4614
Diagnosis of Breast Lesions on MRI using BI-RADS and Kaiser Score in Mass and Non-Mass Enhancement: Benefit of KS and KS+ for Different Readers1First affiliated hospital of Wenzhou Medical University, Wenzhou, China, 2University of California, Irvine, Irvine, CA, United States
Synopsis
Keywords: Breast, Breast
Motivation: Kaiser score (KS) could help diagnose lesions of breast MRI by an intuitive flowchart.
Goal(s): To compare the diagnostic performance of BI-RADS and KS and to evaluate the benefit of the modified KS+ by incorporating diffusion.
Approach: 630 patients were analyzed independently by three radiologists with different experiences, including 458 mass and 172 non-mass enhancement (NME) lesions.
Results: KS outperforms the unstructured BI-RADS, especially for less experienced readers. The diagnosis for NME was more difficult than for masses, true for three readers regardless of the method used. The accuracy of KS+ was improved for masses, but not for NME.
Impact: Kaiser Score provides an intuitive method for lesion interpretation, primarily helpful for mass lesions read by less experienced readers. KS+ is mainly applicable to mass lesions. For NME, the KS criteria need to be improved.
Introduction
Kaiser score (KS) is a machine learning–derived clinical decision rule based on MRI BI-RADS descriptors, which provides the structure of an intuitive flowchart to guide the reader through a stepwise lesion assessment. The main considered features include root sign, DCE pattern, internal enhancement, and peritumoral edema. Moreover, DWI has been incorporated with KS as the modified KS+ to improve diagnostic accuracy. Although non-mass enhancement (NME) lesions were considered during the development phase, the number of cases was small, and these features were not well-defined for NME. The purpose of this study was (1) to compare the diagnostic performance of three readers with different experiences interpreting breast MRI using the BI-RADS and KS systems, (2) to evaluate the benefit of the modified KS+ by incorporating diffusion, and (3) to assess the diagnostic performance in mass and NME lesions separately.Methods
A total of 630 patients receiving MRI for breast cancer diagnosis were included in this study. The pathological diagnosis revealed 393 malignant and 237 benign. Based on the morphology, the cases were separated into mass (N=458) and non-mass enhancement (N=172). Three radiologists with different levels of experience interpreting breast MRI (3, 6, and 13 years) reviewed the cases to make a diagnosis using BI-RADS descriptors and the Kaiser Score tree flowchart. The diagnostic AUC using these two methods in Mass and NME were separately analyzed and compared. Of the 630 cases, 596 (434 mass and 162 NME) had diffusion-weighted imaging, and the apparent diffusion coefficient (ADC) was measured to modify KS to KS+. For lesions with ADC > 1.4 x 10-3 mm2/s, the KS was reduced by 4. The diagnostic AUC of KS and KS+ made by three readers in mass and NME were compared to evaluate the benefit of KS+.Results
The diagnostic performance increased with years of experience among three readers. When using BI-RADS, AUC was 0.878, 0.915, and 0.941 for mass lesions, and 0.771, 0.838, and 0.902 for NME for Reader-1, 2, and 3, respectively. For each reader, the performance is better for mass than for NME. When using KS compared to BI-RADS, the diagnostic accuracy was improved for the less experienced Readers. For Reader-1, AUC was increased from 0.878 to 0.916 for mass (p=0.005), and from 0.771 to 0.822 for NME (p=0.124). For Reader-2, AUC was about the same for mass (0.915 to 0.921) and increased from 0.838 to 0.883 for NME (p=0.114). For the most experienced Reader-3, the results made by BI-RADS and KS were about the same. When ADC was considered to change to KS+, the AUC was significantly improved for all three readers for the mass lesions, but the AUC was about the same for NME.Discussion
The BI-RADS lexicon does not provide processing strategies for transforming specific imaging features into a particular diagnostic category. Integrating the variety of lesion characteristics into the diagnostic analysis is a complex and experience-dependent task and, thus, is more challenging for junior and inexperienced radiologists. KS system is performed step by step according to the tree flowchart to assign a score for each lesion, which is simple and practical without the need for extensive diagnostic training. In this study, we compared the diagnostic performance of three radiologists with different experiences using BI-RADS and KS flowchart. Also, we evaluated the benefit of modified KS+ when diffusion was considered. Furthermore, the diagnosis in mass and NME groups were separately analyzed. The results showed that compared to BI-RADS, KS significantly improved the diagnostic performance for mass lesions, especially for less experienced readers, confirming that Kaiser Score provides an intuitive method for interpreting and diagnosing lesions on breast MRI. The diagnosis of NME is much more challenging than for mass lesions using both BI-RADS and KS. When considering ADC to modify KS to KS+, the benefit was seen for mass lesions. However, the AUC only increased slightly with p values close to 0.05. The main advantage was the improved specificity with slightly degraded sensitivity. Among the three readers, using KS+ could correctly diagnose 9-13 more benign cases (decreased false positives) while missing 1-3 more cancers (increased false negatives), and whether this trade-off in clinical practice is acceptable is debatable. For NME, the benefits of KS and KS+ needed to be clarified, and the criteria may need further improvement.Acknowledgements
This study was supported in part by Research Incubation Project of First Affiliated Hospital of Wenzhou Medical University (No. FHY2019085), Wenzhou Science & Technology Bureau (No. Y20210232), Zhejiang Provincial Natural Science Foundation of China (LY21F020030) and Key Laboratory of Intelligent Medical Imaging of Wenzhou (No. 2021HZSY0057).References
[1]. Baltzer PA, Dietzel M, Kaiser WA (2013) A simple and robust classification tree for differentiation between benign and malignant lesions in MR-mammography. Eur Radiol 23:2051-2060.
[2]. Dietzel M, Baltzer PAT (2018) How to use the Kaiser score as a clinical decision rule for diagnosis in multiparametric breast MRI: a pictorial essay. Insights Imaging 9:325-335.
[3]. Marino MA, Clauser P, Woitek R et al (2016) A simple scoring system for breast MRI interpretation: does it compensate for reader experience? Eur Radiol 26:2529-2537.
[4]. Woitek R, Spick C, Schernthaner M et al (2017) A simple classification system (the Tree flowchart) for breast MRI can reduce the number of unnecessary biopsies in MRI-only lesions. Eur Radiol 27:3799-3809.
[5]. Grippo C, Jagmohan P, Helbich TH, Kapetas P, Clauser P, Baltzer PAT (2021) Correct determination of the enhancement curve is critical to ensure accurate diagnosis using the Kaiser score as a clinical decision rule for breast MRI. Eur J Radiol 138:109630.
[6]. Dietzel M, Krug B, Clauser P et al (2021) A Multicentric Comparison of Apparent Diffusion Coefficient Mapping and the Kaiser Score in the Assessment of Breast Lesions. Invest Radiol 56:274-282.
[7]. Chen ZW, Zhao YF, Liu HR et al (2022) Assessment of breast lesions by the Kaiser score for differential diagnosis on MRI: the added value of ADC and machine learning modeling. Eur Radiol 32:6608-6618.
[8]. Jajodia A, Sindhwani G, Pasricha S et al (2021) Application of the Kaiser score to increase diagnostic accuracy in equivocal lesions on diagnostic mammograms referred for MR mammography. Eur J Radiol 134:109413.
[9]. Avendano D, Marino MA, Leithner D et al (2019) Limited role of DWI with apparent diffusion coefficient mapping in breast lesions presenting as non-mass enhancement on dynamic contrast-enhanced MRI. Breast Cancer Res 21:136.
Figures
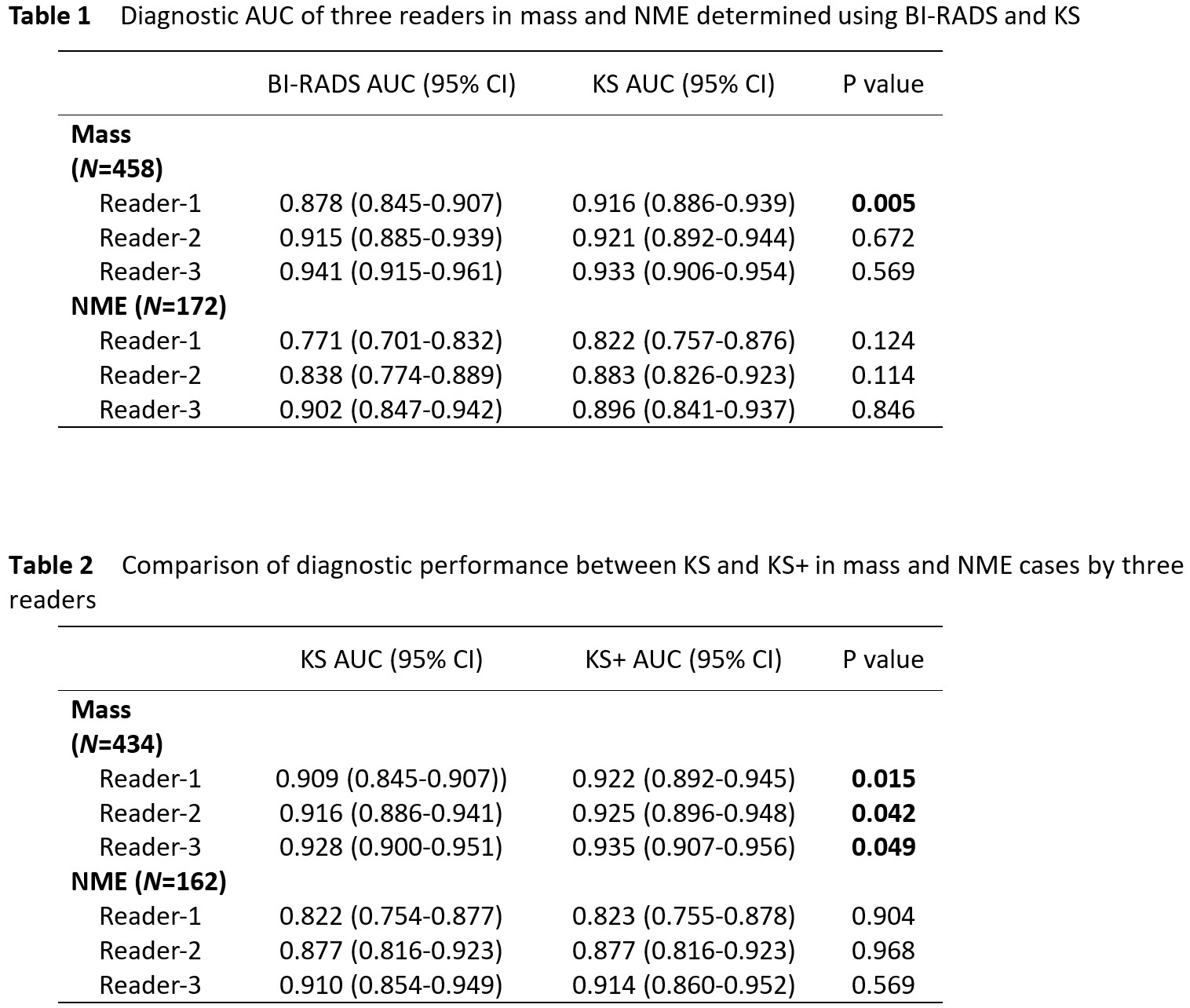
Table 1 Diagnostic AUC of three readers in mass and NME determined using BI-RADS and KS
Table 2 Comparison of diagnostic performance between KS and KS+ in mass and NME cases by three readers