4604
DCE-MRI Tumor Volumetric Changes Predict Response to Neoadjuvant Immunochemotherapy in Triple Negative Breast Cancer Patients1Abdominal and Breast Imaging, The University of Texas MD Anderson Cancer Center, Houston, TX, United States, 2Breast Imaging, The University of Texas MD Anderson Cancer Center, Houston, TX, United States, 3Biostatistics, The University of Texas MD Anderson Cancer Center, Houston, TX, United States, 4Radiology - Breast Imaging, UT Southwestern Medical Center, Dallas, TX, United States, 5Cancer Systems Imaging, The University of Texas MD Anderson Cancer Center, Houston, TX, United States, 6Imaging Physics - Research, The University of Texas MD Anderson Cancer Center, Houston, TX, United States, 7Breast Imaging - Research, The University of Texas MD Anderson Cancer Center, Houston, TX, United States, 8Imaging Physics, The University of Texas MD Anderson Cancer Center, Houston, TX, United States, 9Breast Medical Oncology, The University of Texas MD Anderson Cancer Center, Houston, TX, United States
Synopsis
Keywords: Breast, Breast, Treatment response prediction, DCE-MRI, biomarkers
Motivation: There is unmet need for noninvasive biomarkers for neoadjuvant immunochemotherapy (NICT) response prediction in triple negative breast cancer (TNBC) to guide least toxic and most effective treatment regimens.
Goal(s): To evaluate if DCE-MRI tumor volume changes measured early during NICT can predict treatment response.
Approach: DCE-MRI tumor volume reduction (TVR) was calculated in 64 TNBC at baseline, after 2 and 4 cycles of NICT and correlated with surgical pathology using ROC analysis.
Results: DCE-MRI TVR after 2 cycles of NICT was able to predict pCR with AUC of 0.71 (95%CI:0.57-0.84) and after 4 cycles with AUC of 0.81 (95%CI:0.69-0.92).
Impact: DCE-MRI tumor volume changes early during neoadjuvant immunochemotherapy can identify triple negative breast cancer patients with high/low likelihood of pathologic complete response, triaging them to appropriate management for de-escalation trials versus targeted therapies, avoiding unnecessary toxicity of ineffective treatment.
Introduction
Triple-negative breast cancer (TNBC) is a highly aggressive subtype of breast cancer usually treated with presurgical neoadjuvant chemotherapy. Approximately 50% of the patients achieve pathologic complete response (pCR) at surgery1, with studies showing that the pCR patients have excellent long-term outcomes2,3. Neoadjuvant immunotherapy in combination with neoadjuvant chemotherapy was recently approved for treatment of TNBC patients with an increased rate of pCR (up to 65%) compared to neoadjuvant chemotherapy alone4. However, neoadjuvant immunotherapy is associated with severe toxicity, including death4. DCE-MRI functional tumor volume has been shown to be a better predictor of the neoadjuvant treatment response than clinical measurements or tumor’s longest diameter, as well as predictive of long-term survival5,6. The aim of this study was to determine if changes in TNBC tumor volume based on DCE-MRI measured early during treatment, after 2 and/or 4 cycles of neoadjuvant immunochemotherapy, can identify patients with a high likelihood of achieving pCR, potentially help to triage them to continuation of neoadjuvant immunochemotherapy or, when appropriate, to de-escalation trials. Conversely, treatment resistant tumors that are identified early may benefit from other treatment strategies, including novel targeted trials, to avoid the unnecessary toxicity of an inefficient neoadjuvant immunochemotherapy.Methods
Datasets: Preliminary analysis from our prospective IRB-approved study (NCT02276443) included 64 patients with stage I-III TNBC who underwent DCE-MRI (temporal resolution: 9-12 sec) at baseline, after 2 cycles, and 4 cycles of neoadjuvant immunotherapy combined with standard of care neoadjuvant chemotherapy (Paclitaxel +/- carboplatin) (Figure 1).DCE-MRI series based on differential subsampling with cartesian ordering (DISCO) sequence were obtained with the following scan parameters: field of view = 34 × 34 cm, slice thickness = 3.0 mm, slice spacing = −1.5 mm, flip angle = 12°, repetition time = 7.6 ms, echo time 1/echo time 2 = 1.1/2.3 ms, total acquisition time = 7 min, matrix = 320 × 320, number of acquired slices = 60−115, in-plane spatial resolution = 0.6−0.8 mm, temporal resolution of DISCO series = 8−15.5 s, receiver bandwidth = ±166.7 kHz, and number of excitations = 0.69.
Tumor volumes were calculated using 3 axis measurements of the index lesion in the early phase of DCE-MRI (1 min) using the ellipse volume equation:
Volume = width x length x height x 0.52.
Percent tumor volume reduction (TVR) between baseline, and after 2 and after 4 cycles of treatment was calculated using the following formula:
% Tumor volume reduction = (Volume baseline – Volume 2 cycles or 4 cycles)/ Volume baseline
Pathologic complete response was assessed at surgery after completion of neoadjuvant treatment and was defined as absence of residual invasive cancer in the breast and axillary lymph nodes.
Statistics: Receiver operating characteristic (ROC) analyses and assessment of area under the curve (AUC) were used to evaluate the performance of pCR prediction based on the percentage reduction in tumor volume between baseline and after 2 cycles, as well as between baseline and after 4 cycles of neoadjuvant immunochemotherapy. Positive predictive value (PPV) and negative predictive value (NPV) curve analyses were conducted, along with 95% confidence intervals, to identify the specific tumor volume reduction thresholds that could predict the occurrence of pCR or the presence of residual disease following 2 and 4 cycles of neoadjuvant immunochemotherapy.
Results and Discussion
59% (38/64) of the patients achieved pCR after neoadjuvant immunochemotherapy. Following 4 cycles of treatment DCE-MRI TVR was able to predict pCR with an AUC of 0.81 (95% CI: 0.69-0.92). TVR ≥95% after 4 cycles was predictive of chemosensitivity with PPV 82%, while TVR ≤75% was predictive of chemoresistance with NPV 100% (Figures 2, 3). DCE-MRI TVR after 2 cycles of neoadjuvant immunochemotherapy was able to predict pCR with an AUC of 0.71 (95% CI: 0.57-0.84). TVR≥90% after 2 cycles predicted pCR with PPV 86%, and TVR≤35% predicted chemoresistance with NPV 100% (Figure 4).Conclusion
TVR by DCE-MRI measured early during neoadjuvant immunochemotherapy was able to predict pCR status of TNBC patients, as either excellent responders or nonresponders. Higher accuracy of prediction was seen after 4 cycles of treatment (AUC 0.81) than after 2 cycles (AUC 0.71) of neoadjuvant immunochemotherapy. These preliminary results will be validated in a larger cohort after completion of the ongoing prospective clinical trial.Acknowledgements
This work was supported by the University of Texas MD Anderson Moon Shots Program and Robert D. Moreton Distinguished Chair Funds in Diagnostic Radiology. This study was supported by the NIH/NCI under award number P30CA016672.
References
1. Symmans WF, Yau C, Chen YY, et al. Assessment of residual cancer burden and event-free survival in neoadjuvant treatment for high-risk breast cancer: an analysis of data from the I-SPY 2 randomized clinical trial. JAMA Oncol 2021;7:1654-1663.
2. von Minckwitz G, Untch M, Blohmer JU, et al: Definition and impact of pathologic complete response on prognosis after neoadjuvant chemotherapy in various intrinsic breast cancer subtypes. J Clin Oncol 2012;30:1796-1804.
3. Cortazar P, Zhang L, Untch M, et al: Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet 2014;384:164-172.
4. P. Schmid, J. Cortes, L. Pusztai, H. et al Pembrolizumab for Early Triple-Negative Breast Cancer. N Engl J Med 2020;382:810-21.
5. Hylton NM, Blume JD, Bernreuter WK, et al: Locally advanced breast cancer: MR imaging for prediction of response to neoadjuvant chemotherapy--results from ACRIN 6657/I-SPY TRIAL. Radiology 2012;263:663-672.
6. Hylton NM, Gatsonis CA, Rosen MA, et al: Neoadjuvant Chemotherapy for Breast Cancer: Functional Tumor Volume by MR Imaging Predicts Recurrence-free Survival-Results from the ACRIN 6657/CALGB 150007 I-SPY 1 TRIAL. Radiology 2016;279:44-55.
Figures
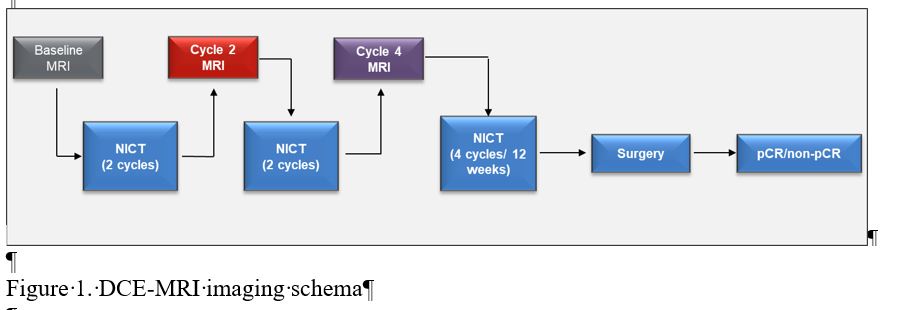
Figure 1. DCE-MRI imaging schema
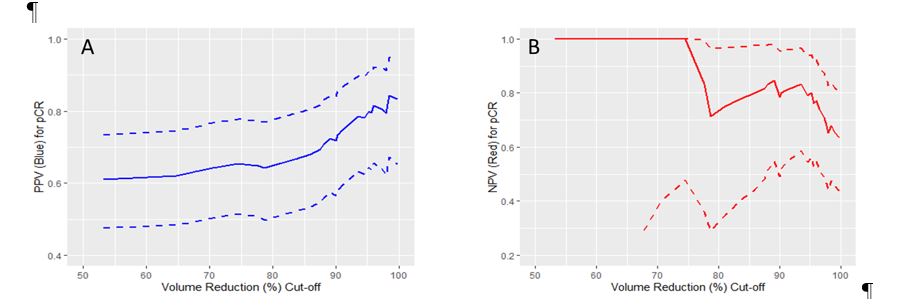
Figure 2. PPV (A) and NPV (B) of DCE-MRI TVR for the prediction of pCR after 4 cycles of neoadjuvant immunochemotherapy, AUC 0.81 (95% CI: 0.69-0.92)
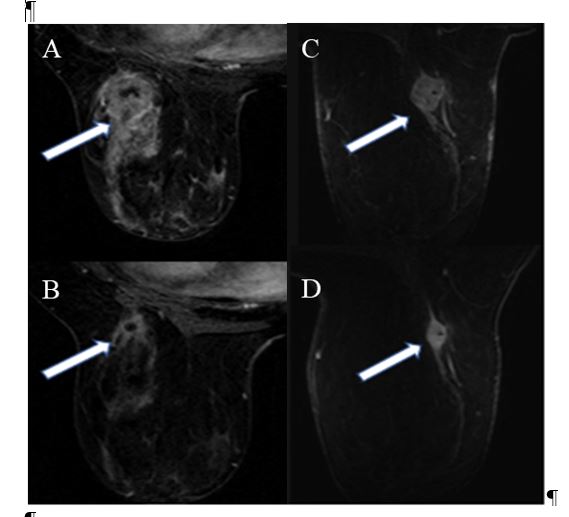
Figure 3. (A) Baseline and (B) after 4 cycles DCE-MRI of a patient with 96% TVR after 4 cycles of neoadjuvant immunochemotherapy; TVR >95% was predictive of pCR. No residual disease was seen at surgical pathology. (C) Baseline and (D) after 4 cycles DCE-MRI of another patient with 49% TVR after 4 cycles of neoadjuvant immunochemotherapy, TVR≤75% was predictive of non pCR. Residual invasive disease was seen at surgical pathology.
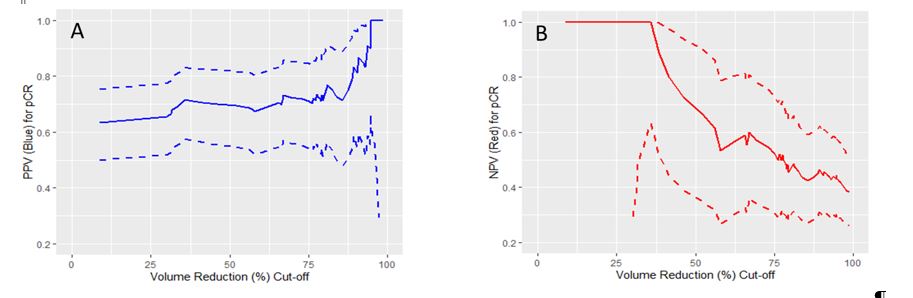
Figure 4. PPV (A) and NPV (B) of DCE-MRI TVR for the prediction of pCR after 2 cycles of neoadjuvant immunochemotherapy, AUC 0.71 (95% CI: 0.57-0.84)