4602
Prediction of axillary lymph nodes metastases in patients with breast cancer : Can synthetic MRI provide additional value to DWI?1Affiliated hospital of Jiangnan university, wu xi, China, 2GE Healthcare, Beijing, China
Synopsis
Keywords: Breast, Breast, Axillary lymph node; metastasis
Motivation: The aim of this study was to investigate whether synthetic MRI-derived quantitative maps can predict metastasis of axillary lymph nodes (ALNs) in breast cancer.
Goal(s): Searching for a noninvasive method to predict lymph node metastasis in breast cancer.
Approach: 61 breast cancer patients were recruited for the study and the status of ALNs was confirmed by pathology. T1, T2, and PD maps were obtained for each patient.
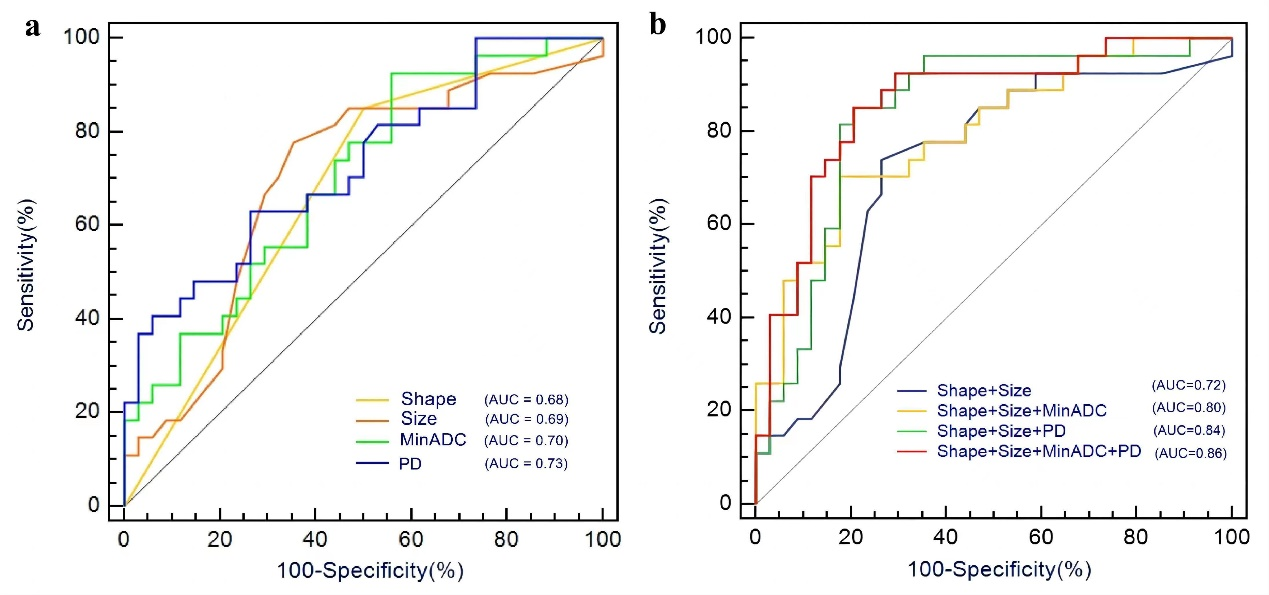
Results: Statistically significant differences in PD, minimal ADC , anatomic features of tumor shape and size were observed between patients with and without metastatic ALNs metastasis. It was shown that PD+Min ADC+shape+size with highest AUC of 0.86.
Impact: it can be concluded that syMRI derived relaxation maps may be useful for predicting ALNs status in breast cancer.
Introduction
Axillary lymph nodes (ALNs) metastases occur in approximately 40% of patients with early-stage breast cancer (BC), significantly affecting the health and prognosis of BC patients and reducing their overall survival rate[1,2]. Moreover, blindly extensive ALNs dissection can lead to complications, such as long thoracic nerve damage, upper arm paresthesia, and lymphedema. Hence, determination of preoperative ALNs status is crucial for accurate clinical staging and individualized treatment in BC patients[3]. Magnetic resonance image compilation (MAGiC), as a vendor-provided synthetic MRI (SyMRI), is a relatively new quantitative imaging technique. MAGiC employs a multi-echo multi-delay acquisition technique, allowing for the simultaneous quantification of T1 and T2 relaxation times, as well as proton density (PD) images, in a matter of minutes.[4-6] Recent studies have utilized SyMRI for the identification of lymph node status in rectal cancer[7] and nasopharyngeal cancer[8].The purpose of this study was to investigate whether synthetic MRI (SyMRI) provides additional value to conventional MRI and diffusion-weighted imaging (DWI) in predicting ALNs metastases through breast lesions.Methods
SubjectsA total of 61 patients were recruited for the study, including patients with metastatic ALNs(n=37) and patients without metastatic ALNs(n=24). All patients underwent postoperative pathologic analysis. MRI acquisitionAll MRI examinations were performed on a 3.0T scanner (Signa Architect; GE Healthcare) equipped with an 8-channel phased-array breast coil. Conventional T1WI, T2WI , DWI, and MAGiC imaging were performed for each participant. The scanning parameters for SyMRI were as follows: field of view (FOV), 36 × 36 cm2; repetition time (TR), 4032 ms; echo time (TE), 24.5/97.9 ms; matrix, 320 × 256; echo train length, 12; number of excitation (NEX), 1; and slice thickness/gap, 4/1 mm.Image analysisThe MAGiC data were processed using SyMRI 8.0 software to generate quantitative T1, T2, and PD maps. To obtain quantitative parameters of breast tumors from SyMRI, the regions of interest (ROIs) were manually delineated along the tumor’s edge, avoiding artifacts, large vessels, necrotic areas, and cystic regions on the largest axial cross-section of breast tumor from synthetic T2WI. Automated localization could be performed directly on the T1, T2, and PD maps simultaneously.Statistical analysis
All statistical analyses were performed by utilizing SPSS (version 25.0) and MedCalc software (version 19.2.6). Intraclass correlation coefficients and weighted kappa values assessed interobserver agreement between two radiologists for each parameter measured. All quantitative parameters were tested for normality. Comparisons of each parameter between groups with and without metastatic ALNs were performed using Student's t-test for normal distribution and Mann-Whitney U-test for non-normal distribution. The chi-square test or Fisher exact probability method was used for categorical variables. For statistically significant parameters, the receiver operating characteristic (ROC) curve with the area under the ROC curve (AUC) was used to separately assess their diagnostic efficacies in differentiating metastatic ALNs from non-metastatic ALNs. P<0.05 was considered the difference with statistical significance.Results
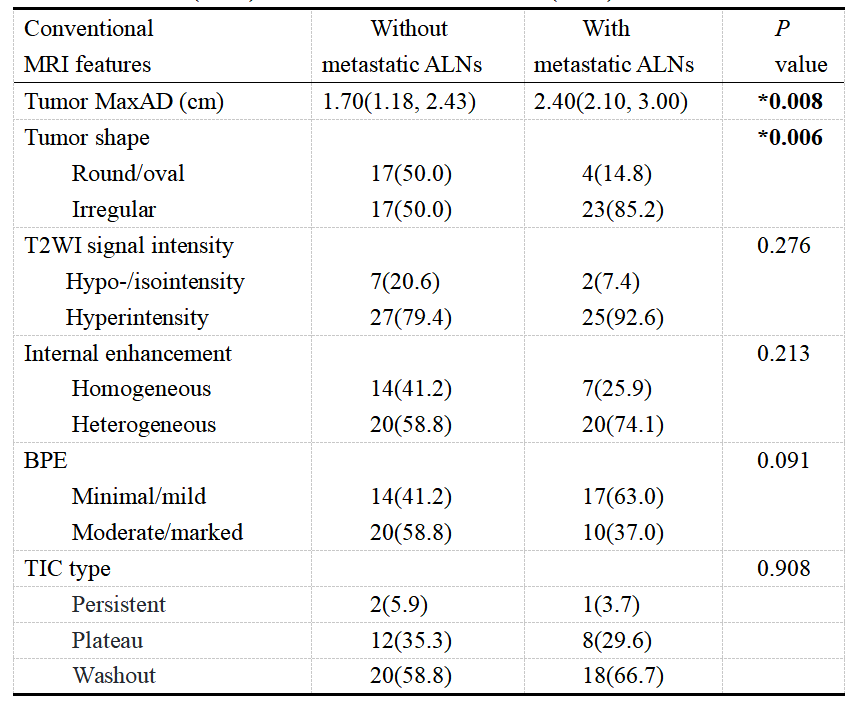
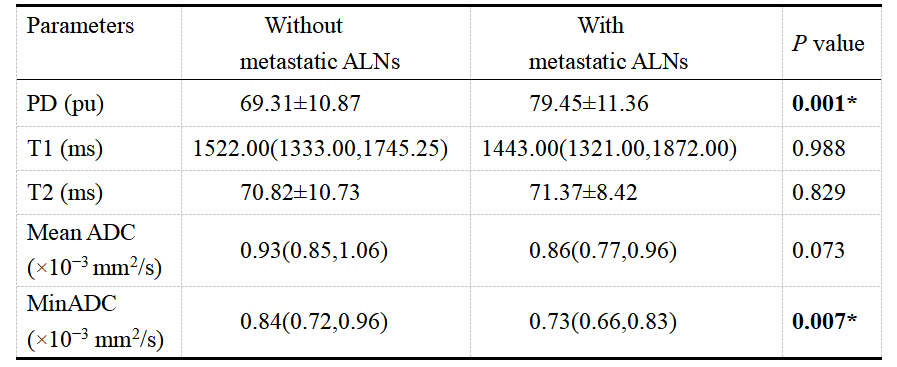
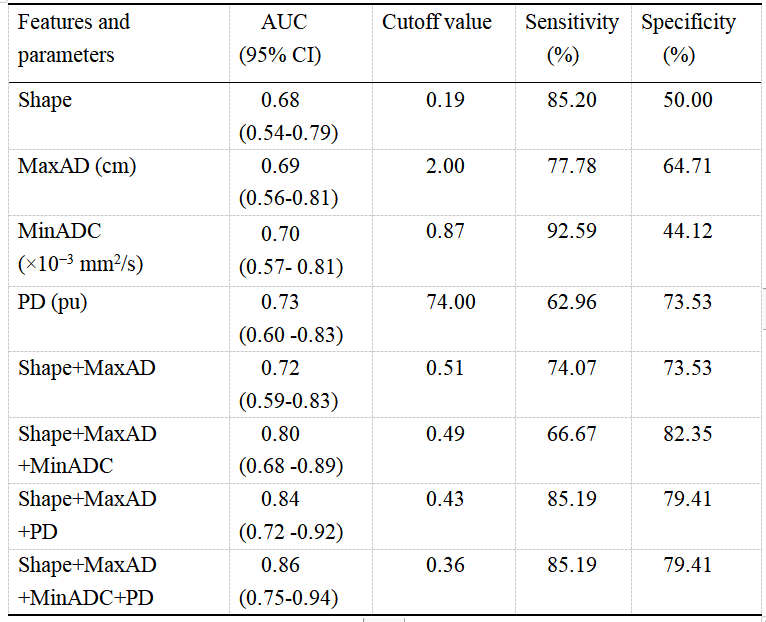
Compared to 34 breast cancer patients without metastatic ALNs, 27 patients with metastatic ALNs had significantly higher proportions of irregular-shaped tumors, larger maximum axis diameter (MaxAD), higher proton density (PD) values, and lower minimum apparent diffusion coefficient (MinADC) values (all P < 0.05). Moreover, the prediction model with conventional and DWI parameters (tumor shape+MaxAD+MinADC) yielded an AUC of 0.80 (95% CI: 0.68-0.89), with a sensitivity of 66.67% and specificity of 82.35%; After adding SyMRI-derived PD to the model (tumor shape+MaxAD+MinADC+PD), the AUC increased to 0.86 (95% CI: 0.75-0.94), with a sensitivity of 85.19% and specificity of 79.41%.Discussion
In this study, we investigated the role of quantitative profiles generated by MAGiC in predicting the status of ALNs in breast cancer. Our study found differences in PD values between patients with and without metastatic ALNs. The possible explanation is that PD is typical property that provide water content information of tissue and thus is sensitive to edema and structural damage[9]. It has been studied that the more malignant the surface tumor is, the higher the PD value is[10]. We hypothesized that breast cancers with metastatic lymph nodes have higher PD values and are more susceptible to necrosis and structural damage.Conclusions
Together with conventional MRI and DWI, SynMRI with quantitative metrics can offer additional value to enhance the predictive performance in determining ALNs status for breast cancer patients before surgery.Acknowledgements
No acknowledgement found.References
[1] Thompson AM. New standards of care in the management of the axilla. Current Opinion in Oncology. 2012 Nov;24(6):605-611.
[2] Zarebczan DB, Neuman HB. Management of the Axilla. Surgical Clinics of North America. 2013 Apr;93(2):429-444.
[3] Langer I, Guller U, Berclaz G et al. Morbidity of sentinel lymph node biopsy (SLN) alone versus SLN and completion axillary lymph node dissection after breast cancer surgery: a prospective Swiss multicenter study on 659 patients. Ann Surg. 2007 Mar;245(3):452-461.
[4] Warntjes JBM, Leinhard OD, West J, Lundberg P. Rapid magnetic resonance quantification on the brain: Optimization for clinical usage. Magn Reson Med. 2008 August;60(2):320-329.
[5] Warntjes JBM, Dahlqvist O, Lundberg P. Novel method for rapid, simultaneous T1, T2*, and proton density quantification. Magn Reson Med. 2007 March;57(3):528-537.
[6] Jung Y, Gho SM, Back SN, Ha T, Kang DK, Kim TH. The feasibility of synthetic MRI in breast cancer patients: comparison of T2 relaxation time with multiecho spin echo T2 mapping method. Br J Radiol. 2018 September;92(1093):20180479.
[7] Ge YX, Hu SD, Wang Z, et al. Feasibility and reproducibility of T2 mapping and DWI for identifying malignant lymph nodes in rectal cancer. Eur Radiol. 2021 May;31(5):3347-3354.
[8] Wang P, Hu S, Wang X, et al. Synthetic MRI in differentiating benign from metastatic retropharyngeal lymph node: combination with diffusion-weighted imaging. Eur Radiol. 2022 Aug;33(1):152-161.
[9] Gracien RM, Reitz SC, Hof SM, et al. Changes and variability of proton density and T1 relaxation times in early multiple sclerosis: MRI markers of neuronal damage in the cerebral cortex. Eur Radiol. 2016 Aug;26(8):2578-2586.
[10] Li Q, Xiao Q, Yang M, et al. Histogram analysis of quantitative parameters from synthetic MRI: Correlations with prognostic factors and molecular subtypes in invasive ductal breast cancer. European Journal of Radiology. 2021 Jun;139:109697.
Figures