4612
Radiomics nomogram based on ultrafast DCE-MRI and DWI: preoperative evaluation of axillary lymph node status in invasive breast cancer1Department of Radiology, Fujian Medical University Union Hospital, Fuzhou, Fujian, China, 2GE Healthcare, Beijing, China
Synopsis
Keywords: Breast, Breast
Motivation: Accurately evaluating the ALN status is pivotal for both prognosis and treatment planning, especially in the context of decreasing axillary surgery.
Goal(s): This retrospective study aimed to develop a radiomics nomogram for preoperative prediction of ALN status in clinical T1-2 stage invasive breast cancer patients.
Approach: Radiomics features were extracted from ultrafast DCE-MRI and DWI, and clinical characteristics were incorporated to construct a radiomics nomogram.
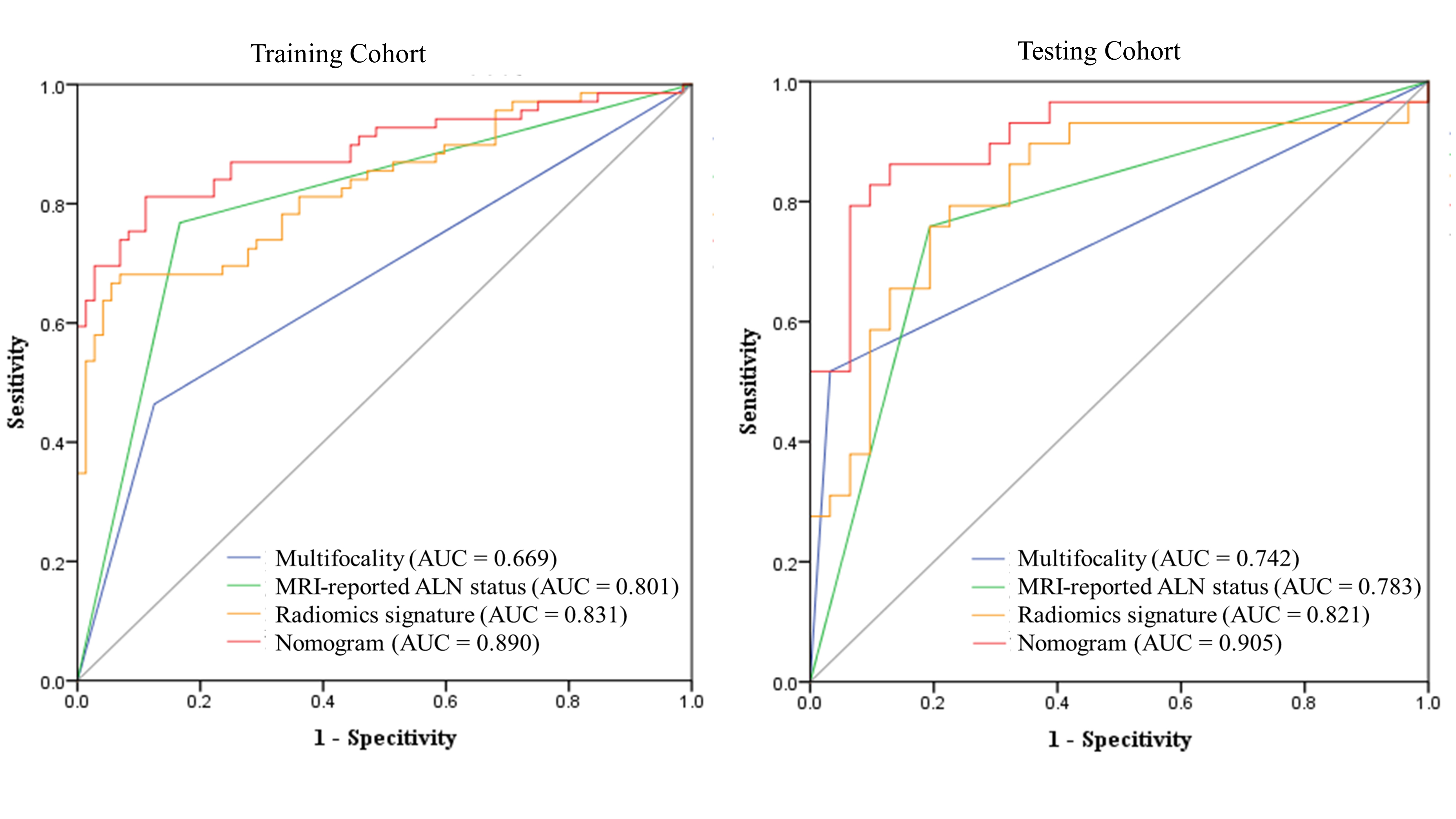
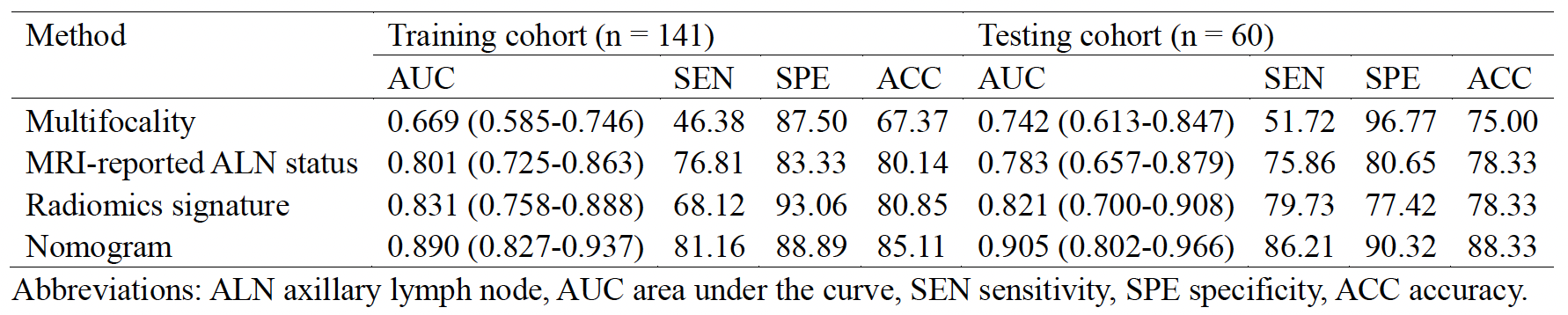
Results: A radiomics signature achieved AUCs of 0.831 and 0.821 in training and validation cohorts, respectively. The radiomics nomogram, incorporating this signature, multifocality, and MRI-reported ALN status, showed superior performance with AUCs of 0.890 and 0.905.
Impact: The proposed nomogram could be valuable for noninvasively assessing ALN status, aiding prognosis and treatment planning while reducing the need for axillary surgery in breast cancer patients.
Introduction
Axillary lymph node (ALN) metastasis plays a pivotal role in breast cancer prognosis and treatment decisions, significantly affecting patient survival1. Those with ALN metastasis experience a 40% reduction in the 5-year overall survival rate compared to those without2. Sentinel lymph node biopsy (SLNB) is the standard approach for ALN staging in clinically ALN-negative patients, reducing invasiveness and yielding outcomes similar to ALN dissection (ALND)3. However, SLNB is invasive and time-consuming due to frozen section analysis, making a noninvasive ALN staging method highly desirable. Noninvasive imaging techniques are promising for assessing ALN status4-7. DCE-MRI offers both morphological and kinetic information, but traditional analysis relies on delayed-phase enhancement, prolonging the procedure8. Ultrafast DCE-MRI provides rapid perfusion quantification and has been shown to yield accurate quantitative parameters in a clinical setting within 120 seconds, making it a practical alternative to assess breast lesions9-12. Therefore, ultrafast DCE-MRI could streamline quantitative analysis and potentially replace the lengthier standard DCE-MRI13. DWI provides insights into tumor cellularity and is an independent predictor of ALN metastasis5. Radiomics, an emerging approach in precision medicine for breast cancer, enables quantitative analysis of tumor heterogeneity by mining high-dimensional features from the entire tumor14,15. However, a combined radiomics model integrating quantitative ultrafast DCE-MRI and DWI parameters for predicting ALN metastasis has not been established. This study aimed to develop and validate a nomogram based on MRI, integrating radiomics signatures from ultrafast DCE-MRI and DWI quantitative maps with clinical risk factors to predict ALN involvement in patients with clinical T1-2 stage breast cancer.Materials and Methods
This study was approved by the institutional review board of our hospital. A total of 201 patients with invasive breast cancer at clinical T1-2 stage were included. All patients underwent breast MRI on a 3T MRI system (SIGNA Pioneer; GE Healthcare, Milwaukee, WI) with a comprehensive protocol that included T2WI, MUSE DWI, and ultrafast DCE-MRI DISCO with 26 phases. Standard DCE-MRI was also acquired using VIBRANT sequence with 4 phases. Breast MRI analysis was conducted by an experienced radiologist according to ACR BI-RADS. Various image features were evaluated. Ultrafast DCE-MRI images were processed using GenIQ software on Advantage Workstation 4.7 (GE Healthcare) to correct for motion, obtain individual AIF, and generate quantitative Ktrans, Kep, and Ve maps. MUSE DWI images were processed using monoexponential fitting to generate ADC maps. A 3D ROI was semiautomatically delineated on DCE-MRI images and transferred to quantitative maps. A total of 354 radiomics features were extracted. Normalization, intra-class correlation coefficient analysis, Pearson correction coefficient analysis, and feature selection were performed to construct SVM model. Clinical, histologic, MRI, and radiomics features related to ALN metastasis were examined through univariate and multivariate logistic analysis to construct a nomogram. Chi-square tests, logistic regression, variance inflation factor assessment, and ROC analysis were used to evaluate the clinical, radiomics, and nomogram prediction models' performance.Results
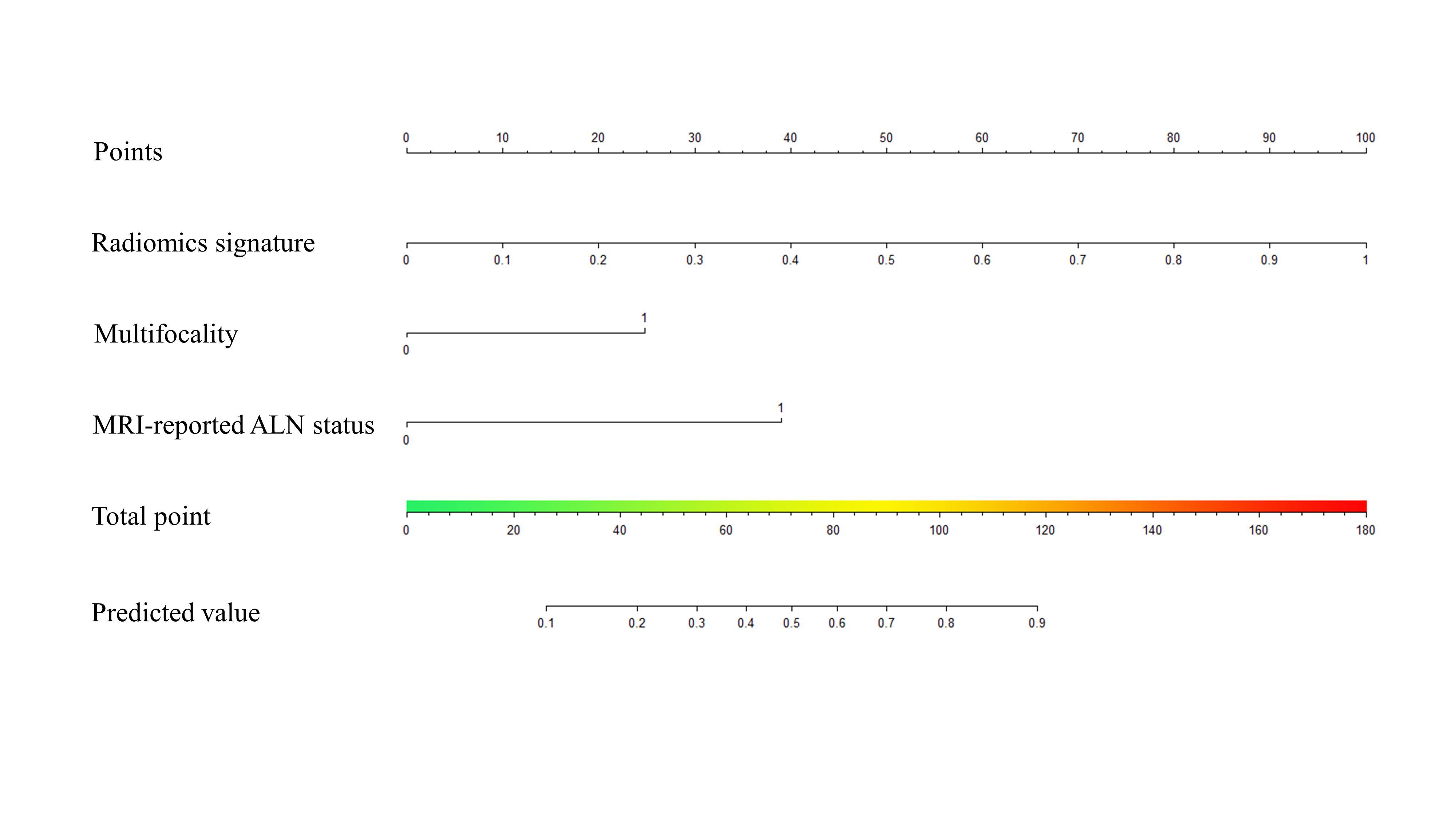
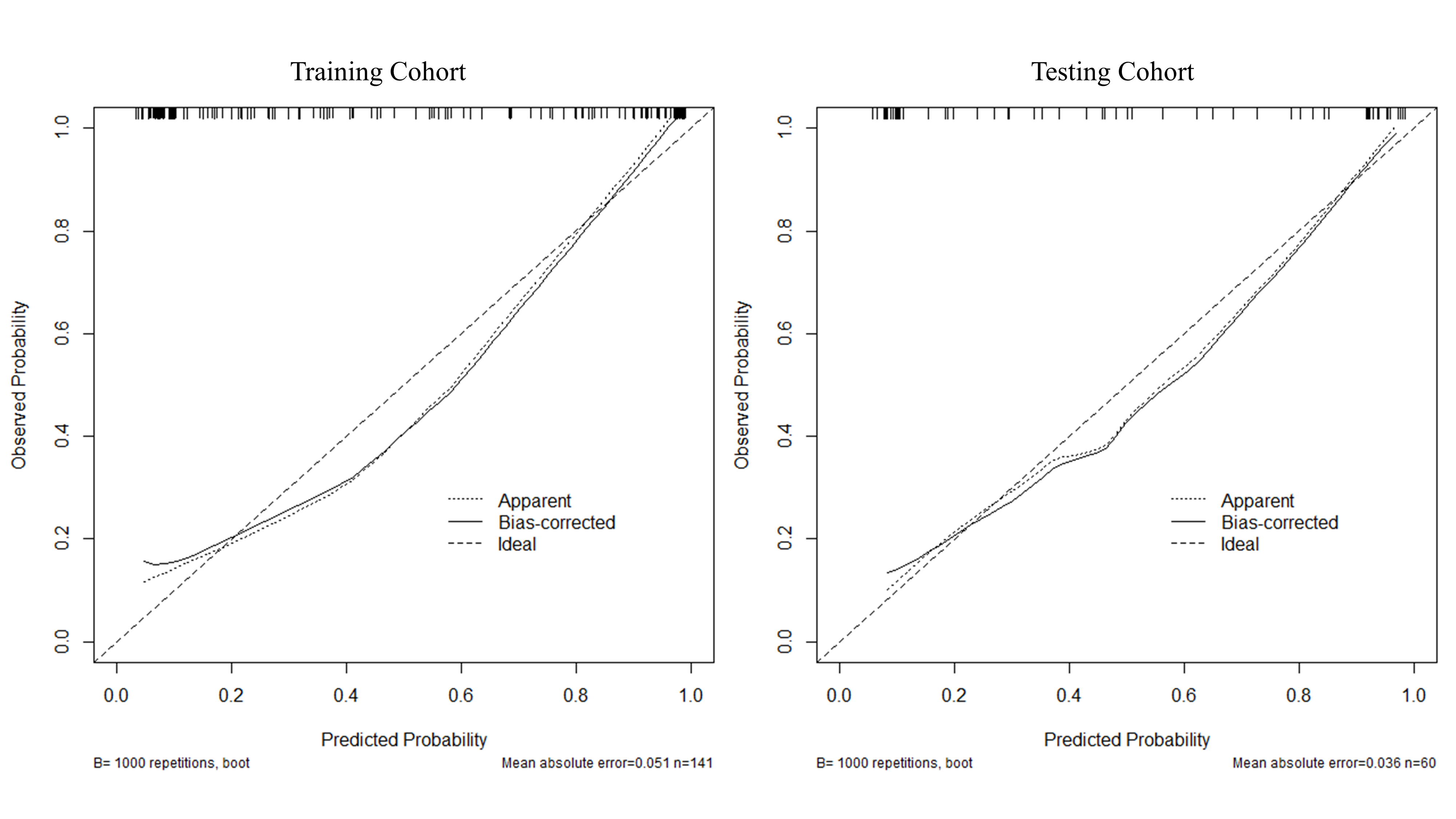
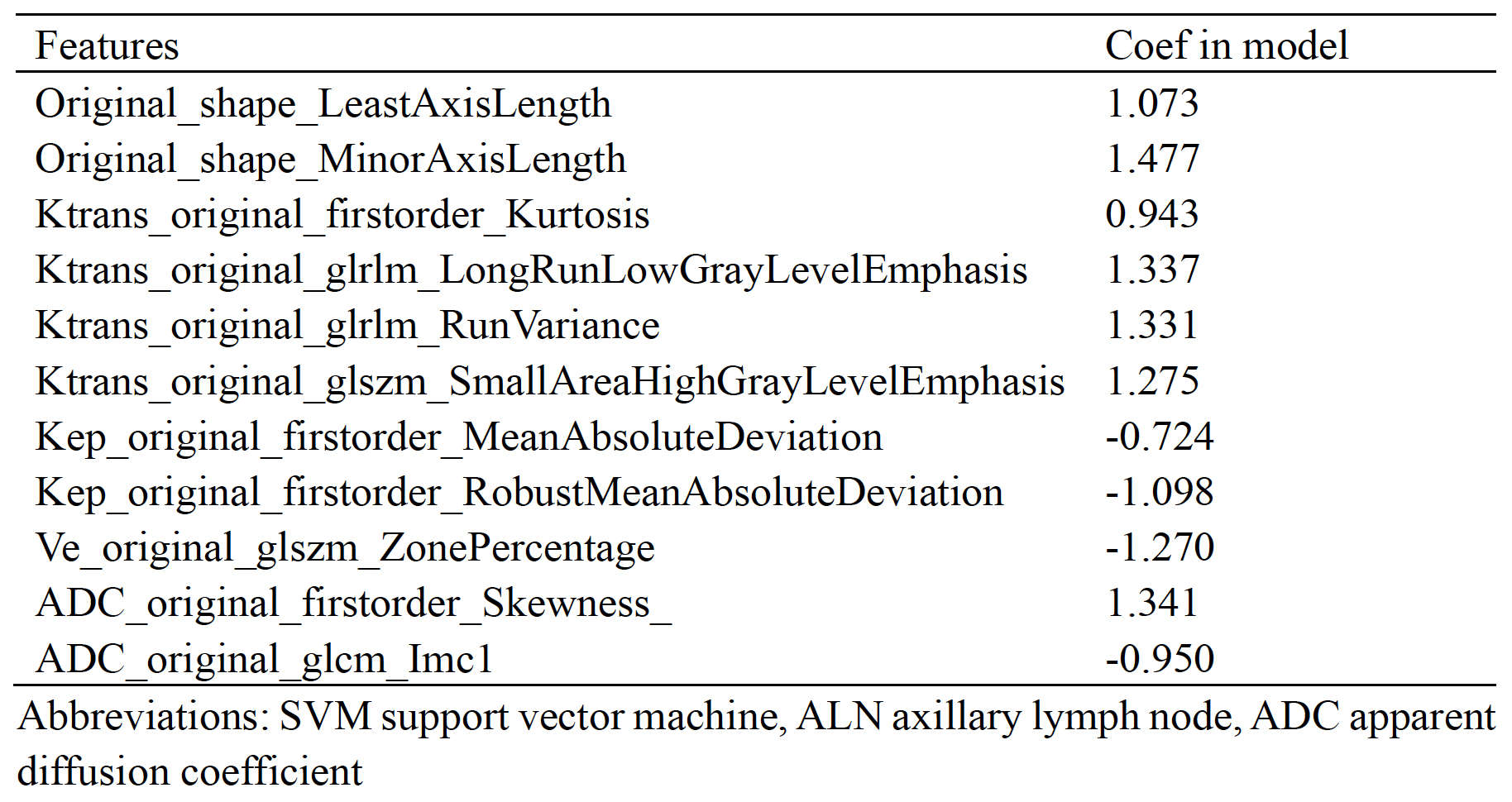
98 (48.76%) patients were confirmed to have ALN metastasis. ALN metastasis was associated with higher clinical T stage and Ki-67 index. Imaging features, such as multifocality, shape, margin, enhancement, edema, and MRI-reported ALN status, also significantly differed between two groups. From the combined quantitative maps, 11 optimized radiomics features were selected in the training group to establish the SVM model (Table 1). These radiomics features exhibited strong predictive performance with AUCs of 0.831 in training cohort and 0.821 in testing cohort (Table 2). The radiomics signature showed high specificity, reaching 93.06% in training cohort and 77.42% in testing cohort, with lower sensitivity at 68.12% and 79.73% in training and testing cohorts, respectively. 10 significant predictors, including clinical-histologic variables (clinical T stage and Ki-67 index), imaging features (multifocality, shape, margin, enhancement, MRI-reported ALN status), and radiomics signature, were identified. In the multivariate regression model, multifocality, edema, MRI-reported ALN status, and radiomics signature were independent predictors of ALN metastasis. A nomogram was constructed based on multifocality, MRI-reported ALN status, and radiomics signature (Figure 1). The nomogram demonstrated superior discrimination ability compared to clinical and radiomics signature models, with higher AUCs of 0.890 and 0.905 in training and testing cohorts, respectively (Figure 2). The Hosmer-Lemeshow test on the calibration curve yielded non-significant results, indicating good calibration (Figure 3).Discussion
Our study demonstrated that radiomics features from ultrafast DCE-MRI and DWI quantitative maps can serve as potential biomarkers for ALN metastasis prediction. The developed nomogram, combining radiomics signature, multifocality, and MRI-reported LN status, displayed the highest discriminative capacity. This approach offered a valuable tool for predicting ALN status in patients with clinical T1-2 stage invasive breast cancer.Acknowledgements
No acknowledgement found.References
1. Ahmed, M., A.D. Purushotham, and M. Douek, Novel techniques for sentinel lymph node biopsy in breast cancer: a systematic review. Lancet Oncol, 2014. 15(8): p. e351-62.
2. Danko, M.E., et al., Improved staging in node-positive breast cancer patients using lymph node ratio: results in 1,788 patients with long-term follow-up. J Am Coll Surg, 2010. 210(5): p. 797-805 e1, 805-7.
3. Krag, D.N., et al., Sentinel-lymph-node resection compared with conventional axillary-lymph-node dissection in clinically node-negative patients with breast cancer: overall survival findings from the NSABP B-32 randomised phase 3 trial. Lancet Oncol, 2010. 11(10): p. 927-33.
4. Chen, S.T., et al., Diagnostic accuracy of pre-operative breast magnetic resonance imaging (MRI) in predicting axillary lymph node metastasis: variations in intrinsic subtypes, and strategy to improve negative predictive value-an analysis of 2473 invasive breast cancer patients. Breast Cancer, 2023.
5. Xue, M., et al., Nomogram Based on Breast MRI and Clinicopathologic Features for Predicting Axillary Lymph Node Metastasis in Patients with Early-Stage Invasive Breast Cancer: A Retrospective Study. Clin Breast Cancer, 2022. 22(4): p. e428-e437.
6. Carriero, A., et al., Maximum intensity projection analysis in magnetic resonance of the breast. J Exp Clin Cancer Res, 2002. 21(3 Suppl): p. 77-81.
7. Zhao, M., et al., Magnetic resonance imaging features for predicting axillary lymph node metastasis in patients with breast cancer. Eur J Radiol, 2020. 129: p. 109093.
8. Kuhl, C.K., et al., Dynamic breast MR imaging: are signal intensity time course data useful for differential diagnosis of enhancing lesions? Radiology, 1999. 211(1): p. 101-10.
9. Gao, Y. and S.L. Heller, Abbreviated and Ultrafast Breast MRI in Clinical Practice. Radiographics, 2020. 40(6): p. 1507-1527.
10. Jena, A., S.B. Mehta, and S. Taneja, Optimizing MRI scan time in the computation of pharmacokinetic parameters (K(trans) ) in breast cancer diagnosis. J Magn Reson Imaging, 2013. 38(3): p. 573-9.
11. Hao, W., et al., Influence of scan duration on the estimation of pharmacokinetic parameters for breast lesions: a study based on CAIPIRINHA-Dixon-TWIST-VIBE technique. Eur Radiol, 2015. 25(4): p. 1162-71.
12. Aerts, H.J., K. Jaspers, and W.H. Backes, The precision of pharmacokinetic parameters in dynamic contrast-enhanced magnetic resonance imaging: the effect of sampling frequency and duration. Phys Med Biol, 2011. 56(17): p. 5665-78.
13. Milon, A., et al., Abbreviated breast MRI combining FAST protocol and high temporal resolution (HTR) dynamic contrast enhanced (DCE) sequence. Eur J Radiol, 2019. 117: p. 199-208.
14. Yu, Y., et al., Development and Validation of a Preoperative Magnetic Resonance Imaging Radiomics-Based Signature to Predict Axillary Lymph Node Metastasis and Disease-Free Survival in Patients With Early-Stage Breast Cancer. JAMA Netw Open, 2020. 3(12): p. e2028086.
15. Chen, M., et al., Development and validation of convolutional neural network-based model to predict the risk of sentinel or non-sentinel lymph node metastasis in patients with breast cancer: a machine learning study.EClinicalMedicine, 2023. 63: p. 102176.
Figures