4620
Short Supine Breast Magnetic Resonance Imaging to Assess Preoperative Breast Radiotherapy Boost Targets1Breast Imaging, MD Anderson Cancer Center, Houston, TX, United States, 2Imaging Physics, MD Anderson Cancer Center, Houston, TX, United States, 3Biostatistics, MD Anderson Cancer Center, Houston, TX, United States, 4Radiation Physics, MD Anderson Cancer Center, Houston, TX, United States, 5Breast Radiation Oncology, MD Anderson Cancer Center, Houston, TX, United States
Synopsis
Keywords: Breast, Breast
Motivation: Breast MRI is performed prone and has not been optimized for supine treatment position and with the personalized radiation mold, limiting application for radiation treatment monitoring
Goal(s): To evaluate the image quality and tumor size accuracy from short supine breast MRI (ssbMRI).
Approach: ssbMRI studies were acquired before and after neoadjuvant radiotherapy along with mammography and ultrasound in 20 patients. Image quality of ssbMRI was evaluated by expert readers and image derived tumor sizes were correlated with other imaging modalities and final pathology.
Results: ssbMR had acceptable image quality in 70% of the cases and best correlation with pathology.
Impact: Breast MRI in supine positioning is of diagnostic quality despite the technical challenges for patients with breast cancer. This pilot study allows the development of a short supine diagnostic breast MRI for radiation planning and possibly fusion with CT.
Introduction
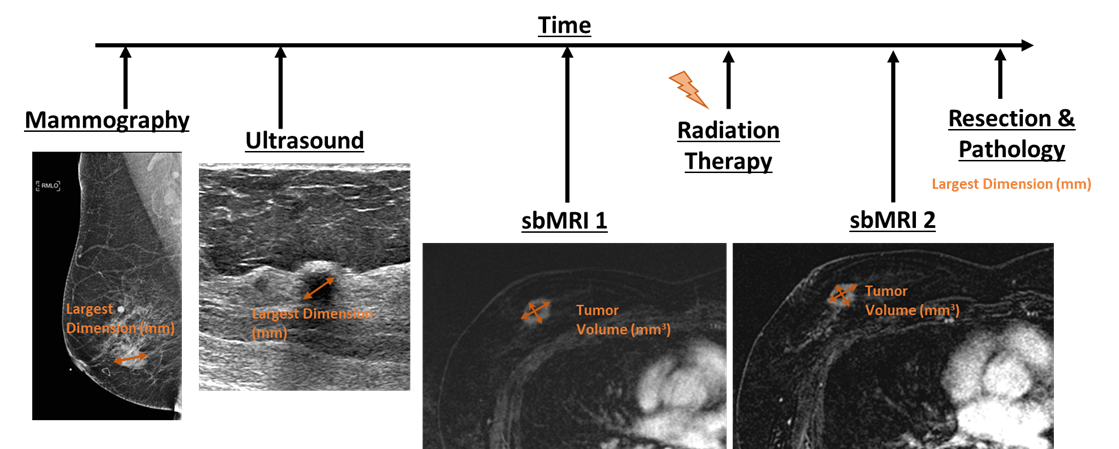
Breast MRI is most commonly performed in a prone position and with a dedicated breast coil for the diagnosis and follow-up of breast cancer patients1,2. Although it can also be useful for monitoring the response to radiotherapy, breast MRI has not been optimized for a typical supine treatment position and with the personalized radiation mold. This work aims to investigate the feasibility of a short breast MRI (ssbMRI) with the patient in a supine position, with a personalized radiation treatment immobilization mold and a flexible phases array body coil. We evaluated the image quality and accuracy of tumor size measurement of ssbMRI compared to mammography, ultrasound and final surgical pathology.Methods
20 breast cancer patients undergoing neoadjuvant radiotherapy prior to surgery were recruited to this IRB approved prospective study. All patients received diagnostic mammogram and ultrasound as standard of care at a single cancer center. ssbMRI was performed with a personalized radiation mold and with the patient in a supine position. ssbMRI consisted of the following sequences: (1)a 3-plane localizer in 0:22min, (2) axial T2-weighted Dixon in 4:09min, (3) and axial contrast enhanced DISCO of 8-14 phases in 2:02 min, (5) sagittal post-contrast T1-weighted Dixon in 3:03min. All images were acquired with the patient in a supine position and a 24-channel phased array flexible body coil placed around the radiation mold. The exam was abbreviated compared to the conventional breast MRI to improve patient’s tolerance and comfort. The same ssbMRI was performed before (MRI1) and after (MRI2) the preoperative radiation boost treatment that was completed 6-8 days prior to surgery. Images were reviewed by a specialized breast radiologist and a radiation oncologist with 22 and 16 years of experience, respectively. MR image quality was subjectively assessed for overall fat saturation homogeneity and tumor margin conspicuity, using a 3-point scale of poor, average, and good. For ultrasound and mammography images and pathology, the longest single axis of the tumor was measured. For 3D MR images, the volume of the tumor was calculated by multiplying the longest dimension in three orthogonal plans using the post contrast T1- weighted dynamic series. Correlation coefficients and linear fit norms were calculated for all size measurements.Results
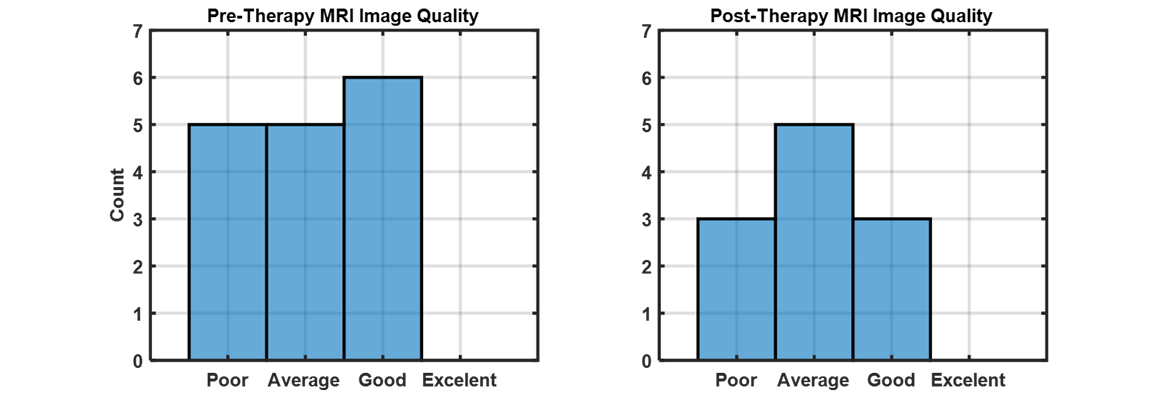
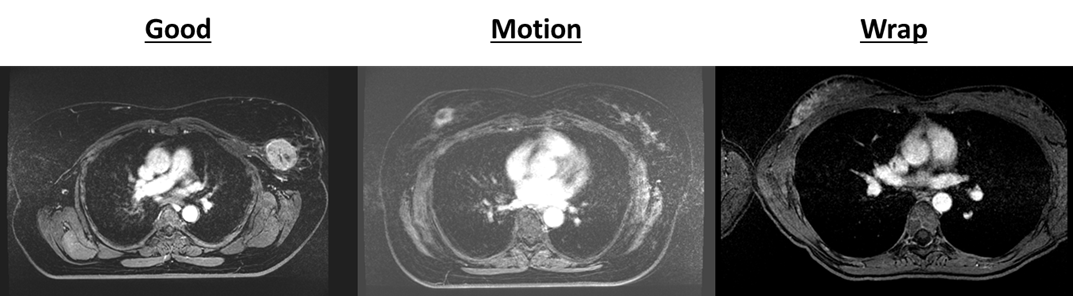
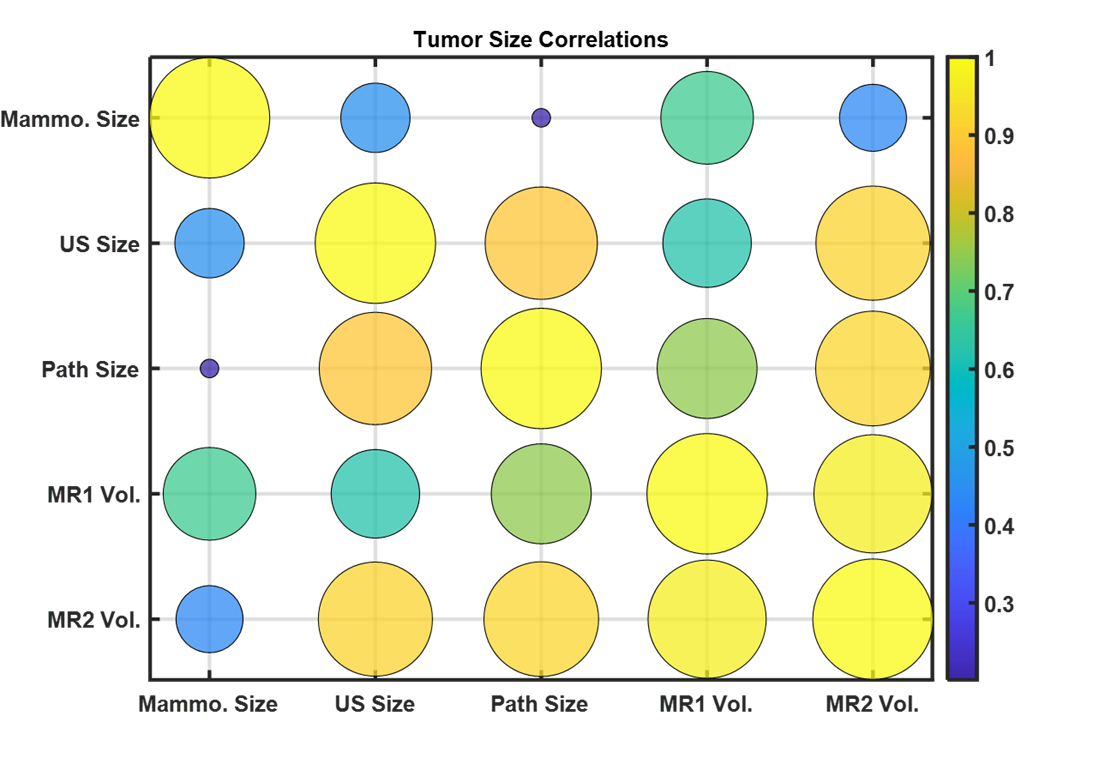
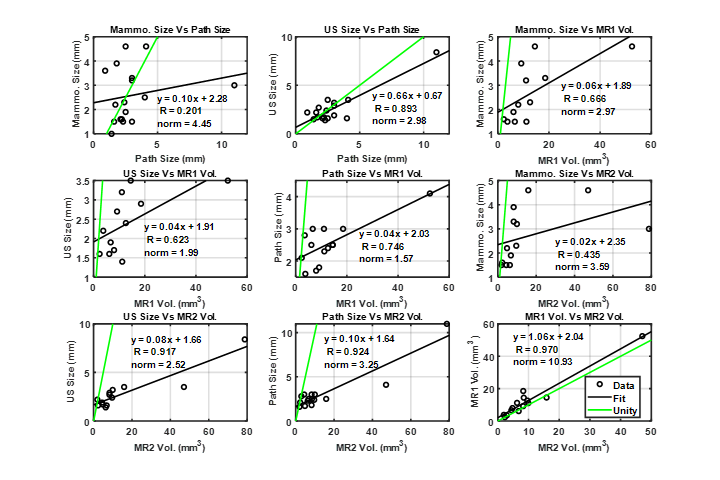
18 of 20 enrolled patients completed both sets of ssbMRI that are available for analysis. All patients had clinical stage IA-IIIB breast cancer, 10 right-sided and 8 left-sided. Average age at diagnosis is 54.4, range 33 – 73. 13/18 (70%) MRI studies were considered of diagnostic quality or average to good on subjective evaluation of overall fat saturation homogeneity and tumor margin conspicuity (Figure 1). The remaining cases were categorized as poor in image quality due to artifacts from signal wrap-around, respiratory/involuntary motion, or cardiac motion through the tumor bed (Figure 2). Median table time for ssbMRI was approximately 30 minutes and the actual total acquisition time was approximately 15 minutes. Average tumor size is 2.8 cm on mammogram, 2.6 cm on ultrasound, 2.8 cm on pre-radiation MRI1, and 2.5 cm on post-radiation MRI2. Average tumor size on final pathology is 2.9 cm, range 0.9 – 11cm. When tumor volume was calculated between the pre-RT and post-RT MRI, tumor volume decreased by -2.661 mm3 or -21.4% change after RT (p=0.550). MRI2 best correlated with final surgical pathology size (R = 0.92), compared to MRI1 (R = 0.75), US (R = 0.89), mammogram (R = 0.2) (Figure 3). A significant decrease of 22.4% between tumor size on MRI1 and MRI2 was seen in response to therapy (p=0.007) but the values were still well correlated (R=0.97) was detected. Mammography size did not correlate with any other measurements (Figures 4 and 5). Ultrasound had the closest linear slope to unity but did not have the highest correlation. Volume calculations from MRI measurements best correlate with final pathology. All patients received breast conserving surgery, and none had experienced a recurrence during the median of 4 years follow-up (range 1 – 5 years). 18/20 patients with follow-up data received annual mammogram, and 8 received adjunct surveillance ultrasound in addition to mammogram. No patients received MRI surveillance after their breast cancer treatment.Conclusion
In this pilot study, a short breast MRI exam was successfully developed to enable adequate tumor bed visibility and accurate tumor size measurement for radiation planning and treatment response monitoring, despite common MRI artifacts associated with supine positioning and without a dedicated breast coil.Acknowledgements
No acknowledgement found.References
1. Newell MS, Giess CS, Argus AD, et al. ACR practice parameter for the performance of contrast enhanced magnetic resonance imaging (MRI) of the breast. Reston, Va: American College of Radiology, 2018.
2. Ritse M.M., Nariya C., and Linda M., Breast MRI: State of the Art. Radiology 2019 292:3, 520-536
Figures