4613
The Optimal Timepoint for Lesion depiction in Ultrafast DCE MRI: Correlation with lesion size and Invasive Breast Cancer Subtype1Diagnostic Imaging and Nuclear Medicine, Graduate School of Medicine Kyoto University, Kyoto, Japan, 2Department of Diagnostic Radiology, Kobe City Medical Center General Hospital, Kobe, Japan, 3Department of Diagnostic Radiology, Kansai Electric Power Hospital, Osaka, Japan, 4Breast Surgery, Graduate School of Medicine Kyoto University, Kyoto, Japan, 5Graduate School of Medicine Kyoto University, Kyoto, Japan
Synopsis
Keywords: Breast, Breast, ultrafast DCE MRI
Motivation: To know the factors affecting optimal timing of lesion evaluation in ultrafast (UF)- DCE MRI other than BPE.
Goal(s): To investigated the optimal timing for lesion depiction on UF-DCE MRI in relation to lesion size and invasive breast cancer subtype.
Approach: Optimal timing of lesion evaluation over 400 lesions were assessed by experienced readers. Its association with lesion size and subtype were examined.
Results: Optimal timing of breast lesion evaluation on UF-DCE MRI can be earlier for those with larger lesion, and not affected by subtype in case of invasive carcinoma.
Impact: UF-DCE MRI normally involves hundreds of images with multiple timing. Predicting optimal timing before scanning may help in efficient reading, efficient post-processing/reconstruction, and protocol improvement. The current results indicate the impact of lesion size, not subtype on optimal timing.
Introduction and Purposes
Ultrafast Dynamic contrast MRI (UF-DCE MRI) is becoming a useful addition or alternative to conventional DCE MRI due to its ability to selectively depict the target hypervascular lesions. Avoidance of marked background parenchymal enhancement (BPE) is a clinical benefit for using UF-DCE MRI. However, there is no consensus on the ideal scan time frame or scan timing for the best depiction, which may be affected by various factors associated with individual lesions including lesion size and invasive breast cancer subtype. Knowing optimal timing may help in efficient reading and protocol improvement. Therefore, we investigated the optimal timing for lesion depiction on UF-DCE MRI in relation to lesion size and invasive breast cancer subtypes.Materials and Methods
Study population: Inclusion criteria are patients who underwent UF-DCE MRI at our hospital from 2018 to 2021, had at least one enhanced lesion suspected of malignancy with information of measurable enhanced timing. For subtype analysis, those with histopathologically confirmed invasive carcinoma (no special type and invasive lobular carcinoma) were included. MRI protocol: MRI was acquired using a 3T MRI scanner (Prisma; Siemens Healthineers, Erlangen, Germany) and a 18-channel dedicated breast coil. The UF-DCE protocol used a 3D gradient-echo VIBE with compressed sensing. UF-DCE acquisitions were obtained using a prototype sequence based on the 3D gradient-echo VIBE sequence at a very early phase, with TR/TE 5.0/2.5, FA 15, FOV 360 mm×360 mm, matrix 384x269, thickness 2.5 mm ,CS acceleration=16.5. CS reconstruction was conducted with 30 iterations. Gadobutrol was injected at 2 ml/s. UF-DCE MRI (from 15 sec before to 60 sec after contrast injection, 2 sec preparation time followed by 3.65 sec/frame x 20 frames) were obtained. Axial subtracted MIP images (2nd -20th frames) were computed. Image analysis: An experienced breast radiologist evaluated the serial MIP images and evaluated the first frames of optimal lesion evaluation. The frame number is used as a proxy to time (sec) from the contrast injection. lesion size was also recorded. Statistical analysis: Lesion size were categorized into four : group 0: ≤10mm, group 1: >10mm and ≤20mm, group 2: >20mm and ≤50mm, and group 3: >50mm. Correlation between lesion size and the above timings (number of frames) were examined using trend test. P value of 0.05 was used as a criteria of significance.Results
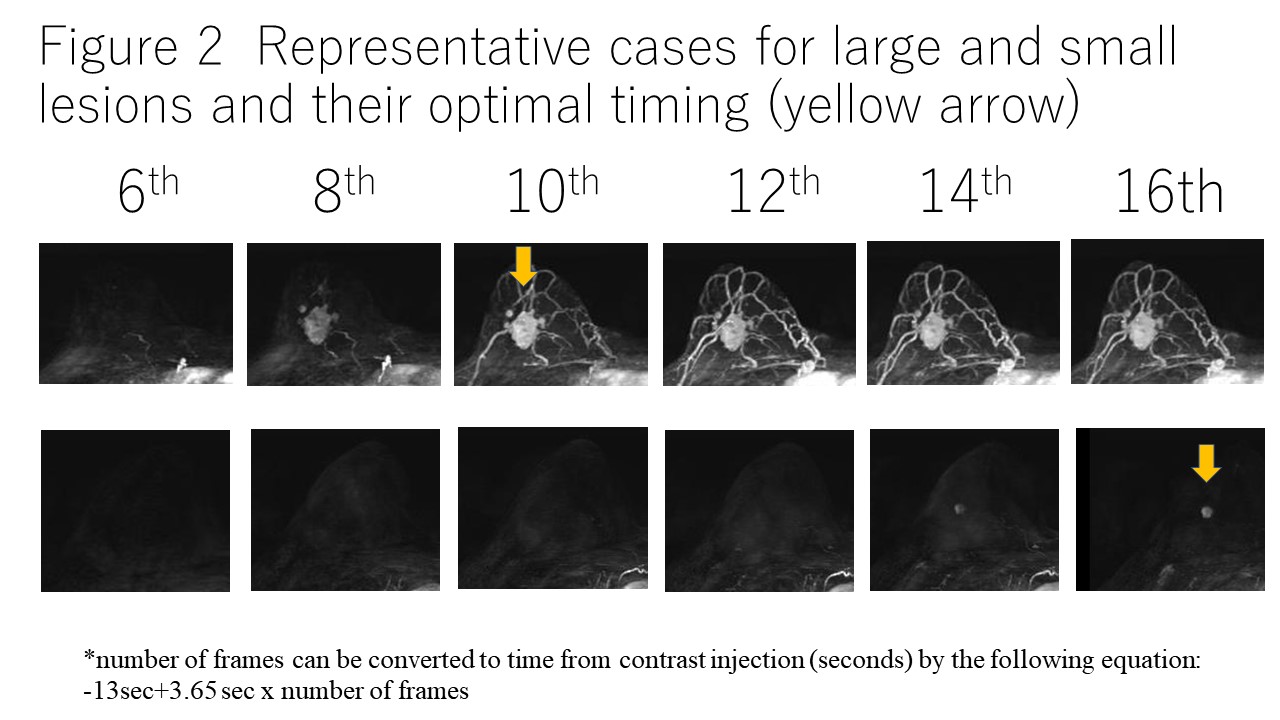
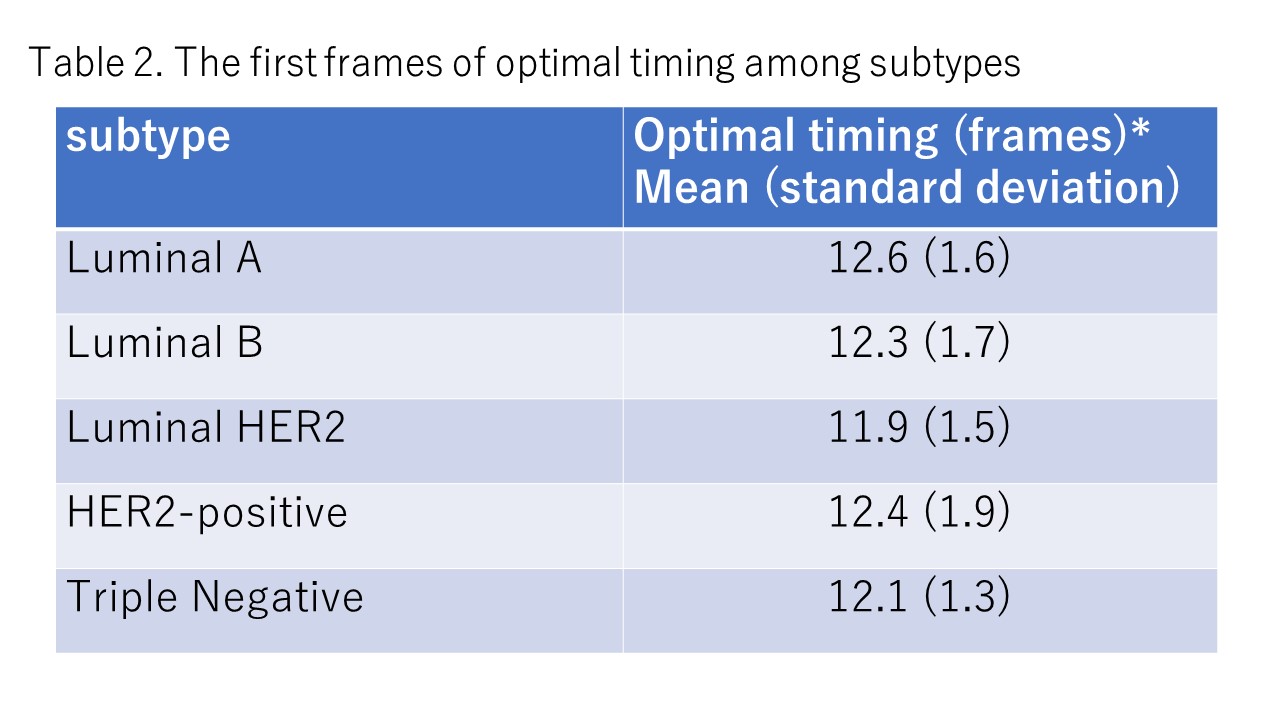
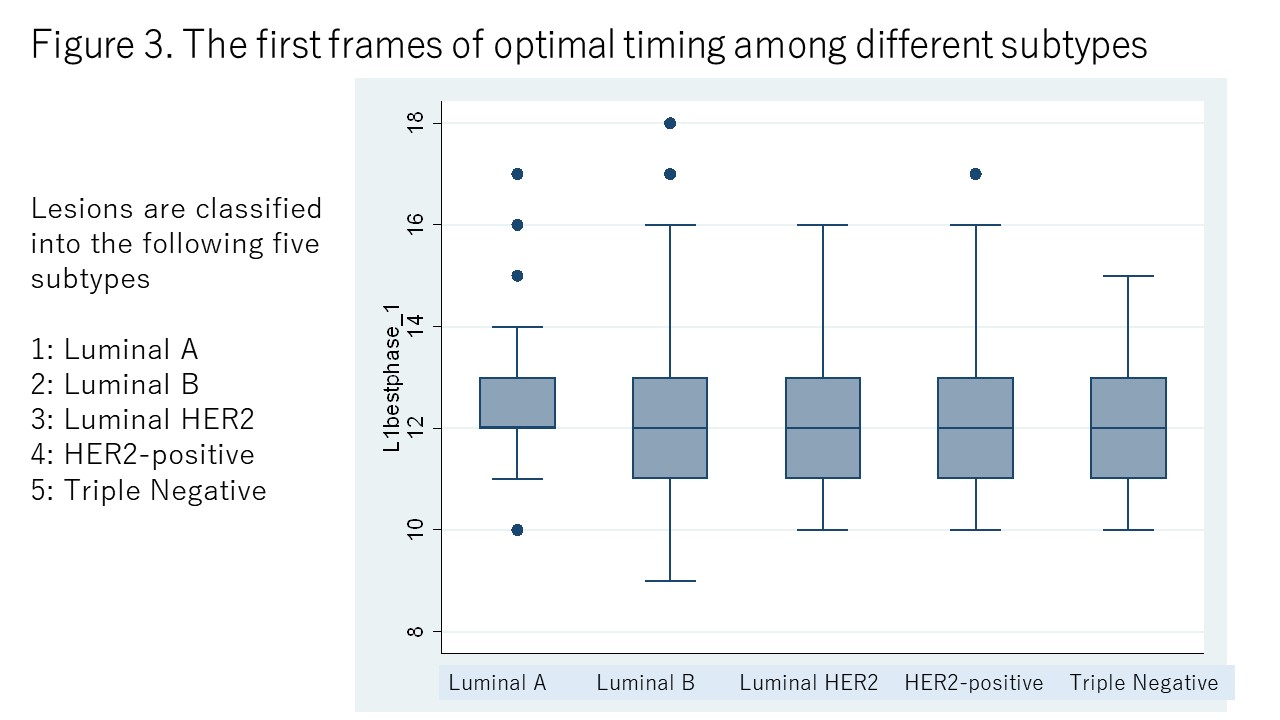
In total 402 patients (mean age 56 years) with pathologically confirmed 282 patients with invasive carcinoma ( 91 luminal A, 102 luminal B, 18 luminal-HER2, 21 HER2-positive, and 50 triple negative subtypes) were included. Lesion size and timing: Average timing per each group are shown in table 1. There was a trend of earlier timing for larger lesions for the first frames of optimal lesion evaluation (p= 0.004) (Figure 1). A representative figure is shown in figure 2. Subtype and timing: There was no significant difference in timing among groups with different invasive carcinoma subtypes for the first frames of optimal lesion evaluation. (Table 2) (Figure 3)Discussions and Conclusions
Optimal timing of breast lesion evaluation on UF-DCE MRI can be earlier for those with larger lesion, later for those with smaller lesion. Adjustment of scanning and reconstruction protocol by lesion size may be useful. There was no significant difference in optimal timing among different subtypes of invasive carcinoma, indicating that there was no need to modify the UF-DCE protocol according to subtype.Acknowledgements
NoneReferences
1. Honda M et al. EJR 2020 2. Kataoka M et al. MRMS 2022Figures
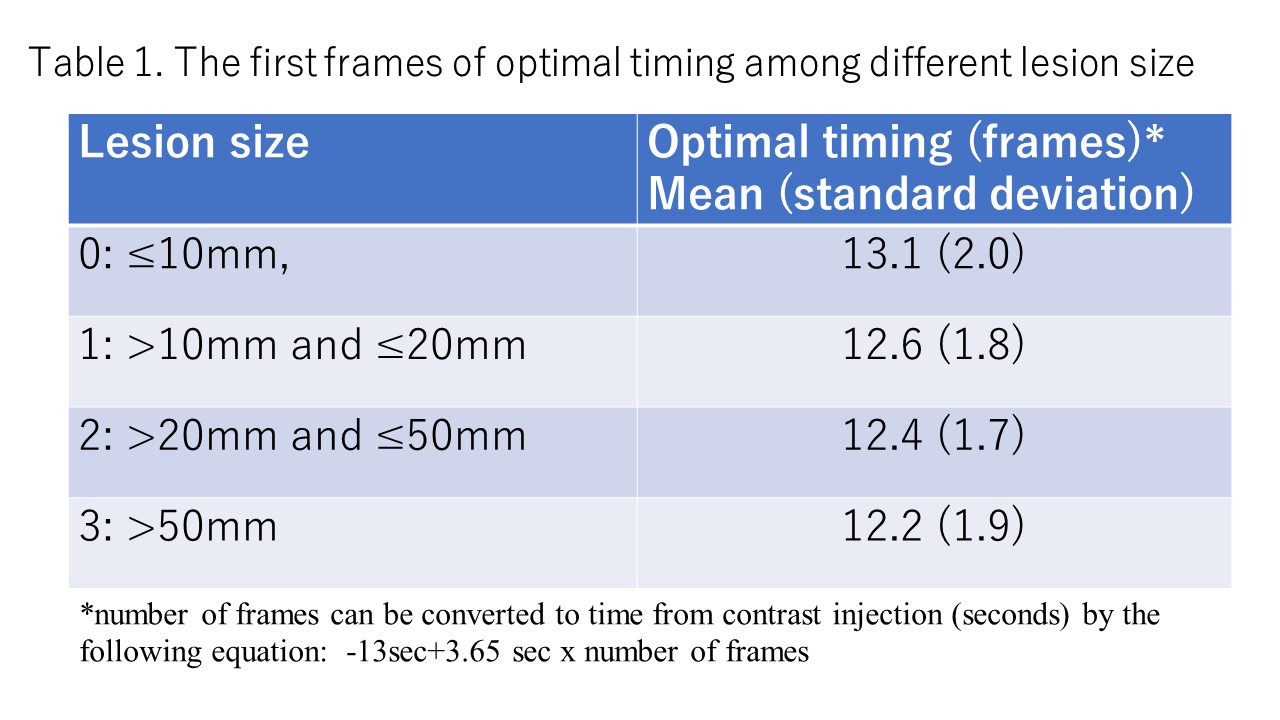
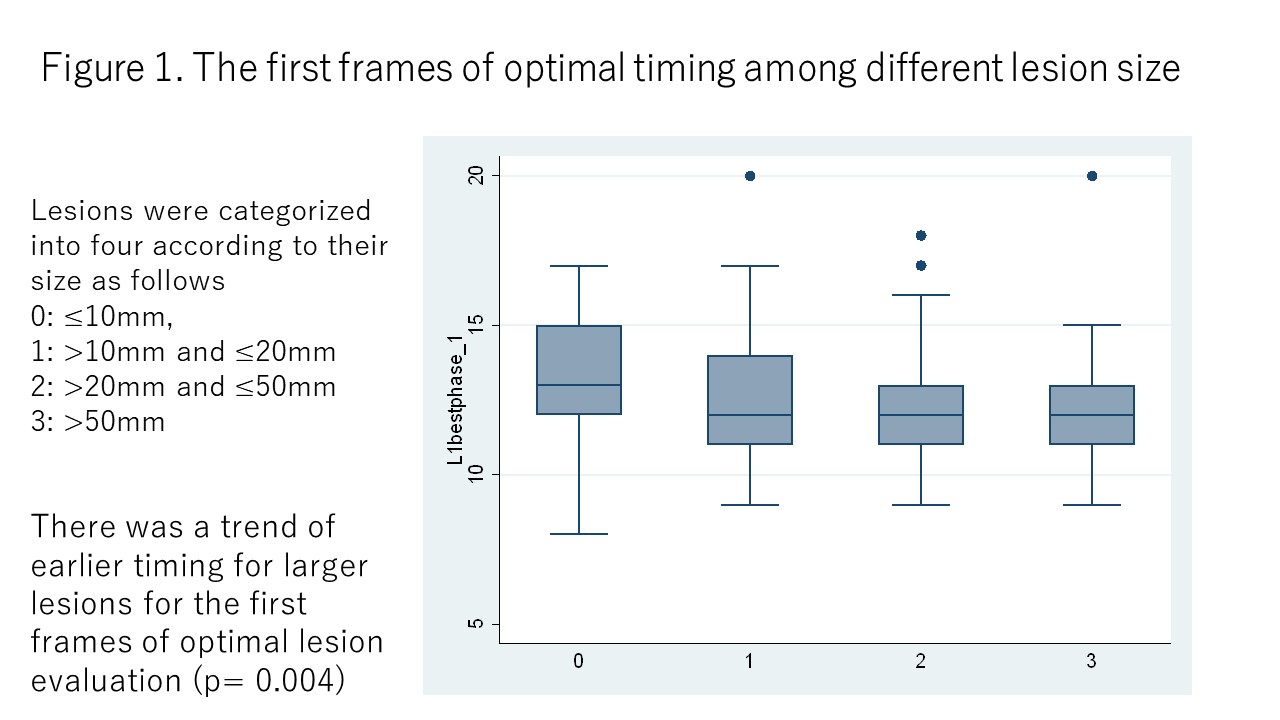
Figure 1. The first frames of optimal timing among different lesion size
Lesions were categorized into four according to their size as follows 0: ≤10mm, 1: >10mm and ≤20mm 2: >20mm and ≤50mm 3: >50mm