4610
Predicting response to neoadjuvant chemotherapy in breast cancer by biomechanics quantified with Magnetic Resonance Elastography.1School of Cancer and Pharmaceutical Sciences, King’s College London, London, United Kingdom, 2Guy’s and St Thomas Foundation Trust NHS, London, United Kingdom, 3King's College Hospital NHS Foundation Trust, London, United Kingdom, 4School of Biomedical Engineering & Imaging Sciences, King’s College London, London, United Kingdom, 5LVTS, Inserm U1148, University Paris Diderot, Paris, France
Synopsis
Keywords: Breast, Cancer, Breast, Response, Chemotherapy
Motivation: To achieve de-escalation of surgery in breast cancer patients having complete response after primary chemotherapy, we require better accuracy than the current gold standard DCE-MRI, which has a sensitivity of 80-90% and a specificity of 37-97%.
Goal(s): Investigate the diagnostic value of biomechanical imaging biomarkers quantified via MR-Elastography (MRE) for gauging complete pathological response non-invasively.
Approach: Incorporate MRE into standard Breast MRI protocol for NACT patients within standard-of-care MRI protocol.
Results: Biomechanical changes in conjunction with DCE MRI improved sensitivity to 94.4% and specificity to 95.7%, making this approach a promising new concept to predict complete response after NACT.
Impact: Quantifying biomechanics throughout chemotherapy via MR-Elastography (MRE) in conjunction with DCE-MRI in breast cancer patients undergoing primary chemotherapy yields more accurate results in predicting complete pathological response than current international imaging gold standard methods.
Background
Patients with breast cancer undergoing neoadjuvant chemotherapy (NACT) are monitored using Magnetic Resonance Imaging (MRI) with Dynamic Contrast Enhancement (DCE) as the gold-standard imaging technique to assess tumour response.MRI has a sensitivity of 80-90% and a specificity of 37-97%(1–3). Therefore, it is essential to identify alternative, non-invasive imaging biomarkers which show promise in identifying tissue alterations related to mechanisms of response to neoadjuvant chemotherapy (4).
We investigate the hypothesis whether biomechanics quantified over time via MR-Elastography (MRE) can identify complete pathological response in patients undergoing NACT and potentially predict response at an earlier timepoint throughout NACT.
Method
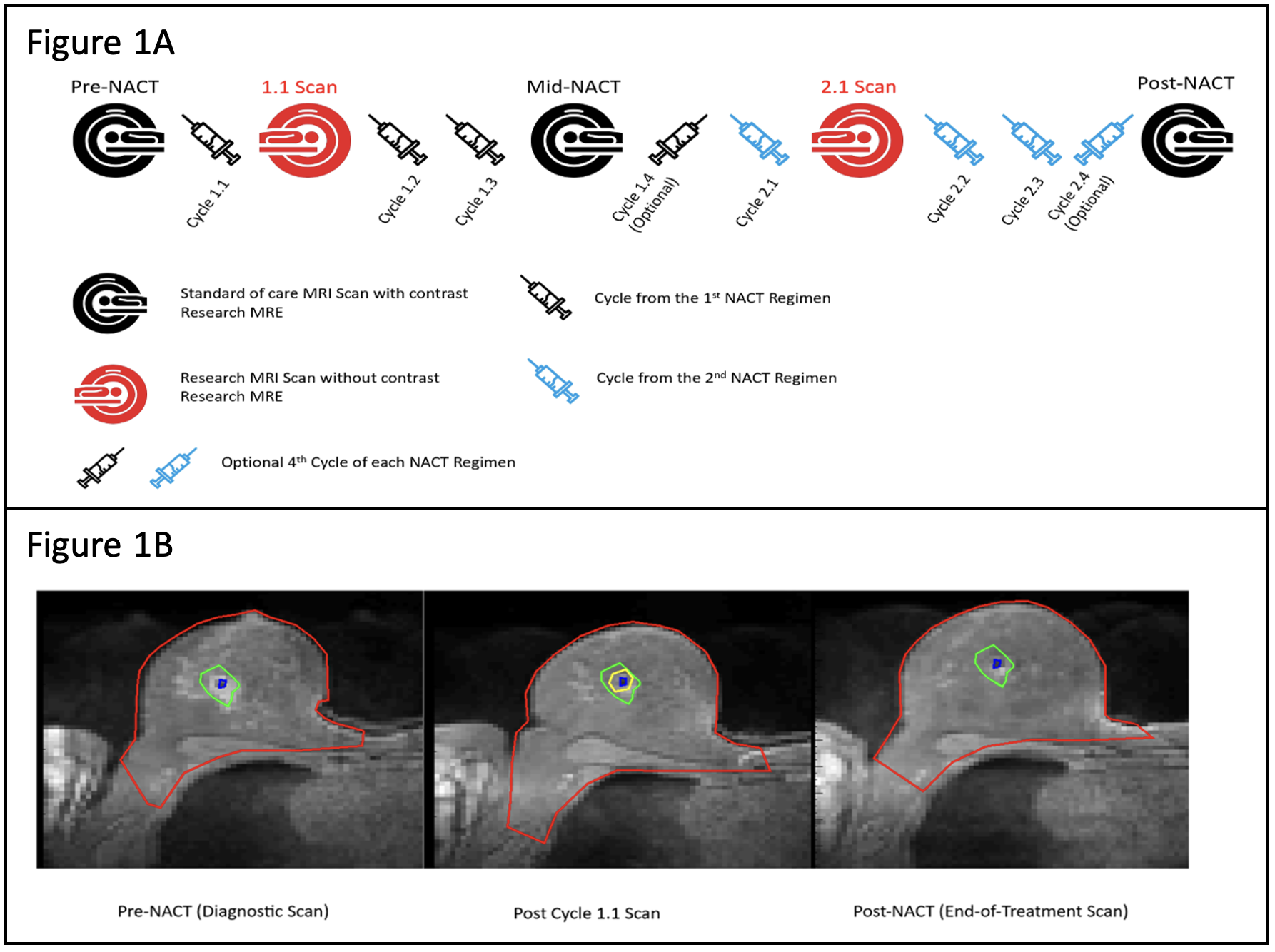
The gravitational MRE driver concept (5) was incorporated into the biopsy coil (SIEMENS) for seamless integration of data acquisition within the standard clinical routine protocol for breast MRI. Data were acquired at a 1.5T system (AERA, SIEMENS Healthineers), throughout a 7mins scan using a 3D MRE GRE sequence (6), enabling the non-invasive quantification of tissue biomechanics (complex shear modulus) over 16 consecutive slices at 36Hz mechanical vibration with an isotropic spatial resolution of 3mm.Participating breast cancer patients undergoing NACT underwent MRE in addition to clinical scans illustrated in Figure 1A.
DCE and elastography findings were compared to the post-operative histopathology results. The ROI of the initial untreated tumour was identified on DCE pre-NACT images and referred to as the “footprint” of the tumour. Before the 1st scan, a localisation coil was implanted into the tumour which was used as a landmark in translating the “footprint” ROI over time (Figure 1B). Changes in biomechanics quantified within the footprint between pre-NACT and post-NACT were used to investigate the ability to identify a complete or partial histopathological response.
An additional research scan was performed after the first cycle of chemotherapy to investigate whether biomechanics could inform at an earlier timepoint about response. Here, the tumour was still clearly visible (unlike often at end-NACT). Therefore, an additional ROI was drawn for that very timepoint to precisely demarcate the tumour (Fig.1B, yellow ROI).
3D MRE allows to quantify the local elastic modulus (G’, [elasticity]) and the loss modulus (G”) of tissue. Furthermore, the phase angle (2/p*arctan[G”/G’]) reports the intrinsic balance between elastic and viscous properties, which has previously been reported as indicative of malignancy(7).
Results
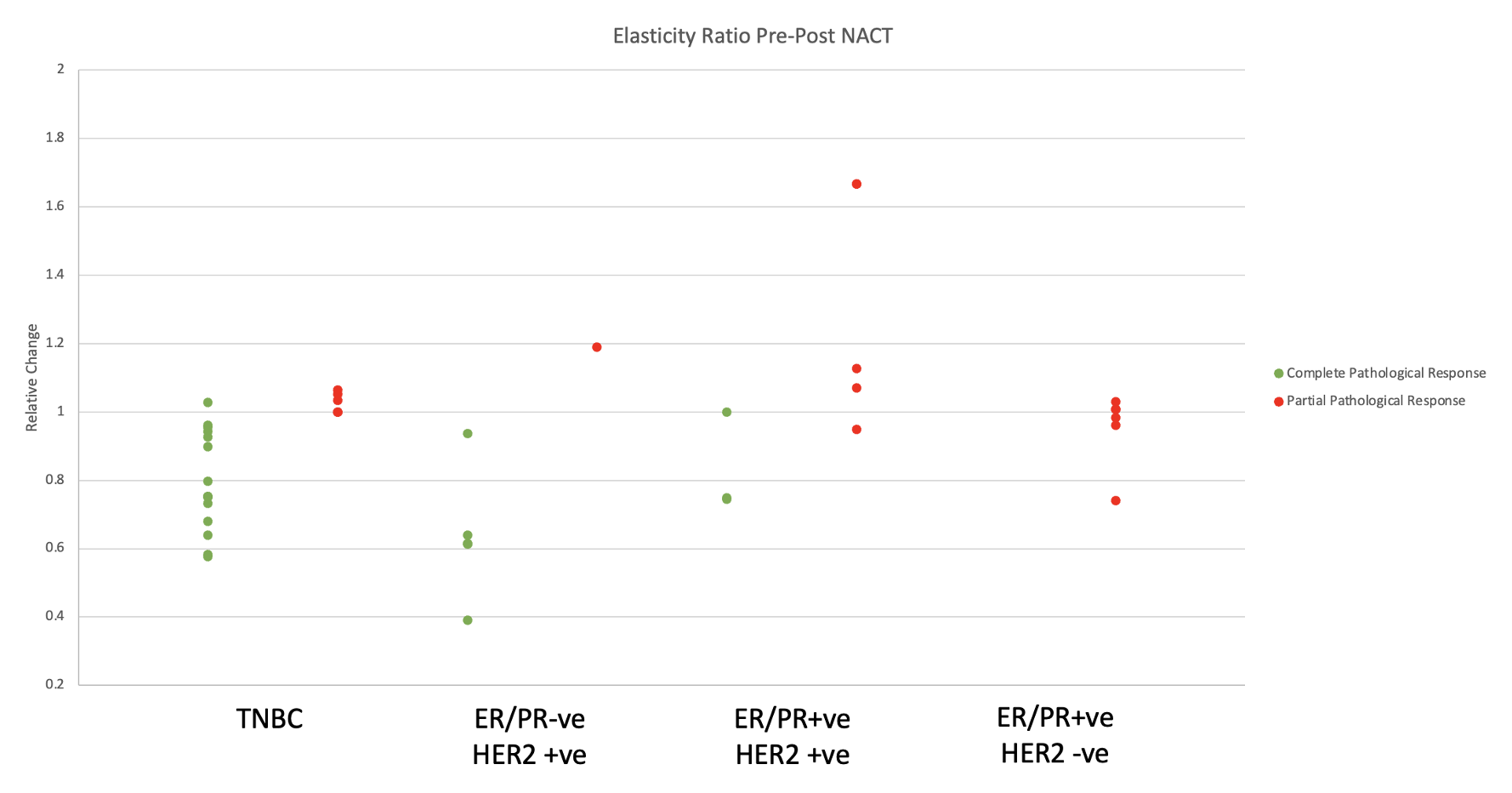
In all, forty-one patients – (205 individual scans) - were included in the analysis as they had completed their neoadjuvant chemotherapy and surgery and passed all data quality checks.Figure 2 shows the relative elasticity change within the footprint ROI between the diagnostic scan at the end-of-treatment and before treatment, i.e., Relative Elasticity = (Elasticity at Post-NACT/Elasticity at Pre-NACT). Patients with a complete pathological response showed a drop, whereas those with a partial response had a constant or increased elasticity. No correlation was seen in the viscosity at this time point which could potentially differentiating complete responders from partial responders. Pathological response depended on tumour type as expected, (Chi2 test – p=0.004), with a complete pathological response more likely in TNBC and HER2+/ERPR- breast cancer.
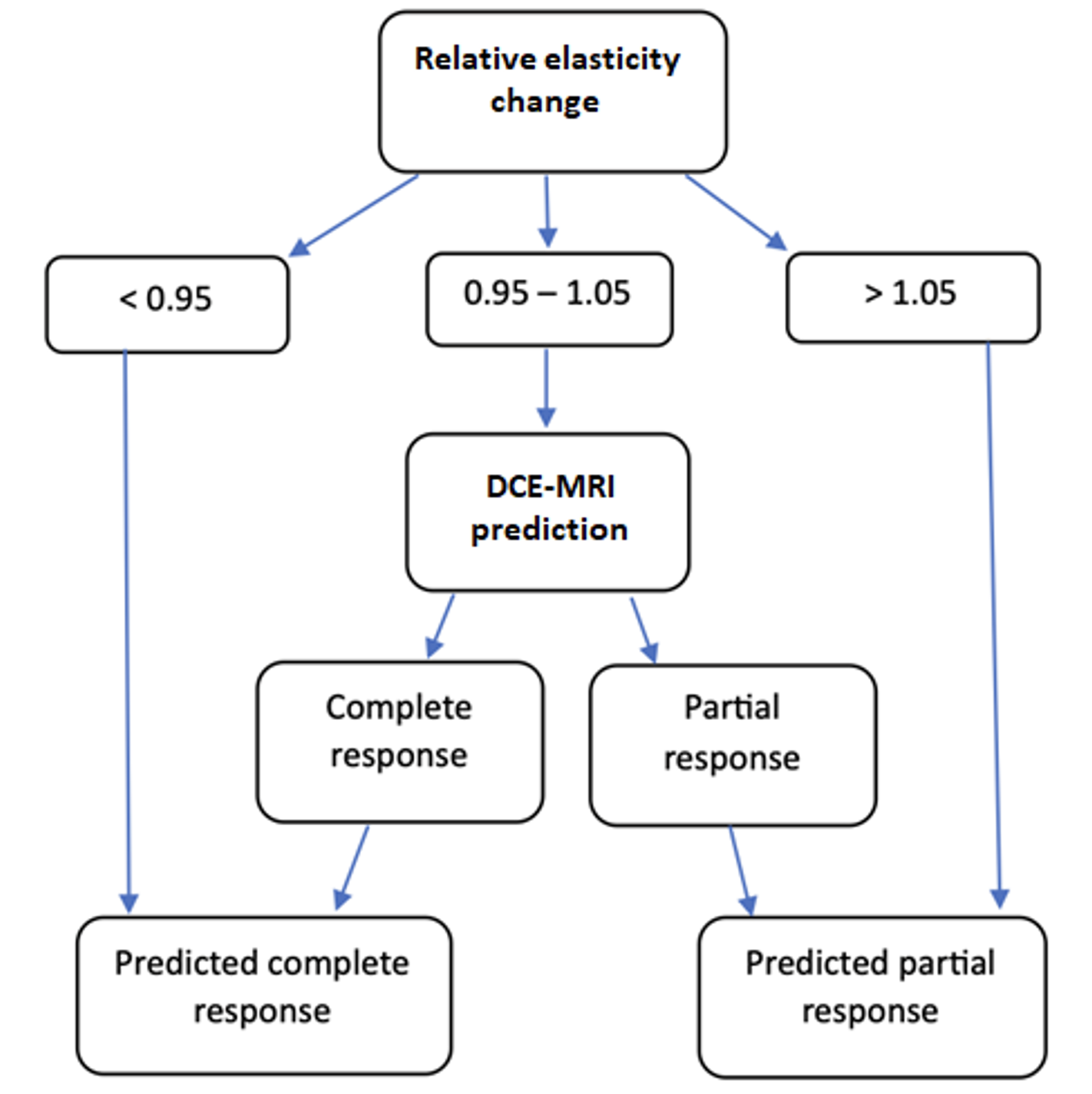
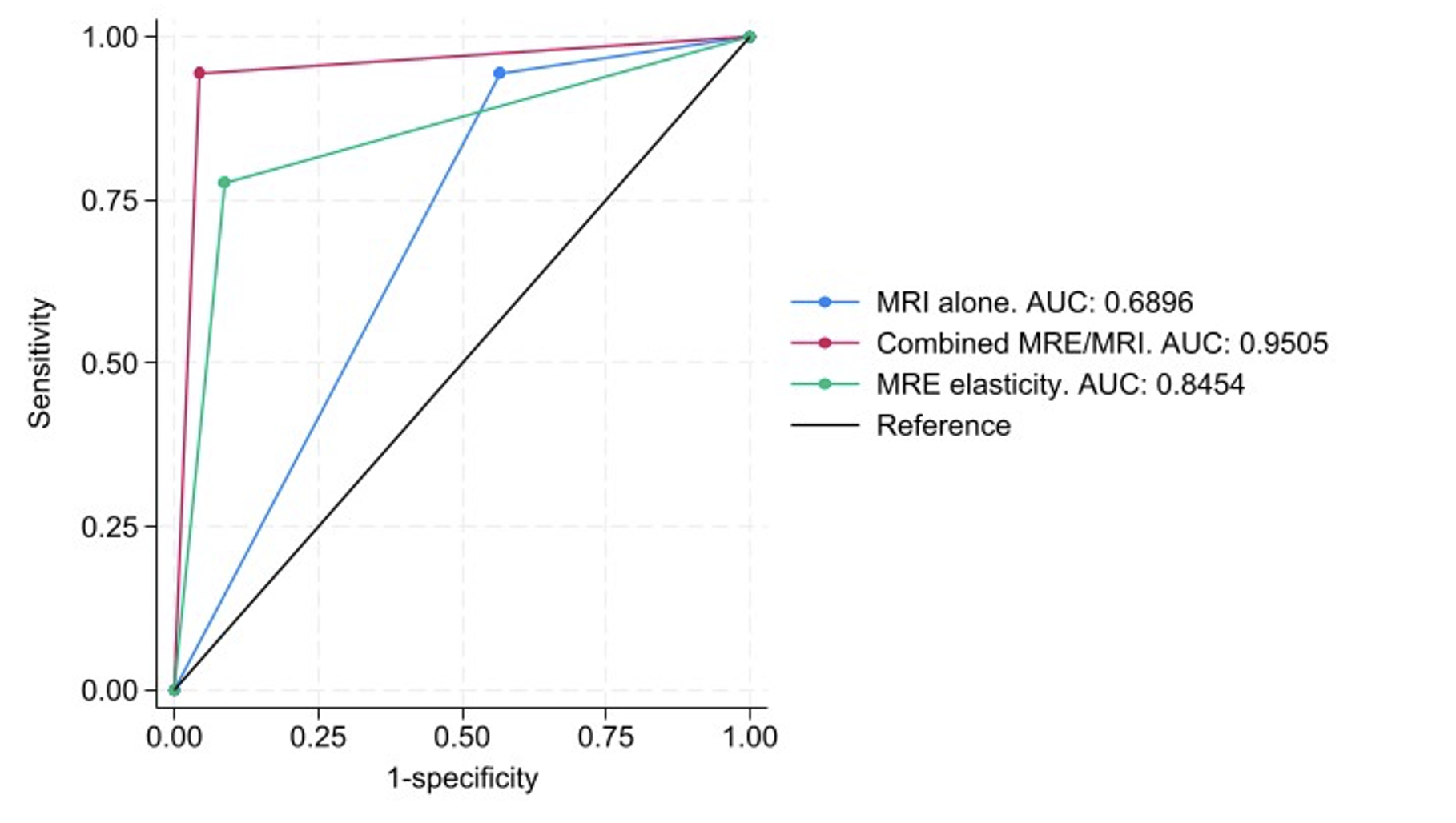
Relative elasticity was the most accurate individual predictor of histopathological response to treatment; however, it was not as sensitive as DCE-MRI. To investigate a combined biomarker approach, when the elasticity ratio was borderline (0.95-1.05), the decision tree in Figure 3 was used to predict whether patients had complete pathological responses. This concept improved sensitivity from 77.8% to 94.4%, whilst maintaining the high specificity of MRE alone (95.7% compared with 91.3%).
The combined approach yielded superior performance outperforming each individual approach indicative of the complementary information provided by both methods.
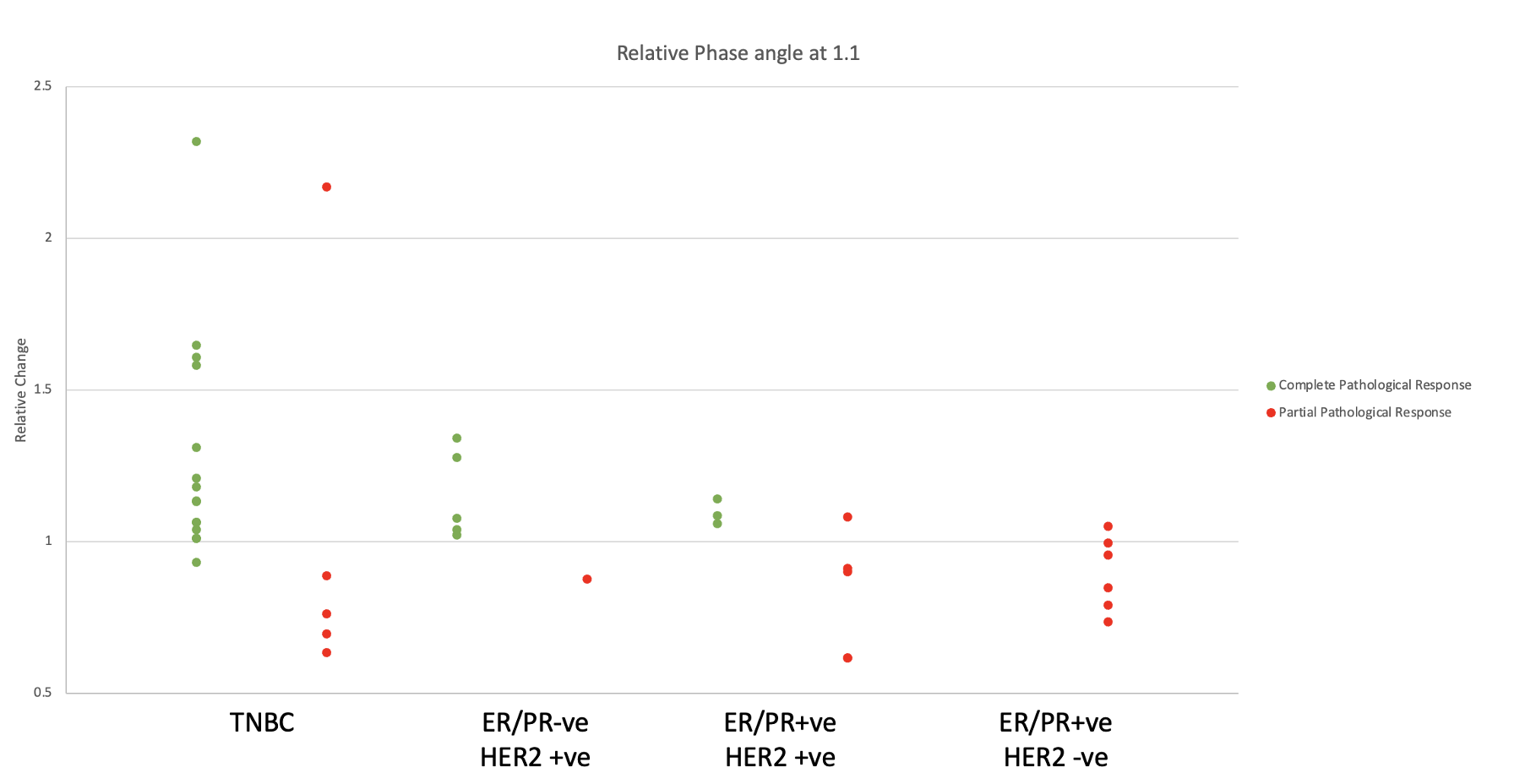
At the early timepoint 1.1 (Fig.1A) response/resistance correlated with a corresponding rise/drop in phase angle. It is important to remember that response/resistance is determined via histopathology at end-NACT. As such, it is intriguing that the relative change in phase angle carries such early predictive information (p<0.0001, Figure 5).
Conclusion
This study investigates the diagnostic value biomechanics can provide in the context of NACT for gauging response/resistance. Integrating MRE in a routine MRI scanner and using a combined biomarker approach (DCE+MRE) is promising to predict complete pathological response at the end of NACT in breast cancer patients. Although both DCE-MRI and MRE have good sensitivity and specificity individually, DCE-MRI and MRE combined have a sensitivity of 94.4% and a specificity of 95.7% in predicting complete pathological response, which could be a beneficial non-invasive diagnostic tool when considering de-escalation in surgery. Additionally, it was noted that the phase angle predicts early in the treatment cycle whether a patient will have a complete pathological response at the end of their treatment.Acknowledgements
Horizon Grant 2020
WellcomeLeap Grant 2022
Guy's Cancer Charity Grant 2023
References
1. Menezes GLG, Knuttel FM, Stehouwer BL, Pijnappel RM, Van Den Bosch MAAJ. Magnetic resonance imaging in breast cancer: A literature review and future perspectives. World J Clin Oncol [Internet]. 2014 May 10 [cited 2023 Oct 18];5(2):61–70. Available from: https://pubmed.ncbi.nlm.nih.gov/24829852/
2. Lord SJ, Lei W, Craft P, Cawson JN, Morris I, Walleser S, et al. A systematic review of the effectiveness of magnetic resonance imaging (MRI) as an addition to mammography and ultrasound in screening young women at high risk of breast cancer. Eur J Cancer [Internet]. 2007 Sep [cited 2023 Oct 18];43(13):1905–17. Available from: https://pubmed.ncbi.nlm.nih.gov/17681781/
3. Shahid H, … JWA, 2016 undefined. An overview of breast MRI. pdfs.semanticscholar.orgH Shahid, JF Wiedenhoefer, D Carol Dornbluth MD, MD Pamela Otto, KA KistApplied Radiology, 2016•pdfs.semanticscholar.org [Internet]. 2016 [cited 2023 Oct 18]; Available from: https://pdfs.semanticscholar.org/ed62/4e7681bf54c930c51b16de8344e5368383c0.pdf
4. Henke E, Nandigama R, Ergün S. Extracellular Matrix in the Tumor Microenvironment and Its Impact on Cancer Therapy. Front Mol Biosci [Internet]. 2020 Jan 31 [cited 2023 Nov 6];6. Available from: https://pubmed.ncbi.nlm.nih.gov/32118030/
5. Runge JH, Hoelzl SH, Sudakova J, Dokumaci AS, Nelissen JL, Guenthner C, et al. A novel magnetic resonance elastography transducer concept based on a rotational eccentric mass: preliminary experiences with the gravitational transducer. Phys Med Biol [Internet]. 2019 Feb 7 [cited 2023 Oct 18];64(4):045007. Available from: https://iopscience.iop.org/article/10.1088/1361-6560/aaf9f8
6. Garteiser P, Sahebjavaher RS, Ter Beek LC, Salcudean S, Vilgrain V, Van Beers BE, et al. Rapid acquisition of multifrequency, multislice and multidirectional MR elastography data with a fractionally encoded gradient echo sequence. NMR Biomed [Internet]. 2013 Oct [cited 2023 Nov 6];26(10):1326–35. Available from: https://pubmed.ncbi.nlm.nih.gov/23712852/
7. Balleyguier C, Lakhdar A Ben, Dunant A, Mathieu MC, Delaloge S, Sinkus R. Value of whole breast magnetic resonance elastography added to MRI for lesion characterization. NMR Biomed [Internet]. 2018 Jan 1 [cited 2023 Nov 6];31(1). Available from: https://pubmed.ncbi.nlm.nih.gov/29073719/
Figures