details are provided in Streitberger et al(10) and Tzschätzsch et al(1). Resulting stiffness (c) and fluidity (φ) were obtained from the cortex and medulla for each set blood pressure scenario.
Results
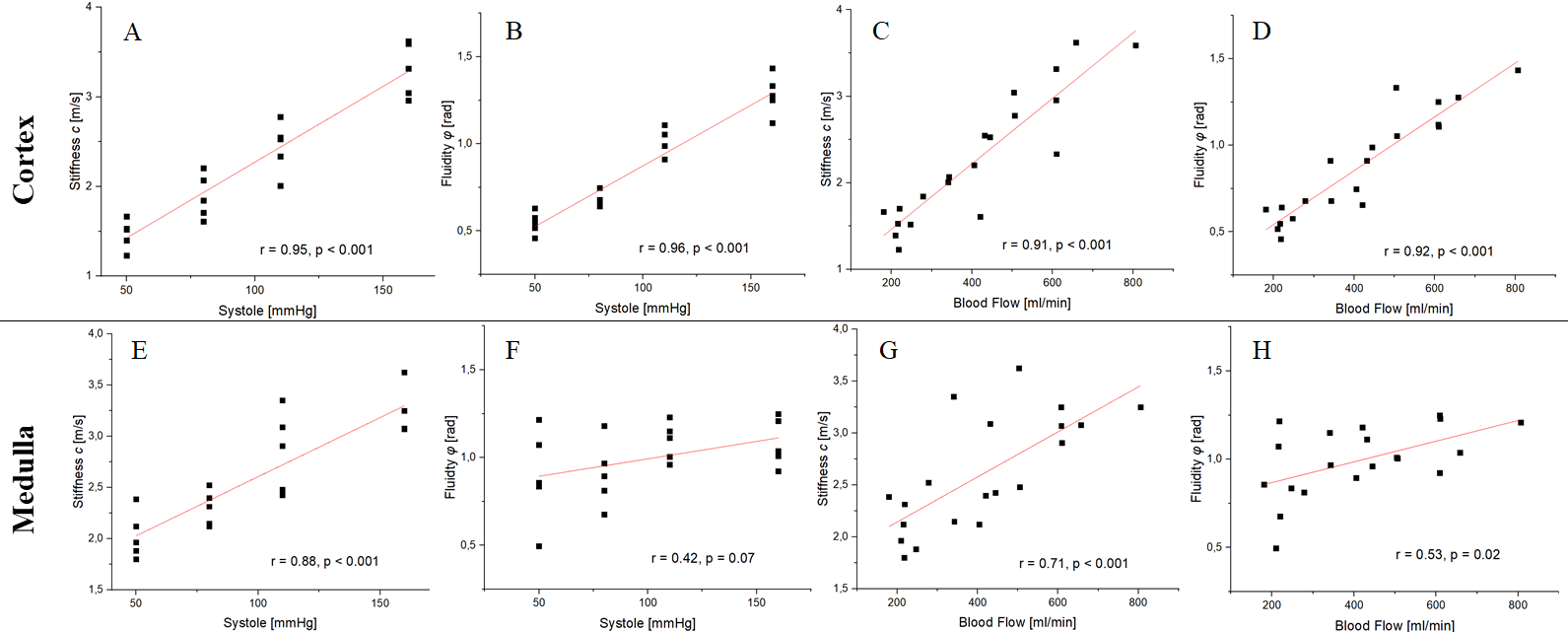
Overall, stiffness and fluidity increased with blood pressure in both the renal cortex and medulla. In the cortical tissue, wave speed increased in the order of approximately 124%, and fluidity by 132% in the range from 50/10 mmHg to 160/120 mmHg. In contrast, a much smaller increase in medullary mechanical properties was observed, being 60% in stiffness, and 21% in fluidity.Highly significant positive correlations were observed between systolic blood pressure and blood flow in cortical stiffness (blood pressure: r = 0.95, p < 0.001; blood flow: r = 0.91, p < 0.001) and fluidity (blood pressure: r = 0.96, p < 0.001; blood flow: r = 0.92, p < 0.001). Likewise, we found a statistically significant association between medullary stiffness and systolic blood pressure (r = 0.88, p < 0.001) and blood flow (r = 0.71, p < 0.001). On the contrary, there was no statistically significant correlation observed between medullary fluidity and systolic blood pressure (r = 0.42, p < 0.07) or blood flow (r = 0.53, p < 0.02).
Discussion
The entire kidney is surrounded by a fibrous capsule composed of tough fibers with minor flexibility. Increasing vascular pressure leads to an increase in renal cortical and medullary stiffness due to the minimal elasticity of the renal capsule. As one of the highly vascularized organs, variations in the renal perfusion will have a greater impact on the tomoelastography findings than in other organs. This effect may play a major role in the assessment of the mechanical properties of in vivo kidneys to detect early structural changes as well as to provide valid cut-off values for specific pathologies.Moreover, renal blood flow is well autoregulated and distributes about 80% of its blood flow to the cortex as well as 15% to the outer medulla(11). This variation in perfusion between the cortex and medulla is in line with the observed differences in the increase in stiffness (124% vs 60%) and fluidity (132% vs 21%) in our study. In addition, our results stress the minor elasticity of the fibrous renal capsule. To account for this perfusion dependency, the future use of a correction factor based on blood pressure or e.g. ASL derived blood flow may lead to higher validity in in-vivo renal tomoelastography as well as allow for better inter-study comparisons.
Conclusion
In conclusion, our study has highlighted the impact of perfusion on the mechanical properties of renal tissue. Moreover, we observed that renal stiffness and fluidity rapidly change with altered blood circulation. Future studies should focus on validating our encouraging results in an in vivo setting as well as exploring correction factors for perfusion dependency in certain renal pathologies such as renal fibrosis.Acknowledgements
No acknowledgement found.References
1. Tzschätzsch, H. et al. Tomoelastography by multifrequency wave number recovery from time-harmonic propagating shear waves. Med. Image Anal. 30, 1–10 (2016).
2. Garcia, S. R. M. et al. Multifrequency magnetic resonance elastography for the assessment of renal allograft function. Invest. Radiol. 51, 591–595 (2016).
3. Garcia, S. R. M. et al. Tomoelastography for longitudinal monitoring of viscoelasticity changes in the liver and in renal allografts after direct-acting antiviral treatment in 15 kidney transplant recipients with chronic hcv infection. J. Clin. Med. 10, 1–15 (2021).
4. Marticorena Garcia, S. R. et al. Tomoelastography paired with T2∗ magnetic resonance imaging detects lupus nephritis with normal renal function. Invest. Radiol. 54, 89–97 (2019).
5. Gandhi, D. et al. Magnetic Resonance Elastography of Kidneys: SE-EPI MRE reproducibility and its comparison to GRE MRE. NMR Biomed. 32, e4141 (2019).
6. Brown, R. S. et al. The utility of magnetic resonance imaging for noninvasive evaluation of diabetic nephropathy. Nephrol. Dial. Transplant 35, 970–978 (2020).
7. Yin, M. et al. Distinguishing between Hepatic Inflammation and Fibrosis with MR Elastography. Radiology 284, 694–705 (2017).
8. Warner, L. et al. Noninvasive In vivo assessment of renal tissue elasticity during graded renal ischemia using MR elastography. Invest. Radiol. 46, 509–514 (2011).
9. Gennisson, J. L., Grenier, N., Combe, C. & Tanter, M. Supersonic shear wave elastography of in vivo pig kidney: influence of blood pressure, urinary pressure and tissue anisotropy. Ultrasound Med. Biol. 38, 1559–1567 (2012).
10. Streitberger, K. J. et al. High-resolution mechanical imaging of glioblastoma by multifrequency magnetic resonance elastography. PLoS One 9, (2014).
11. Duke, J. Renal Function and Anesthesia. Anesth. Secrets 308–316 (2011) doi:10.1016/B978-0-323-06524-5.00045-3.
Figures