4621
Volumetric TSE-Based DWI Acquisition with a Pseudospiral K-Space Trajectory and Phase Correction Algorithm: Application in the Breast1Department of Radiology, UT Southwestern Medical Center, Dallas, TX, United States, 2Advanced Imaging Research Center, UT Southwestern Medical Center, Dallas, TX, United States
Synopsis
Keywords: Breast, Data Acquisition, Breast, Diffusion
Motivation: Current image quality limitations of conventional diffusion weighted sequences in the breast offer an exciting opportunity for novel acquisitions that can generate distortion-free images within clinically feasible scan times.
Goal(s): To test a novel TSE-based 3D DWI sequence (VD-CASPR) in the breast of healthy volunteers and assess image quality with an incorporated phase correction algorithm.
Approach: Four healthy volunteers were scanned with current reference standard DW-EPI and DW-TSE for breast serving as benchmark for our 3D DWI sequence.
Results: Our VD-CASPR sequence with phase correction was able to generate high quality images at various b-values within shorter scan times compared to DW-TSE.
Impact: Our novel 3D DWI sequence and reconstruction pipeline generated high SNR images free of geometric distortions in the breast of healthy volunteers. Volumetric coverage without geometric distortion can facilitate co-registration with anatomical images for improved tumor characterization.
Introduction
Diffusion-weighted imaging (DWI) has become a highly valuable MR technique in the assessment of breast cancer with many institutions incorporating DWI sequences into their clinical breast imaging protocols1,2. Single-shot EPI (ss-EPI) sequences are the reference standard for DW breast images mainly due to their short acquisition times and robustness to subject motion3. However, a significant drawback of DW-EPI is its susceptibility to magnetic field inhomogeneities, which can cause geometric distortions and incomplete fat suppression in the resulting images4. In this work we present a novel 3D sequence that reduces artifacts in breast DW images by using a fast spin-echo readout, variable-density sampling and a phase correction algorithm. We show preliminary results of our Variable Density Cartesian Acquisition with Spiral Profile Reordering (VD-CASPR) sequence in the breast of three healthy volunteers.Theory and Methods
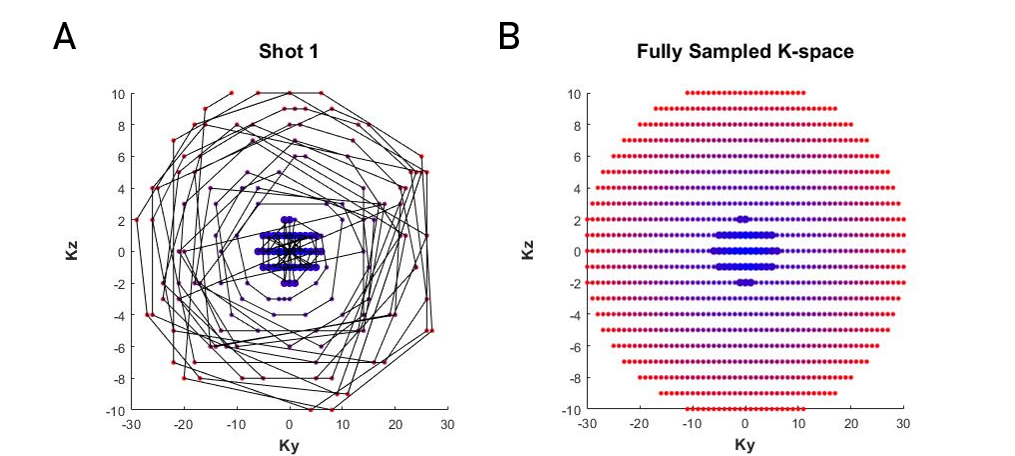
In VD-CASPR, each Ky-Kz profile (or readout in the Kx direction) is acquired following a pseudo spiral trajectory on a cartesian grid. At the beginning of each echo train, a user-defined number of profiles in the center of k-space is consistently sampled. The remaining ETL – N profiles are then sampled following a pseudo-spiral trajectory that is calculated based on a golden-step angle algorithm5. At the end of the acquisition, we will effectively have a fully sampled outer shell of k-space and an oversampled inner shell of k-space. This oversampled region increases the overall SNR of the sequence and also serves as navigators to correct for phase errors that result from the multi-shot acquisition.The acquisition trajectory is calculated based on the field of view (FOV), resolution, and echo train length (ETL). The first N profiles (Ninner), which are closest to the center of k-space, are repeatedly acquired at the beginning of each shot. The total number of shots depends on Ninner as well as the total number of profiles and can be calculated by the following equation: $$$Shots=\frac{ETL-N_{inner}}{Profiles – N_{inner}}$$$.
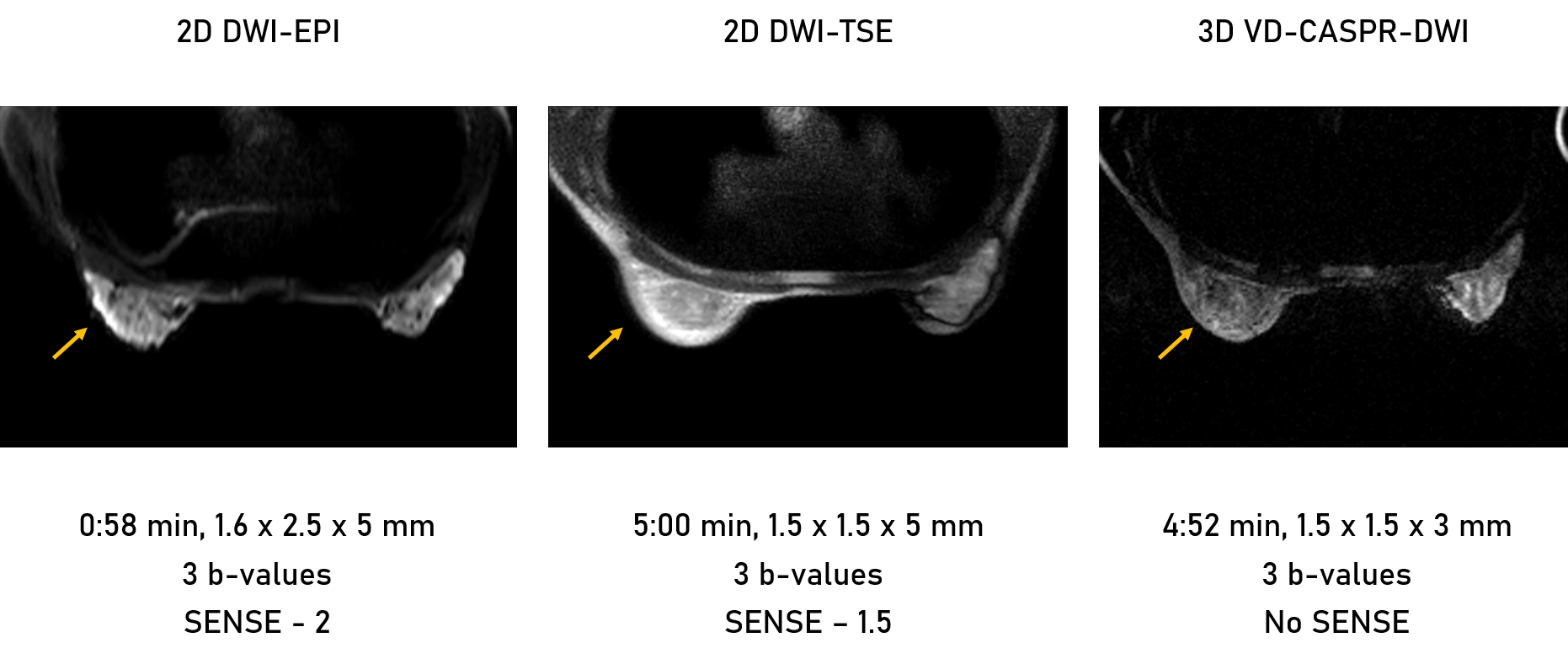
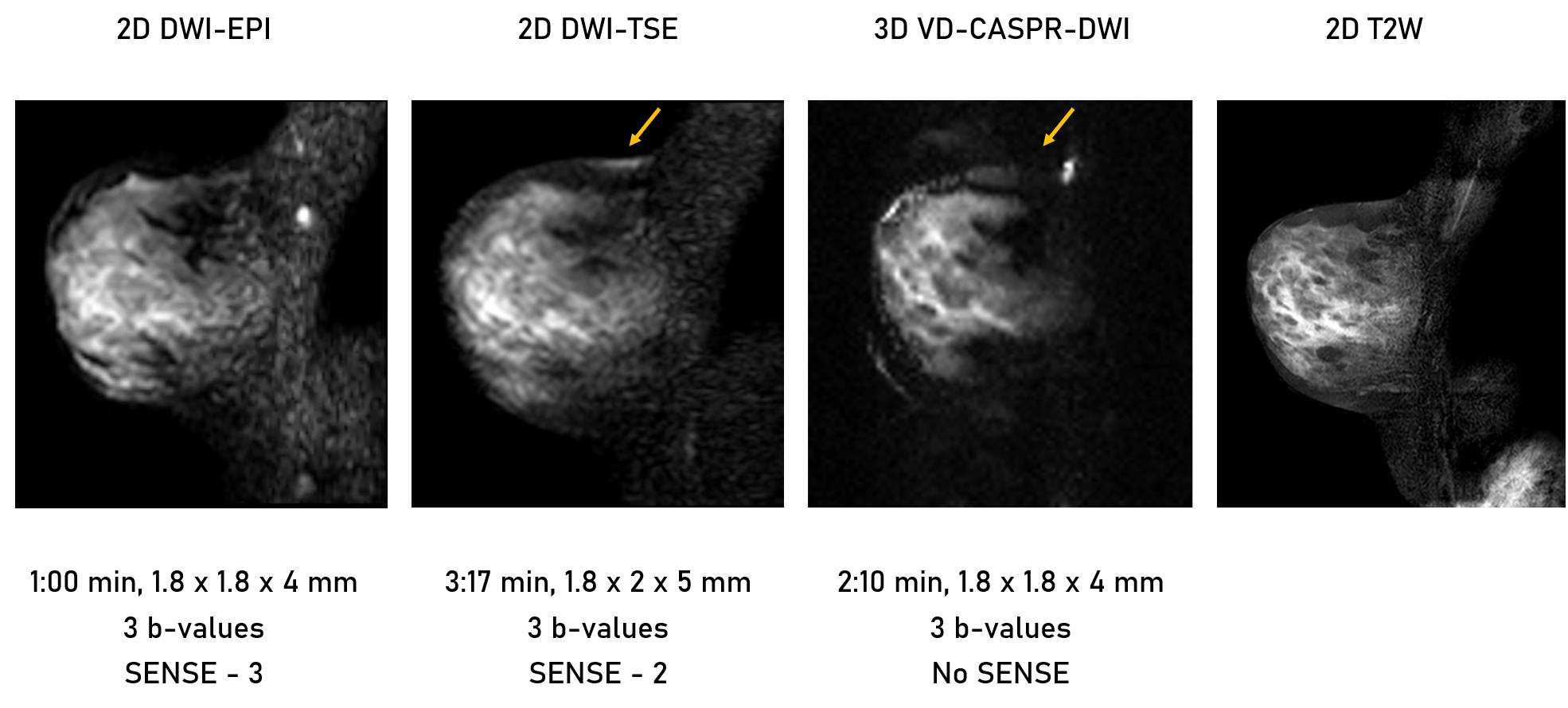
Sagittal and axial images were obtained from three healthy volunteers under an approved IRB protocol. Sagittal VD-CASPR parameters were: TR/TE = 2000/81 ms, ETL = 92, acquired resolution = 1.8x1.8x4 mm3, FOV = 200x200x48 mm3, Ny = 109, Nz = 27, Ninner = 10, b = 0, 200, and 500 s/mm2, scan time = 2:10 minutes. Axial VD-CASPR parameters were: TR/TE = 2000/69 ms, ETL = 92, acquired resolution = 1.5x1.5x3 mm3, FOV = 220x300x48 mm3, Ny = 109, Nz = 27, Ninner = 10, b = 0, 200, and 500 s/mm2, scan time = 4:52 minutes. All VD-CASPR acquisitions were performed with SPIR fat suppression.
K-space data were exported to MATLAB (Mathworks Inc., Natick, Massachusetts) for phase correction, which was previously validated on phantoms. For our algorithm, we created two datasets: the first containing the undersampled k-space acquired in each shot, and the second containing the center-most profiles that are sampled across all echo trains. Both datasets were Fourier transformed and then the phase of the center-only dataset was subtracted from the undersampled dataset in image space. Finally, the phase-corrected data were averaged across shots to generate the final phase-corrected images.
Results
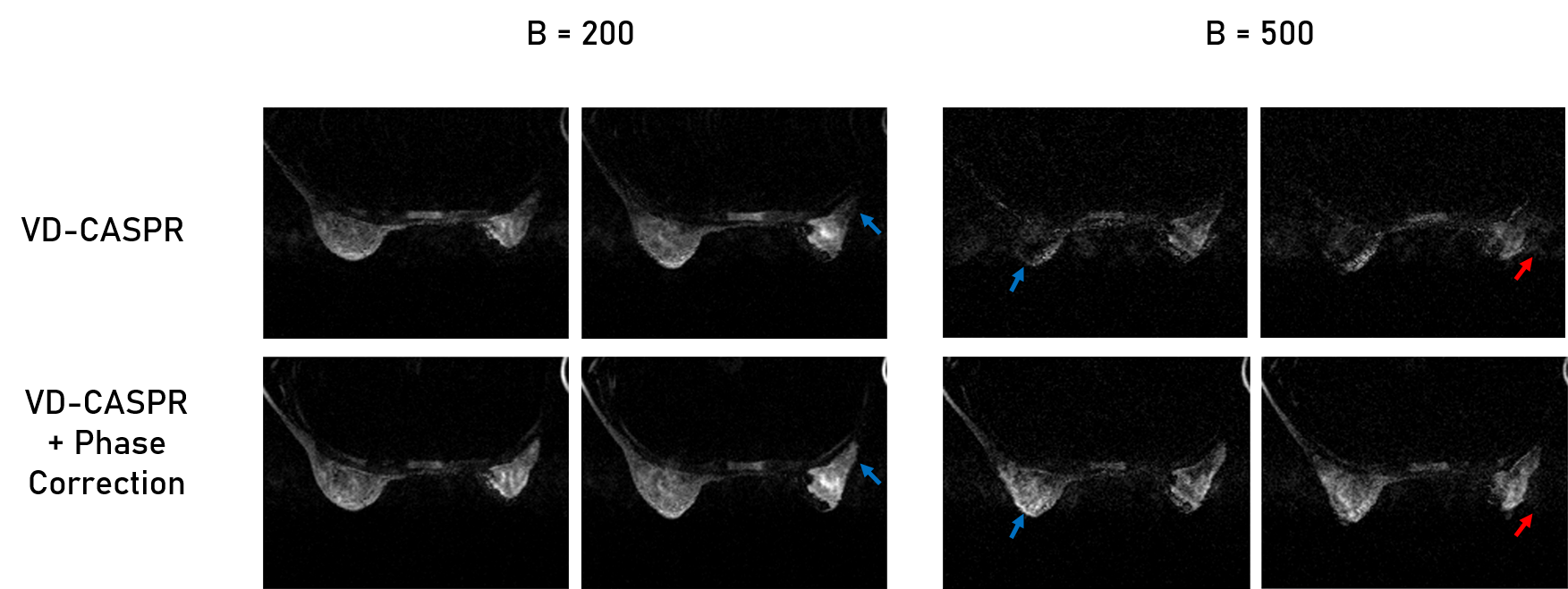
VD-CASPR images suffered from severe void artifacts and blurring, which were significantly improved once the phase correction algorithm was applied [Figure 2]. Additionally, VD-CASPR with phase correction was able to achieve improved image quality with high SNR at different b-values in both axial and sagittal orientations [Figures 3, 4]. Furthermore, VD-CASPR with phase correction showed excellent fat suppression at b = 0 s/mm2 and adequate fat suppression at b = 200, 500 s/mm2. In comparison, single shot DW-EPI had significant geometric distortions in axial and sagittal images. DW-TSE images did not suffer from geometric distortions but exhibited incomplete fat suppression near tissue interfaces and longer scan times compared to VD-CASPR, even with parallel imaging reconstruction. Lastly, VD-CASPR was able to achieve significantly reduced slice thickness in sagittal acquisitions, which could be highly beneficial for tumor detection and segmentation.Discussion and Conclusion
This work presents the application of our novel 3D sequence for volumetric diffusion weighted imaging in the breast. Phase corrected VD-CASPR achieved high quality images at low and intermediate b-values (b = 200, 500 s/mm2) that were robust to B0 inhomogeneities and phase induced errors. VD-CASPR was the diffusion sequence that most closely aligned to the T2-weighted acquisition. This highly valuable feature would allow for perfect co-registration with T2 and T1-weighted images for tumor characterization. Future work will explore additional reconstruction steps to improve image quality at higher b-values (b = 800 s/mm2), where noise is substantially increased.Acknowledgements
This work was supported by NIH/NCI grants U01CA207091, R01CA283663, and CPRIT RP190049. The authors would like to thank all volunteers for their participation in this study. The authors also thank Abey Thomas, RT(MR), Courtney Dawson, RT(MR), Michael Fulkerson, AS, LVN, and Camille Harry, for their help in human imaging, and Ben Wagner, MSEE, for his help with image database and analysis routines.References
1. Partridge, S. C. and E. S. McDonald (2013). "Diffusion weighted magnetic resonance imaging of the breast: protocol optimization, interpretation, and clinical applications." Magn Reson Imaging Clin N Am 21(3): 601-624.
2. Partridge, S. C., et al. (2017). "Diffusion-weighted breast MRI: Clinical applications and emerging techniques." J Magn Reson Imaging 45(2): 337-355.
3. Wenkel, E., et al. (2007). "Diffusion weighted imaging in breast MRI: comparison of two different pulse sequences." Acad Radiol 14(9): 1077-1083.
4. Singer, L., et al. (2012). "High-resolution diffusion-weighted magnetic resonance imaging in patients with locally advanced breast cancer." Acad Radiol 19(5): 526-534.
5. Prieto, C., et al., Highly efficient respiratory motion compensated free-breathing coronary MRA using golden-step Cartesian acquisition. J Magn Reson Imaging, 2015. 41(3): p. 738-46.
Figures