4607
Tissue-Independent SNR Measurement for Supine Breast Coil Assessment1Stanford University, Stanford, CA, United States, 2GE Healthcare, Chicago, IL, United States
Synopsis
Keywords: Breast, Breast
Motivation: Breast MRI typically is performed with a patient in the prone position. Imaging supine would dramatically improve patient comfort and possibly reduce setup and positioning times.
Goal(s): Compare image quality in breast MRI between the supine and prone positions with specialized coils using signal-to-noise ratio.
Approach: To account for tissue deformation between supine and prone positions, we compare “tissue-independent” relative SNR, which uses the body coil SNR as a reference, in the breast tissue between prone and supine.
Results: In multiple patients, the supine position consistently showed an improvement in SNR over the prone position.
Impact: Improvements in motion correction approaches and development of flexible coils may enable supine breast imaging, which is much more comfortable for the patient than prone imaging. Using a careful comparison, we demonstrate substantially higher SNR in supine imaging.
Introduction
Breast MRI is typically performed with the patient in a prone position to mitigate respiration artifacts. However, co-localization of these images with surgery, which is performed in the supine position, is difficult. Additionally, the prone setup tends to be exceedingly uncomfortable for patients, affecting patient movement and positioning during the scan. Recent efforts have focused on developing supine breast imaging methods1-2 and coils to improve signal-to-noise ratio (SNR) and mitigate respiratory motion.Evaluating potential SNR differences between supine and prone setups is exceedingly difficult due to the large deformations, and thus tissue compositions seen by coils, in the breast between the two positions. In this work, we present a novel SNR-based metric that is independent of signal to allow for a tissue-independent SNR comparison between supine and prone breast coils.
Methods
TheoryTo evaluate SNR differences between the two positions, we propose a relative SNR metric: $$$SNR_{rel} = \frac{SNR_{ext}}{SNR_{body}}$$$, where $$$SNR_{ext}$$$ refers to the SNR of the external coil and $$$SNR_{body}$$$ refers to the SNR of the the body coil. Assuming the MR signal in each voxel does not change (gains constant at each position), we get that $$$SNR_{rel} = \frac{\sigma_{body}}{\sigma_{ext}}$$$, where $$$\sigma$$$ represents the standard deviation of the noise normalized by the signal sensitivity at each pixel, implying independence from underlying signal variation.
Methods
Phantom experiments were performed on a breast phantom to validate the signal-independence of the relative SNR metric. Data was acquired using 3D T1-weighted SPGR and 3D T2-weighted CUBE sequences on a 3T Premier (GE Healthcare) using the 60-channel breast coil prototype3 and the body coil.
Three patients and two volunteers were recruited for a research breast MRI exam. Recruitment followed IRB polices and all subjects provided written informed consent. Volunteers and patients were scanned on a 3T Signa Premier System (GE HealthCare) in both the supine (60-channel breast-specific flexible AIR coil3) and prone (16-channel Sentinelle breast coil) positions. In each position, a low-resolution (~3.5mm in-plane, 5mm slice thickness) 3D T1-weighted SPGR sequence was acquired for the breast coil and body coil, with transmit gains and receiver gains kept constant.
Images were reconstructed using a standard SENSE reconstruction, and SNR maps were computed using the pseudo-multiple replica method4 with 500 iterations. Coil sensitivity maps were estimated by lowpass filtering the fully sampled k-space data.
Relative SNR was measured in breast tissue on 20 central slices for each acquisition. Segmentation of breast tissue was performed to measure relative change in the tissue of interest. For each set of in vivo data, a left-tailed Wilcoxon rank sum test was performed to determine whether the median relative SNR for supine was greater than for prone.
Results
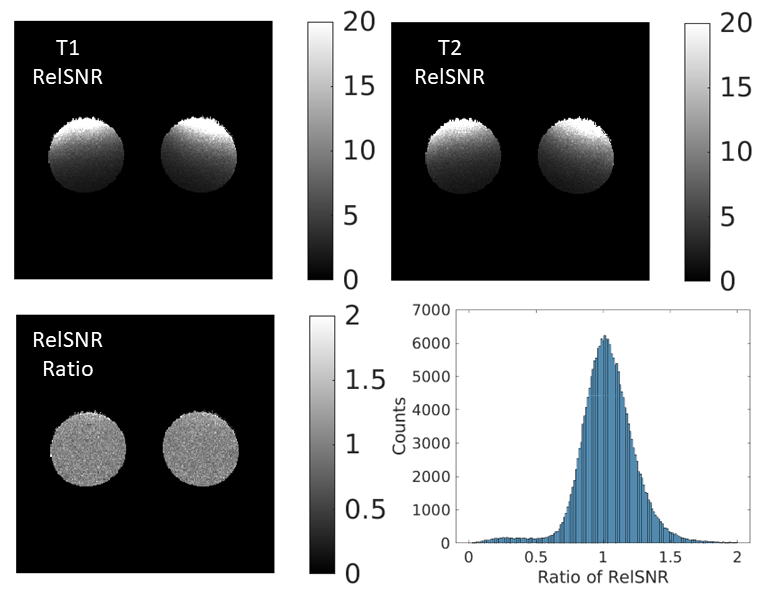
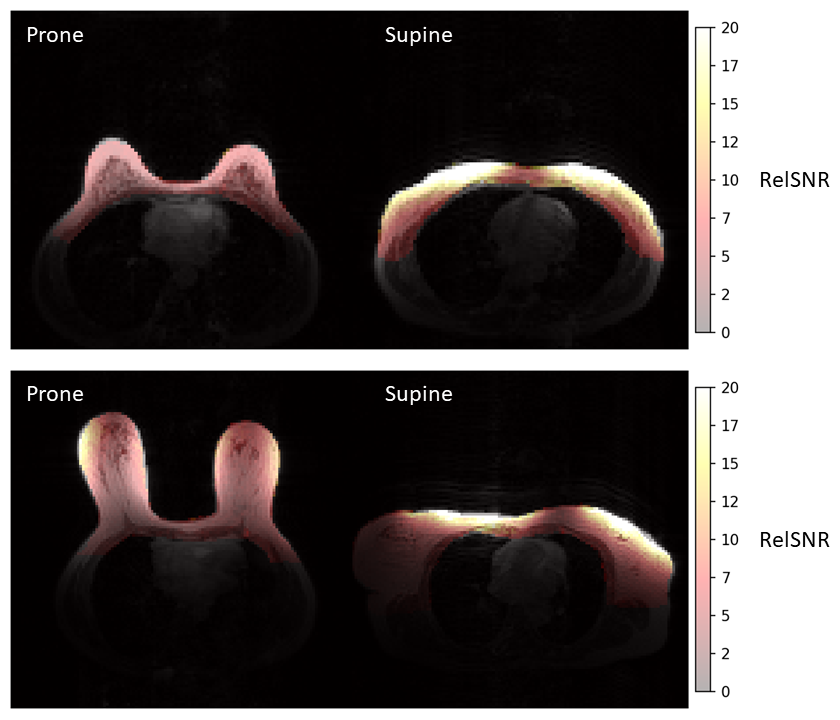
Phantom images demonstrating the metric’s signal independence are shown in Figure 1. The spatial distributions of the relative SNR are similar despite differences in the underlying MR signal, and the ratios of the relative SNR metric is close to 1 across the phantom.Sample images of the relative SNR distributions for two patients overlaid on low-resolution anatomical images are shown in Figure 2. The regional variation in relative SNR can easily be seen between the prone and supine images.
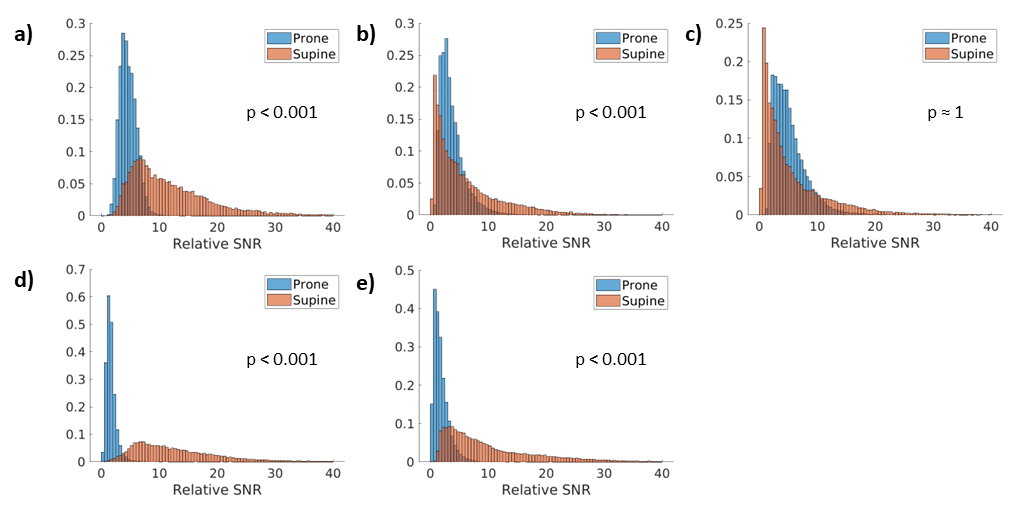
Histograms of the relative SNR distribution for all in vivo cases are shown in Figure 3. The Wilcoxon rank sum test states that for all cases except 3, the median relative SNR of supine is statistically higher than prone.
Discussion
The phantom results indicate that relative SNR is a function of coil performance and overall geometric position and is invariant to the underlying voxel MR signal. The spread of the distribution is most likely due to the Monte Carlo-based method used in calculating the SNR maps. In breast MRI, where tissue composition can vary widely between patients and across the breast, relative SNR can provide a tissue-independent metric for SNR comparison.While 4/5 datasets in this initial method validation demonstrated higher SNR with the supine versus prone coil, further investigation of the SNR performance of the supine coils is necessary. SNR will vary from region to region based on the size and composition of the breast tissue in an individual with both prone and supine coils. Refined tissue segmentation and regional assessment of the SNR will help to inform supine versus prone coil performance.
Conclusion
Relative SNR is a signal-invariant metric for analyzing the image quality between supine and prone breast MRI. In a small number of subjects, these results indicate that supine positioning and flexible coils increase SNR versus prone coils.Acknowledgements
We gratefully acknowledge the research support of GE Healthcare and the following funding sources: NIH R01-EB009055 and NIH R01-CA249893.References
1. Gombos EC, Jayender J, Richman DM, et al. Intraoperative supine breast MR imaging to quantify tumor deformation and detection of residual breast cancer: Preliminary results. Radiology 2016;281:720-729.
2. Mallory MA, Sagara Y, Aydogan F, et al. Feasibility of intraoperative breast MRI and the role of prone versus supine positioning in surgical planning for breast-conserving surgery. Breast J 2017;23:713-717.
3. Vincent J, Follante C, Bayram E, et al. Ultra-flexible, high-resolution, 60-channel RF coil for supine breast imaging. Proceedings of the ISMRM and SMRT annual meeting and exhibition; Concord, CA, 2021 abstract 1591.
4. Robson PM, Grant AK, Madhuranthakam AJ, Lattanzi R, Sodickson DK, McKenzie CA. Comprehensive quantification of signal-to-noise ratio and g-factor for image-based and k-space-based parallel imaging reconstructions. Magn Reson Med. 2008 Oct;60(4):895-907. doi: 10.1002/mrm.21728. PMID: 18816810; PMCID: PMC2838249.
Figures