4599
Evaluation Molecular Receptors Status in Breast Cancer Using an mpMRI-based Feature Fusion Radiomics Model: Mimicking Radiologists’ Diagnosis1Department of Radiology, The Second Affiliated Hospital, School of Medicine, South China University of Technology, Guangzhou, China, 2School of Biomedical Engineering, Southern Medical University, Guangzhou, China, 3Philips Healthcare, Guangzhou, China
Synopsis
Keywords: Breast, Radiomics, Breast Cancer, Molecular Receptors Status, Feature Fusion Radiomics Model
Motivation: Investigating the performance of a feature fusion radiomics (RFF) strategy that mimicked the routine diagnostic practices of radiologists in distinguishing different statuses of molecular receptors in breast cancer (BC) preoperatively.
Goal(s): Develop an RFF model that incorporates optimal mpMRIs for BC’s molecular receptor status identification.
Approach: Constructed and analyzed 150 models to determine the top four optimum sequences for identifying distinct BC’s molecular receptor statuses. Then the optimal single sequence models (Rss) and combined sequences models (RFF) were developed and compared.
Results: The RFF model integrating mpMRI radiomics features exhibited promising ability to imitate radiologists’ diagnosis for preoperative identification of BC’s molecular receptors.
Impact: A multiparametric MR-based RFF model, mimicking the radiologists’ daily diagnostic approach, which fused radiomics features with dominant MR sequences, was able to distinguish different molecular receptor statuses of breast cancer.
Introduction
The radiomics approach has been utilized to preoperatively discern various molecular receptor statuses of BC through one or two specific MRI sequence-derived images, such as T2WI, DWI-derived ADC maps, and early-phase dynamic contrast-enhanced (DCE) MRI[1-3]. However, in routine practice, radiologists are required to review all obtained MRI sequences, including T1WIs, T2WIs, DWIs with diverse b values, DWI-derived ADC maps, and all phases of DCE MRIs for a conclusive diagnosis. To imitate radiologists’ workflow, we constructed an RFF model capable of fusing radiomics features from multiparametric MRIs to investigate its value in distinguishing distinct BC molecular receptor statuses preoperatively.Methods
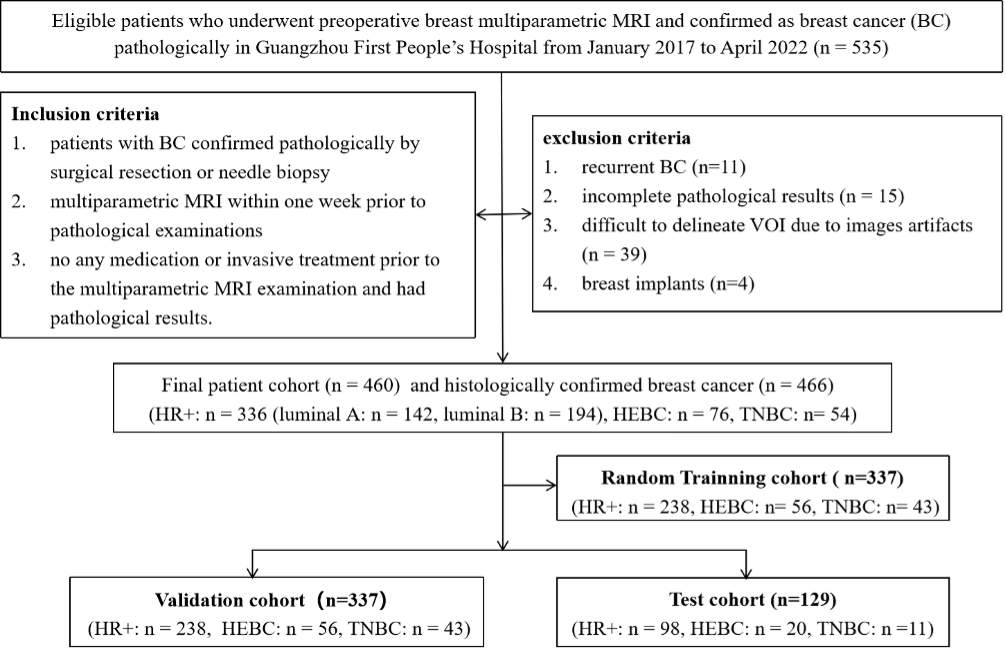
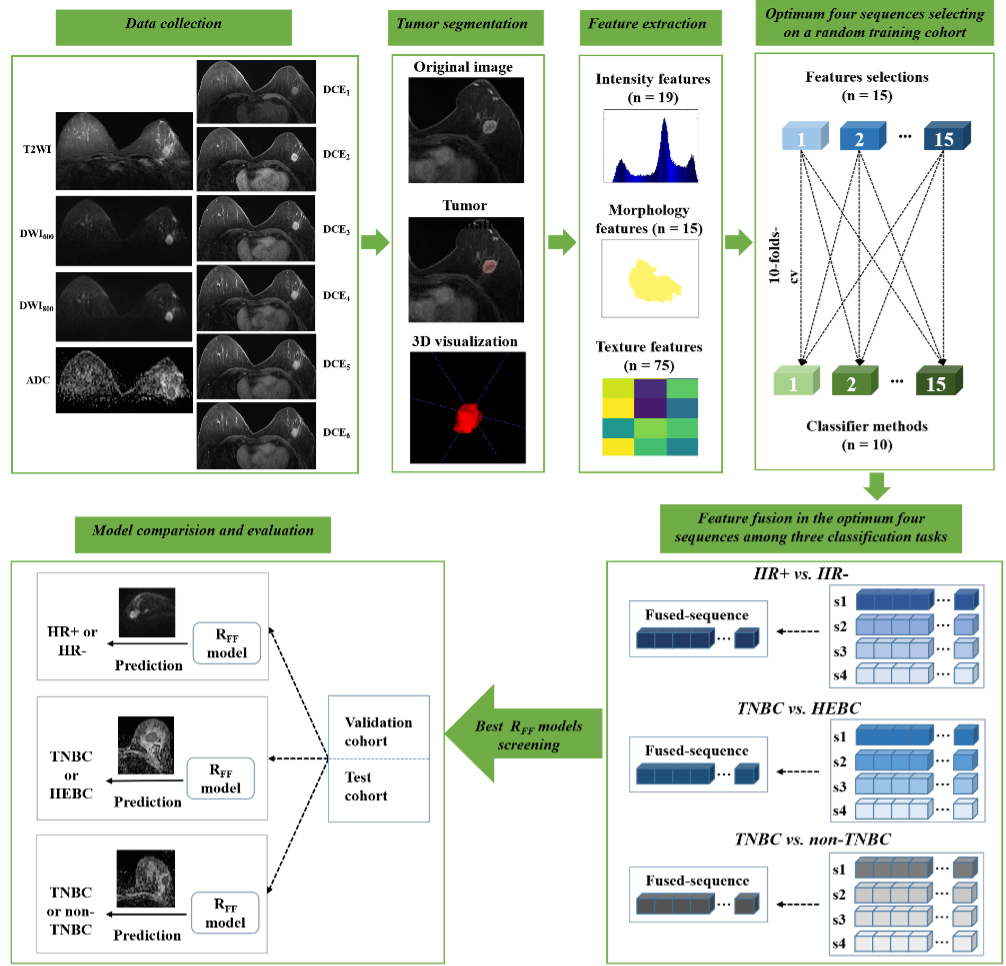
We retrospectively collected data from 460 patients with a total of 466 pathology-confirmed BCs who underwent breast mpMRI on a 1.5T MR scanner (uMR 560, United Imaging) at our center, including hormone receptor (HR) positive (HR+) (n=336) and HR negative (HR-) (n=130). The HR- patients were further categorized into human epidermal growth factor receptor 2 (HER-2) enriched BC (HEBC) (n=76) and triple-negative BC (TNBC) (n=54). All lesions were divided into a training/validation cohort (n=337) and a test cohort (n=129, Figure 1).Ten volumes of interest (VOIs) for each lesion were delineated slice-by-slice on T2WI, DWI600 (b=600 s/mm2), DWI800 (b=800 s/mm2), ADC map, and DCE1-6 (six continuous DCE-MRI) images. A total of 109 radiomics features were extracted from each VOI using Pyradiomics[4] and then fed into 150 classification models that were constructed based on 10 classifiers and 15 feature selection methods.
Approximately 72% of cases (n=337) were selected randomly as the training cohort to analyze all radiomics features from each sequence to identify the optimum sequence capable of distinguishing HR+ vs. HR- BC, TNBC vs. HEBC, and TNBC vs. non-TNBC. The top four high-performance sequences were then chosen for a feature fusion process, to determine the best sequences-combination for developing the RFF models. This process emulated the final assessment by a radiologist, who focuses on sequences with specific features after an initial review. The AUC, sensitivity, accuracy, and specificity of each model were evaluated. The paired samples Wilcoxon signed rank test was used for performance comparison.
Results
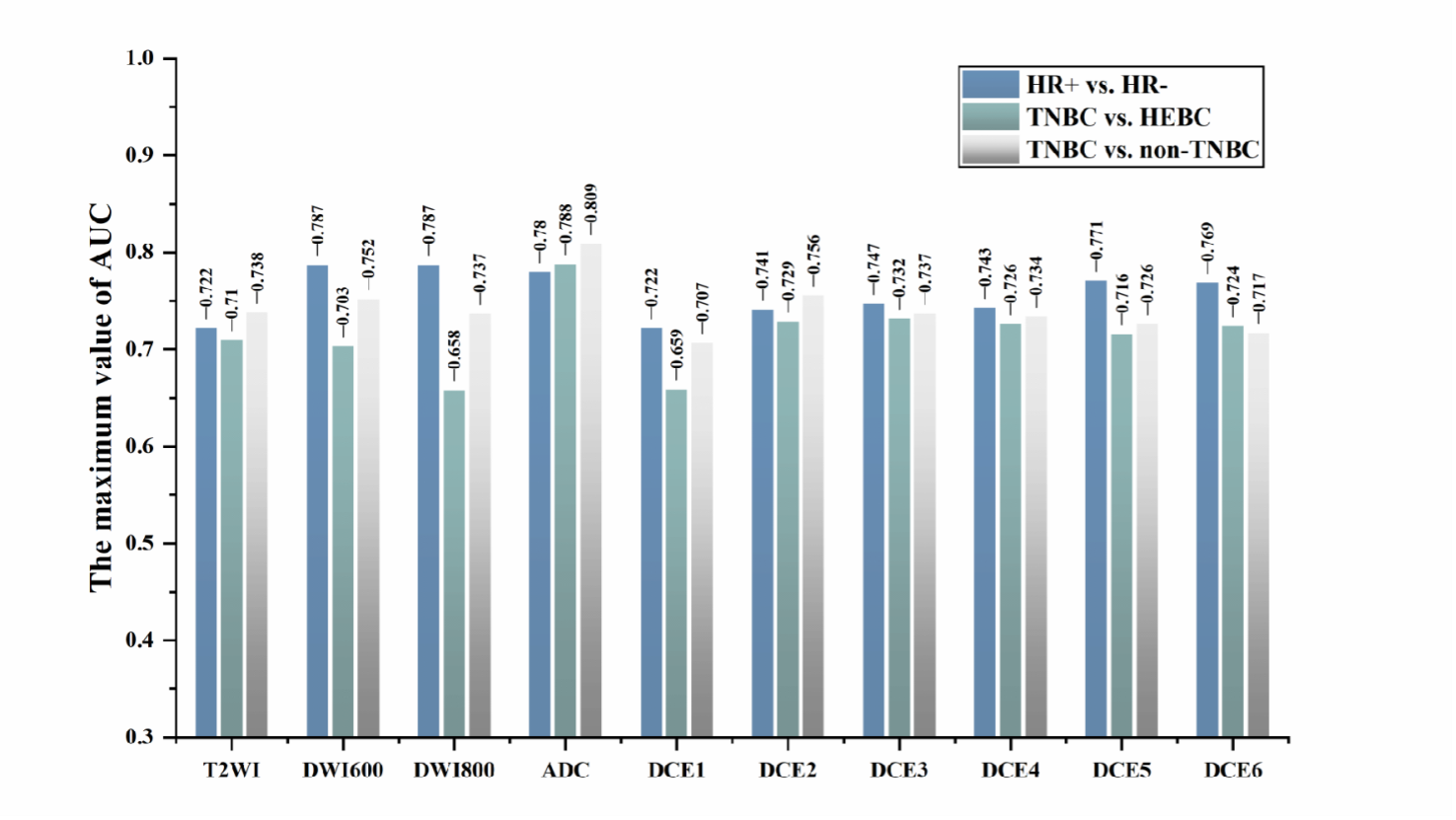
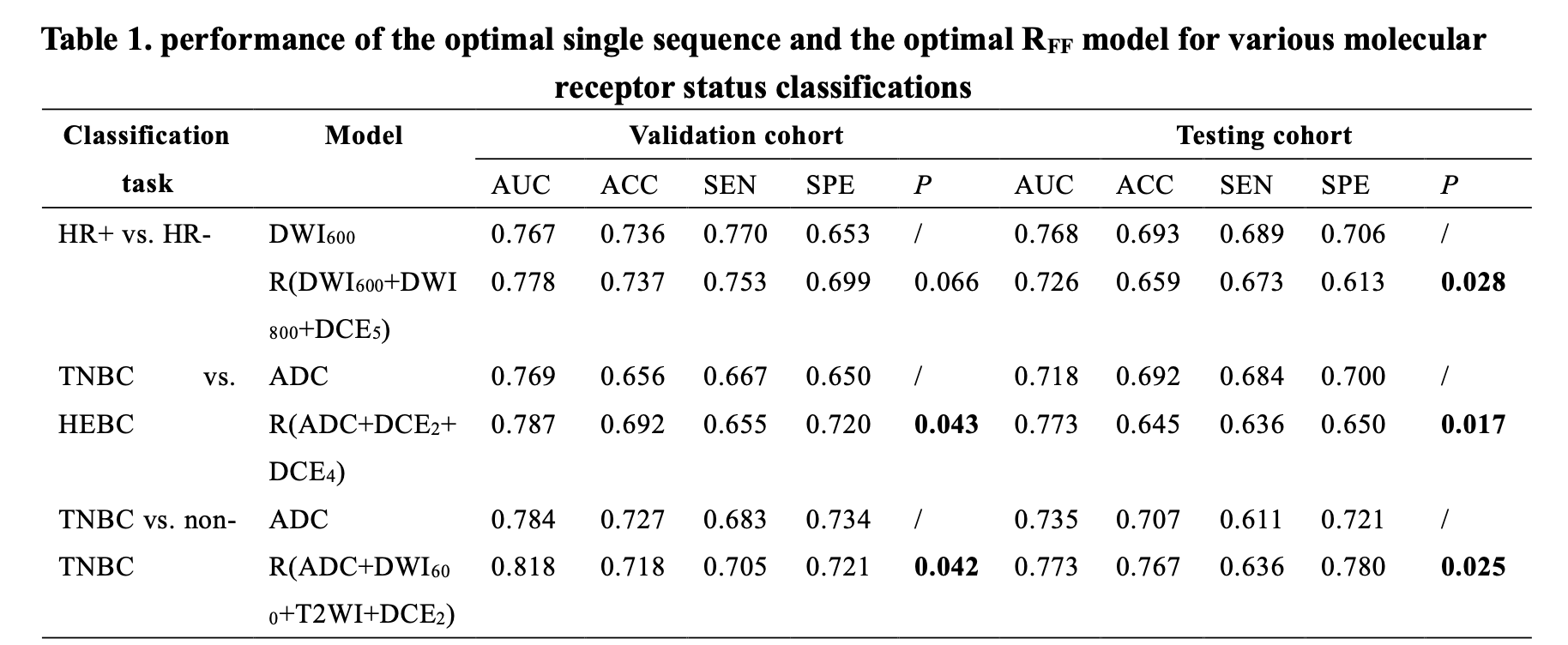
During the three classification tasks, the optimal single sequence for classifying HR+ vs. HR- was DWI600, while the ADC map, derived from DWI800 performed the best in distinguishing TNBC vs. HEBC, as well as identifying TNBC vs. non-TNBC, with corresponding training AUC values of 0.787, 0.788, and 0.809, respectively (Figure 3). Furthermore, the integration of the top four sequences in RFF models yielded improved performance, achieving AUC values of 0.809, 0.805, and 0.847, respectively. Consistent results were observed in both the training/validation and testing cohorts, with AUC values of 0.778,0.787, 0.818, and 0.726, 0.773, 0.773, respectively (all p < 0.05 except HR+ vs. HR-, Table 2).Discussion
Simulating the diagnostic process of radiologists, we comprehensively analyzed radiomics features from mpMRI, screening the optimum MRI sequences for distinguishing HR+ vs. HR -, TNBC vs. HEBC, and TNBC vs. non-TNBC, achieving a good performance with all AUC>0.7. Our strategy compensated for the shortage of previous investigations, where employed only one or two MRI sequence(s) such as T2WI or ADC without exploring all routine multiparameter MRI sequences[1, 5, 6]. In addition, we hypothesized that multi-dimensional image information from multiple MRI sequences could be captured and integrated to provide a more comprehensive representation of the breast lesion, similar to how radiologists concentrate on significant sequences after preliminary review[7]. Thus, we investigated all sequences of a routine breast MRI and selected the top four high-performance sequences to develop the RFF model. Incorporating class structure information, the RFF can effectively integrate features from different MR sequences while ensuring that the fused features are more representative and discriminative, which has been proven to perform successfully in differentiating brain glioblastoma from single brain metastasis (AUC=0.92)[8]. Our findings emphasized the significance of integrating diverse MRI sequences into the radiomics analysis of BC, as it has the potential to improve the precision of molecular subtype classification.Conclusion
We introduced a multiparametric MR-based radiomics feature fusion model that mimics the radiologists’ diagnostic approach to identify different molecular receptors of breast cancer preoperatively. The RFF strategy offers an effective and reliable tool with significant potential for breast tumor diagnosis and prognostic prediction.Acknowledgements
No acknowledgements found.References
[1] Zhang Y, Chen J, Lin Y, et al. Prediction of breast cancer molecular subtypes on DCE-MRI using convolutional neural network with transfer learning between two centers[J]. European Radiology, 2021,31(4):2559-2567.
[2] Qin Y, Tang C, Hu Q, et al. Assessment of Prognostic Factors and Molecular Subtypes of Breast Cancer With a Continuous-Time Random-Walk MR Diffusion Model: Using Whole Tumor Histogram Analysis[J]. J Magn Reson Imaging, 2022.
[3] Xie T, Wang Z, Zhao Q, et al. Machine Learning-Based Analysis of MR Multiparametric Radiomics for the Subtype Classification of Breast Cancer[J]. Frontiers in Oncology, 2019,9.
[4] van Griethuysen J, Fedorov A, Parmar C, et al. Computational Radiomics System to Decode the Radiographic Phenotype[J]. Cancer Res, 2017,77(21):e104-e107.
[5] Lee J Y, Lee K, Seo B K, et al. Radiomic machine learning for predicting prognostic biomarkers and molecular subtypes of breast cancer using tumor heterogeneity and angiogenesis properties on MRI[J]. European Radiology, 2021.
[6] Leithner D, Bernard-Davila B, Martinez D F, et al. Radiomic Signatures Derived from Diffusion-Weighted Imaging for the Assessment of Breast Cancer Receptor Status and Molecular Subtypes[J]. Molecular Imaging and Biology, 2020,22(2):453-461.
[7] Haghighat M, Abdel-Mottaleb M, Alhalabi W. Discriminant Correlation Analysis: Real-Time Feature Level Fusion for Multimodal Biometric Recognition[J]. IEEE transactions on information forensics and security, 2016,11(9):1984-1996.
[8] Wu J, Liang F, Wei R, et al. A Multiparametric MR-Based RadioFusionOmics Model with Robust Capabilities of Differentiating Glioblastoma Multiforme from Solitary Brain Metastasis[J]. Cancers (Basel), 2021,13(22).
Figures