4600
Machine Learning with Multiparametric MRI for preoperative prediction of intraductal component in invasive breast cancer1The Third Affiliated Hospital of Zhengzhou University, Zhengzhou, China, 2GE Healthcare MR Research, Beijing, China, Beijing, China
Synopsis
Keywords: Breast, Breast, Machine Learning
Motivation: To predict the presence of an intraductal component (ductal carcinoma in situ, DCIS) in invasive breast cancer (IBC-IC).
Goal(s): To improve the preoperative prediction of IBC-IC.
Approach: This study was to develop and validate a machine-learning algorithm to preoperatively predict IBC-IC using the multiparametric MRI features.
Results: The machine learning model with multiparametric MRI features could provide the individualized probability of IBC-IC and might help to optimize surgical planning for patients with breast cancer before BCS.
Impact: This study developed a prediction model combining a machine-learning algorithm with multiparametric MRI features to preoperatively predict intraductal component in invasive breast cancer, which may be beneficial to the preoperative planning of breast-conserving surgery for early-stage invasive breast cancer.
Introduction and Purpose
Breast-conserving surgery (BCS) is regarded as the most preferred treatment for early-stage invasive breast cancer (IBC). It is reported that positive surgical margins are correlated with increased locoregional recurrence after BCS [1]. The presence of an intraductal component (ductal carcinoma in situ, DCIS) in invasive breast cancer (IBC-IC) increases the risk of positive resection margins [2], re-operation rate [3], and local-regional recurrence [4]. Compared with the other imaging modalities, Magnetic Resonance Imaging (MRI) can improve the detection and depiction of the IBC-IC before surgery [5]. However, few studies of the incorporation of machine learning and image characteristics to improve the preoperative prediction of IBC-IC are reported. The purpose of this study was to develop and validate a machine-learning algorithm to preoperatively predict IBC-IC using the multiparametric MRI features.Materials and Methods
The prediction model was trained with 320 consecutive patients from January 2017 to March 2022, including 109 IBC-IC and 211 IBC identified by histopathological results. The validation cohort of 140 patients (55 IBC-IC and 85 IBC) from March 2022 to March 2023 was included to test the prediction model. Conventional sequence scans were performed, including T1WI, T2WI, and DWI before dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) scan using two 3.0 T MR scanners (Pioneer, SIGNA, GE Healthcare, Skyra, MAGNETOM, Siemens Healthcare) with the 8-channel phased-array coil. The image characters, including background parenchymal enhancement (BPE), root sign, time-intensity curve (TIC), margins, internal enhancement patterns, and peritumoral edema, were determined based on the MRI BI-RADS lexicon [6]. The lesion size was measured on the first phase of the transaxial image after injection of contrast agent, including long and short diameters. For apparent diffusion coefficient (ADC) measurement, the ROI (6-10mm2) was manually drawn on the darkest part of the lesion avoiding cystic or non-enhancing areas and hemorrhage [7]. The machine learning algorithm, extreme gradient boosting (XGBoost) tree [8], was trained and tuned on the training set using tenfold cross-validation. The hypergrid search was used for hyperparameter tuning. The area under the receiver operating characteristic (ROC) curve (AUC), sensitivity, and specificity were used to evaluate the performance of the models. We used the Shapley additive explanation (SHAP) technique to interpret the optimal model output. All data were analyzed with the SPSS (version 26.0, IBM) and R statistical software (version 4.1.2).Results
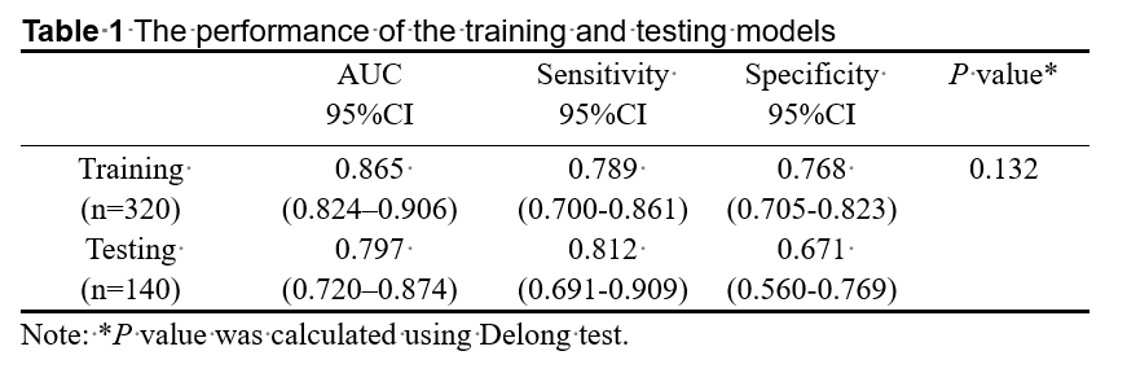
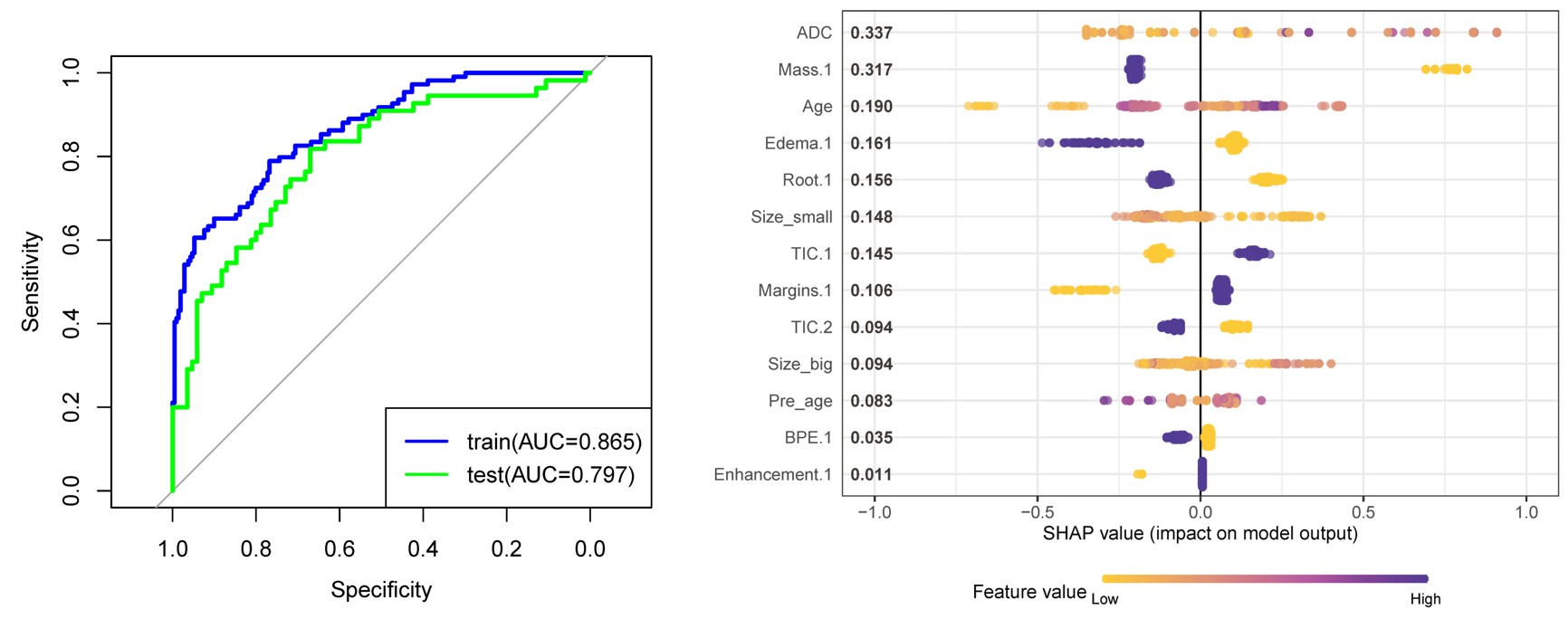
The AUC, sensitivity, and specificity are respectively 0.865 (0.824–0.906), 0.789 (0.700-0.861), and 0.768 (0.705-0.823) in the training cohort and 0.797 (0.720–0.874), 0.812 (0.691-0.909), and 0.671 (0.560-0.769) in the validation cohort. There was no significant difference in AUC between the training and validation models (P = 0.132) (Table 1, Figure 1A). Figure 1B shows the importance of features for the predictions made by the XGBoost tree via the SHAP method. The top three important indices of the model were ADC, the type of enhancement, and patient age. The high ADC value, non-mass enhancement, and higher patient age contribute more to predicting IBC-IC than the other features.Discussion and conclusions
It is crucial to preoperatively predict the presence of an intraductal component in a given tumor for surgical planning and outcome in breast cancer [9]. Recently, Xu et al [10] reported that machine-learning model based on radiomics from DCE-MRI had the potential to predict IBC-IC. However, radiomics approaches are not widely available in current clinical practice because of several issues, including limited availability of efficient and standardized or reproducible systems of feature extraction, and limited data sharing for external validation [11]. Our machine learning model combined with image characteristics showed a similar diagnostic efficiency. Most of them were described in the BI-RADS lexicon, which was based on multi-center large data evaluations, and thus was the most widely guide for describing and categorizing breast lesions. In addition, we used the SHAP technique to evaluate the contribution of each variable to the optimal model. According to our results, the high ADC value was associated with the IBC-IC. The ADC of the intraductal component was higher than that of invasive breast cancer [12]. The feature of non-mass enhancement was also an important variable for the prediction of IBC-IC. Previous studies demonstrated that the extensive IBC-IC often presented as ductal or linear enhancement, long spicules, and a regional enhancing area on MRI [13]. Age is a well-known risk factor for breast cancer [14], which is also shown in our results that patients with IBC-IC were older than those with invasive breast cancers [9]. In conclusion, the machine learning model with multiparametric MRI features could provide the individualized probability of IBC-IC and might help to optimize surgical planning for patients with breast cancer before BCS.Acknowledgements
Funding: This project was supported by the Tianjian Advanced Biomedical Laboratory.References
1 Houssami N, Macaskill P, Luke Marinovich M, Morrow M (2014) The Association of Surgical Margins and Local Recurrence in Women with Early-Stage Invasive Breast Cancer Treated with Breast-Conserving Therapy: A Meta-Analysis. Annals of Surgical Oncology 21:717-730
2 Bae MS, Bernard-Davila B, Sung JS, Morris EA (2019) Preoperative breast MRI features associated with positive or close margins in breast-conserving surgery. European Journal of Radiology 117:171-177
3 Houvenaeghel G, Lambaudie E, Bannier M et al (2019) Positive or close margins: reoperation rate and second conservative resection or total mastectomy. Cancer Management and Research Volume 11:2507-2516
4 Schnitt SJ, Harris JR (2008) Evolution of Breast-Conserving Therapy for Localized Breast Cancer. Journal of Clinical Oncology 26:1395-1396
5 Kuhl CK, Strobel K, Bieling H, et al. Impact of Preoperative Breast MR Imaging and MR-guided Surgery on Diagnosis and Surgical Outcome of Women with Invasive Breast Cancer with and without DCIS Component. Radiology. 2017;284(3):645-655
6 D'Orsi C, Morris E, Mendelson E (2013) ACR BI-RADS® Atlas, Breast Imaging Reporting and Data System
7 Baltzer P, Mann RM, Iima M et al (2020) Diffusion-weighted imaging of the breast-a consensus and mission statement from the EUSOBI International Breast Diffusion-Weighted Imaging working group. Eur Radiol 30:1436-1450
8 Pfob A, Mehrara BJ, Nelson JA, Wilkins EG, Pusic AL, Sidey-Gibbons C (2021) Machine learning to predict individual patient-reported outcomes at 2-year follow-up for women undergoing cancer-related mastectomy and breast reconstruction (INSPiRED-001). Breast 60:111-122
9 Knuttel FM, van der Velden BH, Loo CE et al (2016) Prediction Model For Extensive Ductal Carcinoma In Situ Around Early-Stage Invasive Breast Cancer. Invest Radiol 51:462-468
10 Xu H, Liu J, Chen Z et al (2022) Intratumoral and peritumoral radiomics based on dynamic contrast-enhanced MRI for preoperative prediction of intraductal component in invasive breast cancer. Eur Radiol 32:4845-4856
11 Tagliafico AS, Piana M, Schenone D, Lai R, Massone AM, Houssami N (2020) Overview of radiomics in breast cancer diagnosis and prognostication. The Breast 49:74-80
12 Bickel H, Pinker-Domenig K, Bogner W, et al. Quantitative apparent diffusion coefficient as a noninvasive imaging biomarker for the differentiation of invasive breast cancer and ductal carcinoma in situ. Invest Radiol. 2015;50(2):95-100
13 Van Goethem M, Schelfout K, Kersschot E et al (2007) MR mammography is useful in the preoperative locoregional staging of breast carcinomas with extensive intraductal component. European Journal of Radiology 62:273-282
14 Pfob A, Sidey-Gibbons C, Barr RG et al (2022) Intelligent multi-modal shear wave elastography to reduce unnecessary biopsies in breast cancer diagnosis (INSPiRED 002): a retrospective, international, multicentre analysis. Eur J Cancer 177:1-14
Figures