4616
Pharmacokinetic analysis of ultrafast DCE-MRI for DCIS grading and prediction of DCIS upgrading to IDC1Radiology, The University of Chicago, Chicago, IL, United States, 2Loyola Stritch School of Medicine, Loyola University Chicago, Chicago, IL, United States
Synopsis
Keywords: Breast, Quantitative Imaging, Pharmacokinetic analysis, ultrafast DCE-MRI, DCIS grading, DCIS upgrade
Motivation: Accurate grading and predicting the upgrade of DCIS can assist in surgical planning.
Goal(s): This study investigates whether the pharmacokinetic parameters from ultrafast DCE-MRI can differentiate DCIS grade and predict the upgrade of DCIS at surgery.
Approach: We reviewed data from 35 patients with DCIS who underwent a protocol that included preoperative ultrafast DCE-MRI (temporal resolution = 3-9 seconds) for the first minute after contrast administration. We measured pharmacokinetic parameters in DCIS from ultrafast images.
Results: The results show that Kep separates low-grade DCIS from intermediate and high-grade DCIS. High-grade DCIS with short bolus arrival time is associated with an upgrade to IDC.
Impact: Pharmacokinetic analysis of ultrafast DCE-MRI could distinguish low-grade DCIS from non-low-grade DCIS and could predict upgrade of high-grade DCIS to IDC.
Introduction
Ductal carcinoma in situ (DCIS) is a pre-invasive breast cancer that starts in the mammary ducts but cannot spread beyond its intraductal region, constituting a known, non-obligate, precursor to invasive breast carcinoma (IDC)1. About 40% DCIS progresses to IDC2. Not surprisingly, the progression rate and time are dependent on the DCIS grade3 – low-grade DCIS lesions have slower progression rates and lower recurrence rates compared to high-grade DCIS lesions or DCIS lesions that are upgraded to IDC4. Accurate grading of DCIS is essential for determining the optimal treatment strategy and predicting outcomes. Breast dynamic-contrast enhancement magnetic resonance imaging (DCE-MRI) plays a vital role in detecting DCIS, particularly for high-grade DCIS5. Growing evidence has shown that ultrafast (UF) DCE-MRI, that uses high temporal resolution (3 – 10 s) during the early phase of contrast media uptake, can be useful in distinguishing DCIS from IDC6 with potential for establishing DCIS grading4 and predicting transformation of DCIS to IDC7. This study investigated whether the pharmacokinetic parameters from UF-DCE-MRI can separate DCIS grade and discriminate stable high-grade DCIS from cancers upgraded to IDC at surgery.Methods
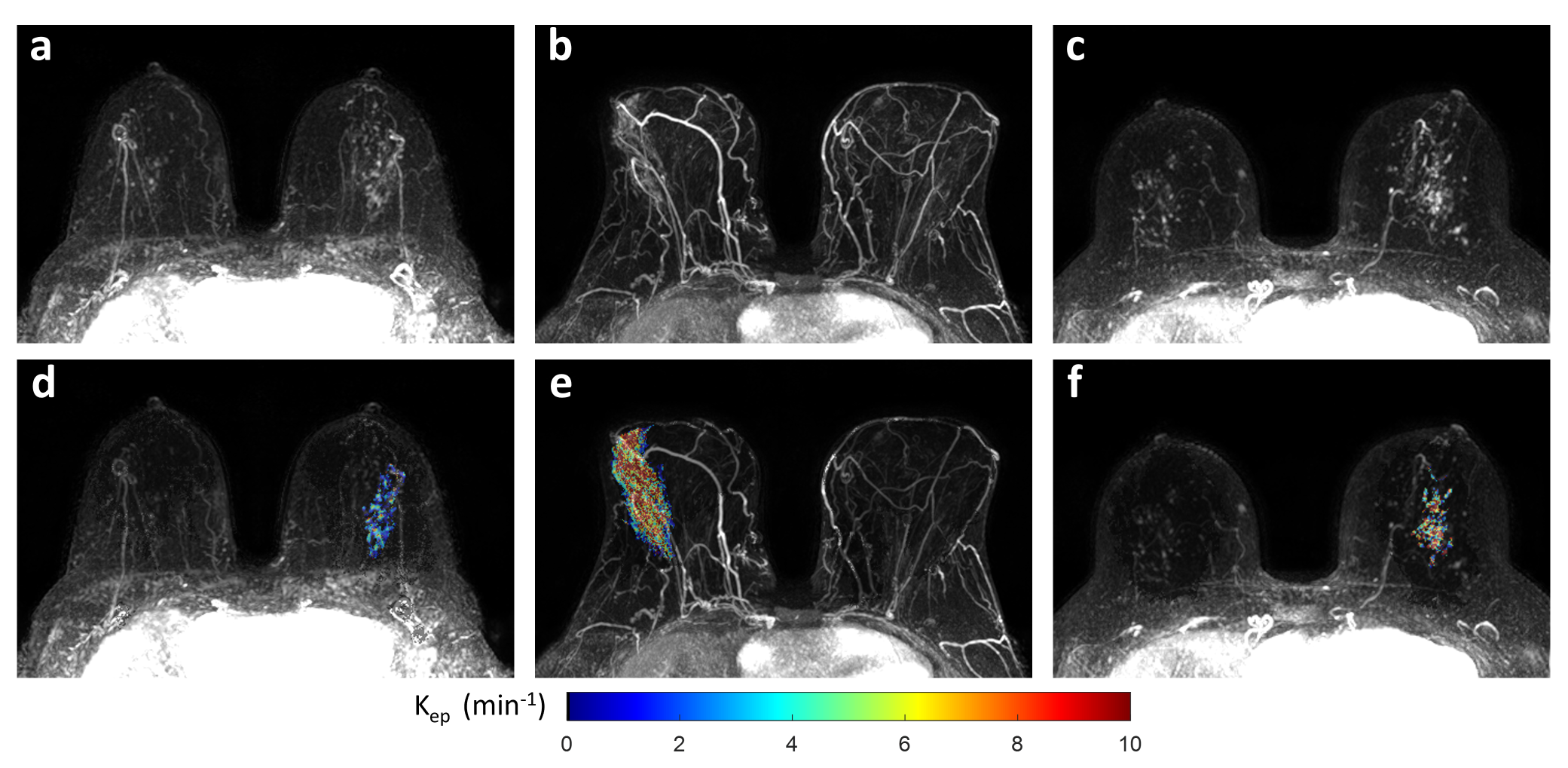
Our IRB approved this retrospective study and waived written informed consent. Thirty-five female patients (median age = 56, range = 25- 79) who were diagnosed with DCIS via biopsy and underwent pre-operative UF-DCE-MRI were enrolled. Data analysis was performed with an in-house MATLAB platform and 3D Slicer. UF images were motion- corrected with a non-rigid registration method8. A semi-automatic volumetric segmentation was performed with 3D Slicer using the first pre-contrast ultrafast time point9. Tumors were manually segmented based on a subtraction image and with guidance of respective radiology reports. Then, the regions of interest (ROIs) were refined using Otsu’s threshold and region growing from voxels with the maximum intensity in each unconnected region. Contrast agent concentration ($$$C(t)$$$) as a function of time (t) was calculated in each pixel using a previously published method based on the gradient echo signal equation (non-linear model) with a literature value of T1. A manually selected region of $$$7\times7$$$ pixels over aorta were used to measure the arterial input function (AIF). The literature values of T1 = 1700 ms for blood10, and T1= 1400 ms11 for breast tissue were used in calculations. Bolus arrival time (BAT) was calculated on the subtraction images by determining the time in seconds between first AIF enhancement in aorta and first enhancement in each lesion pixel. The Tofts model12 was used to fit C(t) to obtain maps of physiological parameters (Ktrans, ve and Kep):$$\int_{0}^{t} C_p(\tau)\exp(-(t-\tau)K^{trans}/v_e)d\tau$$where $$$C_p(t)$$$ is the AIF, $$$K^{trans}$$$ is the volume transfer constant between blood plasma and the extravascular extracellular space (EES), $$$v_e$$$ is the volume of EES per unit volume of tissue, and Kep is the ratio of $$$K^{trans}$$$ over $$$v_e$$$. The Kruskal-Wallis test was used for multiple comparison of MRI parameters by DCIS grade. The Wilcoxon rank-sum test was used to compare MRI parameters between upgrade and non-upgrade groups. A value of p <.05 was considered statistically significant.
Results
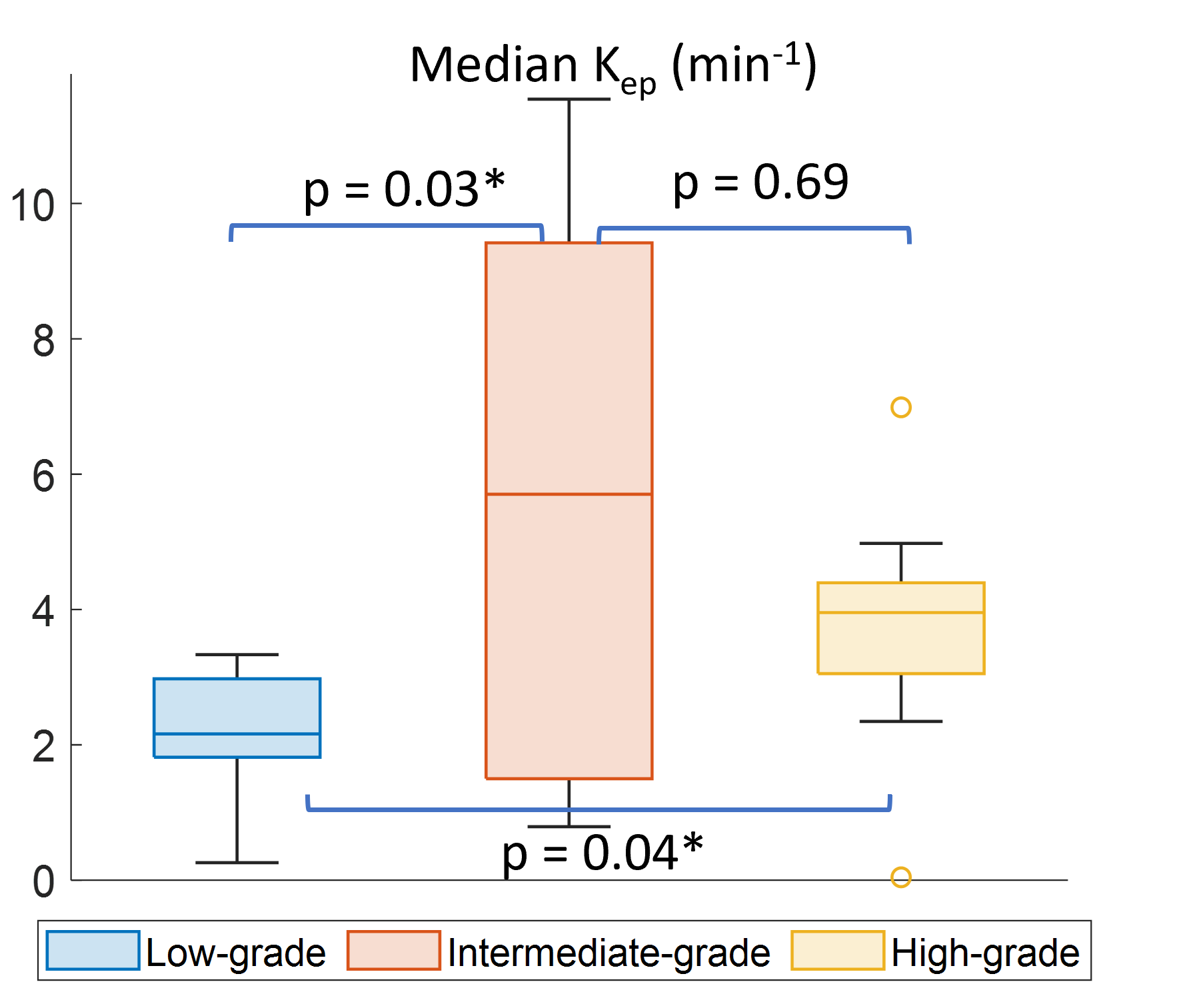
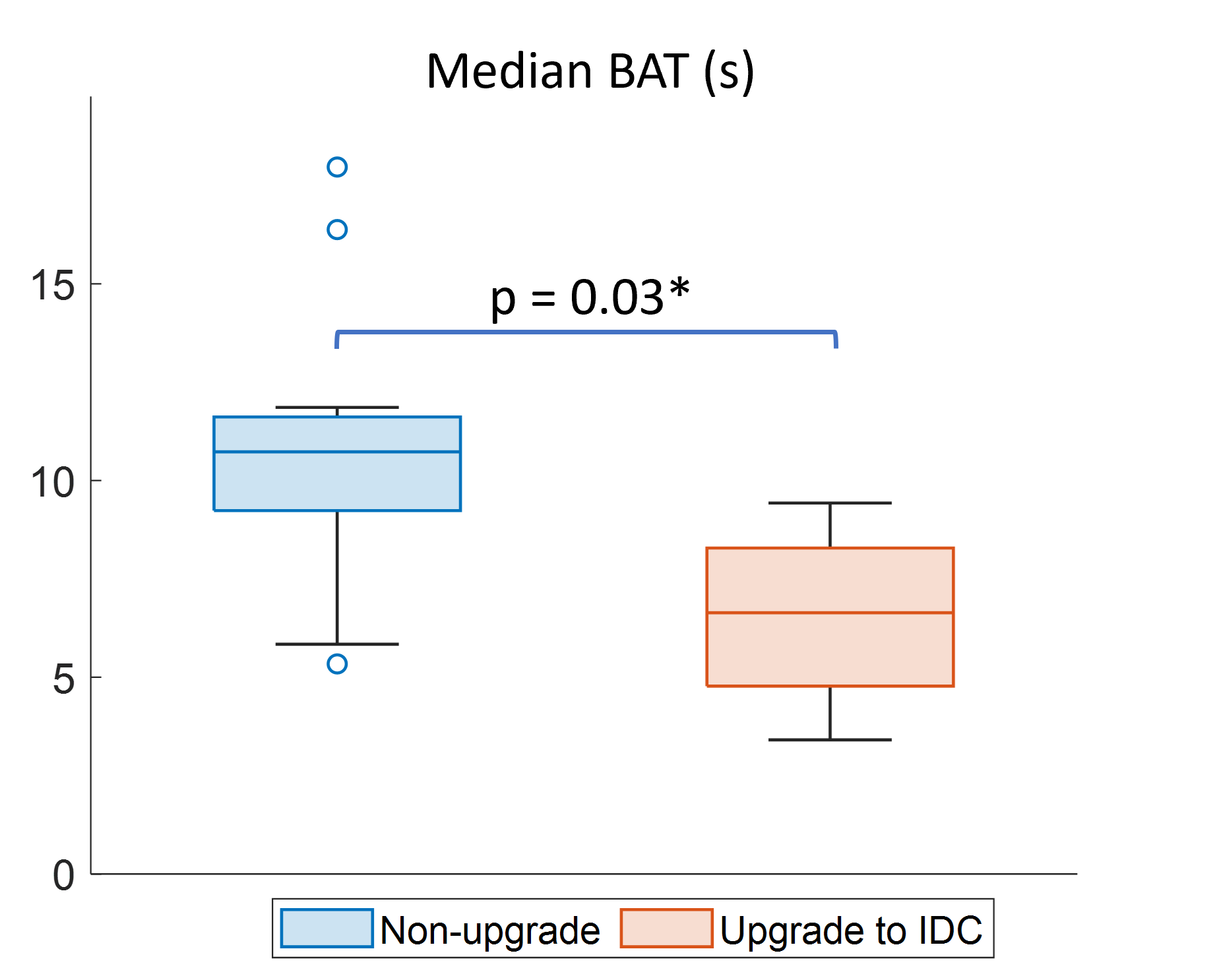
At biopsy, 23 patients were diagnosed with high-grade DCIS: 6 with intermediate-grade, and 6 with low-grade DCIS. After surgery (on average 41 days from biopsy), 4 high-grade DCIS cases (17%) were found to be upgraded to IDC, 1 intermediate-grade DCIS (17%) developed microinvasion, and 2 low-grade DCIS cases (33%) were upgraded to intermediate-grade DCIS. The median value of Kep significantly differentiates between DCIS grades (p = 0.02): low-grade DCIS has significantly lower median Kep than intermediate-grade (p=0.03) and high-grade DCIS (p = 0.04). However, there is no difference between intermediate-grade and high-grade DCIS (p = 0.69) (Figure 1 and Figure 2). There is no evidence of association between $$$K^{trans}$$$, $$$v_e$$$, BAT, and DCIS grades. The upgrade of high-grade DCIS to invasive cancer was significantly associated with shorter BAT on preoperative UF-DCE-MRI (p = 0.03) (Figure 3), but there is no evidence of association between upgrade of low-and intermediate-grade DCIS and MRI parameters.Discussion
While previous studies reported that no effective kinetic parameters from DCE-MRI can differentiate DCIS grade4, the result here shows that low Kep, reflecting low transfer rate from EES to blood plasma, is associated with low-grade DCIS. An early contrast uptake in high-grade DCIS might be an indicator for future upgrade to IDC. Higher temporal resolution would improve prediction of an upgrade of DCIS based on bolus arrival time.Conclusion
The preoperative UF-DCE-MRI has potential to assist in differentiating DCIS grades and prediction of upgrade of high-grade DCIS to IDC at surgery. The information can aid in surgical planning of DCIS.Acknowledgements
This study is supported in part by the National Cancer Institute of the National Institutes of Health through grants U01 CA142565, R01 CA172801, 1U24 CA226110, 1F32 CA265232, the Segal Family Foundation, the University of Chicago Cancer Center.References
1. Gorringe KL, Fox SB. Ductal Carcinoma. Front Oncol. 2017;7:248. doi:10.3389/fonc.2017.00248
2. Dettogni RS, Stur E, Laus AC, et al. Potential biomarkers of ductal carcinoma in situ progression. BMC Cancer. Feb 12 2020;20(1):119. doi:10.1186/s12885-020-6608-y
3. Salvatorelli L, Puzzo L, Vecchio GM, Caltabiano R, Virzì V, Magro G. Ductal Carcinoma In Situ of the Breast: An Update with Emphasis on Radiological and Morphological Features as Predictive Prognostic Factors. Cancers (Basel). Mar 06 2020;12(3)doi:10.3390/cancers12030609
4. Mori N, Abe H, Mugikura S, et al. Discriminating low-grade ductal carcinoma in situ (DCIS) from non-low-grade DCIS or DCIS upgraded to invasive carcinoma: effective texture features on ultrafast dynamic contrast-enhanced magnetic resonance imaging. Breast Cancer. Sep 2021;28(5):1141-1153. doi:10.1007/s12282-021-01257-6
5. Tajima CC, de Sousa LLC, Venys GL, Guatelli CS, Bitencourt AGV, Marques EF. Magnetic resonance imaging of the breast: role in the evaluation of ductal carcinoma in situ. Radiol Bras. 2019;52(1):43-47. doi:10.1590/0100-3984.2018.0058
6. Shin SU, Cho N, Kim SY, Lee SH, Chang JM, Moon WK. Time-to-enhancement at ultrafast breast DCE-MRI: potential imaging biomarker of tumour aggressiveness. Eur Radiol. Jul 2020;30(7):4058-4068. doi:10.1007/s00330-020-06693-0
7. Miceli R, Gao Y, Qian K, Heller SL. Predicting Upgrade of Ductal Carcinoma In Situ to Invasive Breast Cancer at Surgery With Ultrafast Imaging. AJR Am J Roentgenol. Jul 2023;221(1):34-43. doi:10.2214/AJR.22.28698
8. Vercauteren T, Pennec X, Perchant A, Ayache N. Diffeomorphic demons: efficient non-parametric image registration. Neuroimage. Mar 2009;45(1 Suppl):S61-72. doi:10.1016/j.neuroimage.2008.10.040
9. Ren Z, Pineda FD, Howard FM, et al. Differences Between Ipsilateral and Contralateral Early Parenchymal Enhancement Kinetics Predict Response of Breast Cancer to Neoadjuvant Therapy. Acad Radiol. Mar 26 2022;doi:10.1016/j.acra.2022.02.008
10. Shen Y, Goerner FL, Snyder C, et al. T1 relaxivities of gadolinium-based magnetic resonance contrast agents in human whole blood at 1.5, 3, and 7 T. Invest Radiol. May 2015;50(5):330-8. doi:10.1097/RLI.0000000000000132
11. Rakow-Penner R, Daniel B, Yu H, Sawyer-Glover A, Glover GH. Relaxation times of breast tissue at 1.5T and 3T measured using IDEAL. J Magn Reson Imaging. Jan 2006;23(1):87-91. doi:10.1002/jmri.20469
12. Tofts PS, Brix G, Buckley DL, et al. Estimating kinetic parameters from dynamic contrast-enhanced T(1)-weighted MRI of a diffusable tracer: standardized quantities and symbols. J Magn Reson Imaging. Sep 1999;10(3):223-32. doi:10.1002/(sici)1522-2586(199909)10:3<223::aid-jmri2>3.0.co;2-s
Figures