4597
Microcalcification Detection and Differentiation in Breast Cancer using Ultrashort Echo Time (UTE) MRI1Aberdeen Biomedical Imaging Centre, Institute of Medical Sciences, School of Medicine, Medical Sciences and Nutrition, University of Aberdeen, Aberdeen, United Kingdom, 2Pathology Department, Aberdeen Royal Infirmary, Aberdeen, United Kingdom, 3Breast Unit, Broomfield Hospital, Mid and South Essex NHS Trust, Essex, United Kingdom, 4Newcastle Magnetic Resonance Centre, Translational and Clinical Research Institute, Faculty of Medical Sciences, Newcastle University, Newcastle, United Kingdom
Synopsis
Keywords: Breast, Breast, Microcalcification UTE
Motivation: Ultra short echo time (UTE) has been developed to capture the rapid signal decay of short T2* species, to overcome the insensitivity of conventional MRI towards micro-calcification, a central prognostic marker of breast cancer.
Goal(s): To examine the degree of calcification in breast tumour specimens using UTE.
Approach: The degree of calcification of whole tumour from 20 specimens freshly excised from female patients with breast cancer was derived using dual-echo UTE protocol, with correlation against histological findings.
Results: The degree of calcification was significantly different between malignant and non-calcified tissue, with no significant correlation to Ki-67 and NPI scores.
Impact: Ultra-short echo time (UTE) enhances the sensitivity to micro-calcifications in the breast, through dual-echo approach to maximise the signal of short T2* species. Clinical implementation of UTE can enhance assessment of microcalcification and improve prognostic value of breast cancer imaging.
Introduction
The presence of calcium in solid form, known as calcification, is a central feature in breast cancer (BC)1. The detection and classification of calcification in BC holds significant prognostic value in treatment planning2. Mammography, as the only current clinical radiological approach sensitive to the presence of calcification, cannot reveal the precise classification of calcification3. Ultrashort Echo Time Ultrashort Echo Time (UTE) imaging, a novel radiological method, addresses the limitation of conventional MRI to primarily soft tissue application by capturing rapid signal decay in solid state matters such as calcification. However, UTE demands non-cartesian scanning trajectory and high-performance scanner hardware to minimise the time lag between excitation and signal detection, and only became adequately robust and available on clinical scanners recently4. We therefore set out to examine the feasibility of UTE imaging in identifying histological characteristics of microcalcifications in freshly excised breast tumours.Methods
Twenty breast tumour specimens were removed from female patients undergoing wide local excision, mean (range) age of 57 (35–78) years, with invasive ductal carcinoma: grade II (10)/grade III (10). The fresh specimens were immediately placed in 10% buffered solution of formalin after surgery. UTE imaging was performed to derive degree of calcification, and standard pathological analysis was conducted to determine the calcification status, Nottingham Prognostic Index (NPI) and proliferative activity marker Ki-67. The study was approved by the North West-Greater Manchester East Research Ethics Committee (REC reference number: 16/NW/0221), and signed written informed consent was obtained prior to the study.Image Acquisition: The specimens were scanned on a 3T whole-body MRI scanner (Achieva TX, Philips Healthcare, Best, Netherlands) using a 32-channel receiver coil for high sensitivity detection and a body coil for uniform transmission. For tumour localisation, anatomical images were acquired using standard T1-weighted and T2-weighted sequences with conventional diffusion weighted images (2 b-values of 0 and 800 sec/mm2). The UTE images were acquired with a 3D-radial dual-echo UTE sequence, with echo times (TE1) of 0.17 ms and (TE2) 4.60 ms, repetition time (TR) of 8.5 ms, FOV of 141 × 141 mm2, voxel size of 2.2 × 2.2 × 2.2 mm3. To understand the signal dynamics of calcification, two additional UTE acquisitions were performed with TE1 at 0.2 and 0.6 ms, and TE2 at 6.9 ms, and TR at 18 ms.
Image Analysis: The whole tumour was manually delineated with the reference to T1 and T2 anatomical images in MATLAB (MathWorks Inc., Natick, USA) (Figure 1). Subsequently, the signal intensity of the two echoes were derived as the mean of the image intensity within the whole tumour for each echo. The degree of calcification was computed as the signal difference between the two echoes normalised by the long echo.
Statistical Analysis: All statistical analysis was carried out using SPSS software (Release 27.0, SPSS Inc, IL, USA). Degree of calcification from UTE between histological calcification classes was compared using one-way ANOVA. A Tukey's HSD post hoc tests were conducted to indicate the significance of differences among the three calcification groups. Spearman’s correlation tests were performed between degree of calcification against NPI and Ki-67 scores.
Results
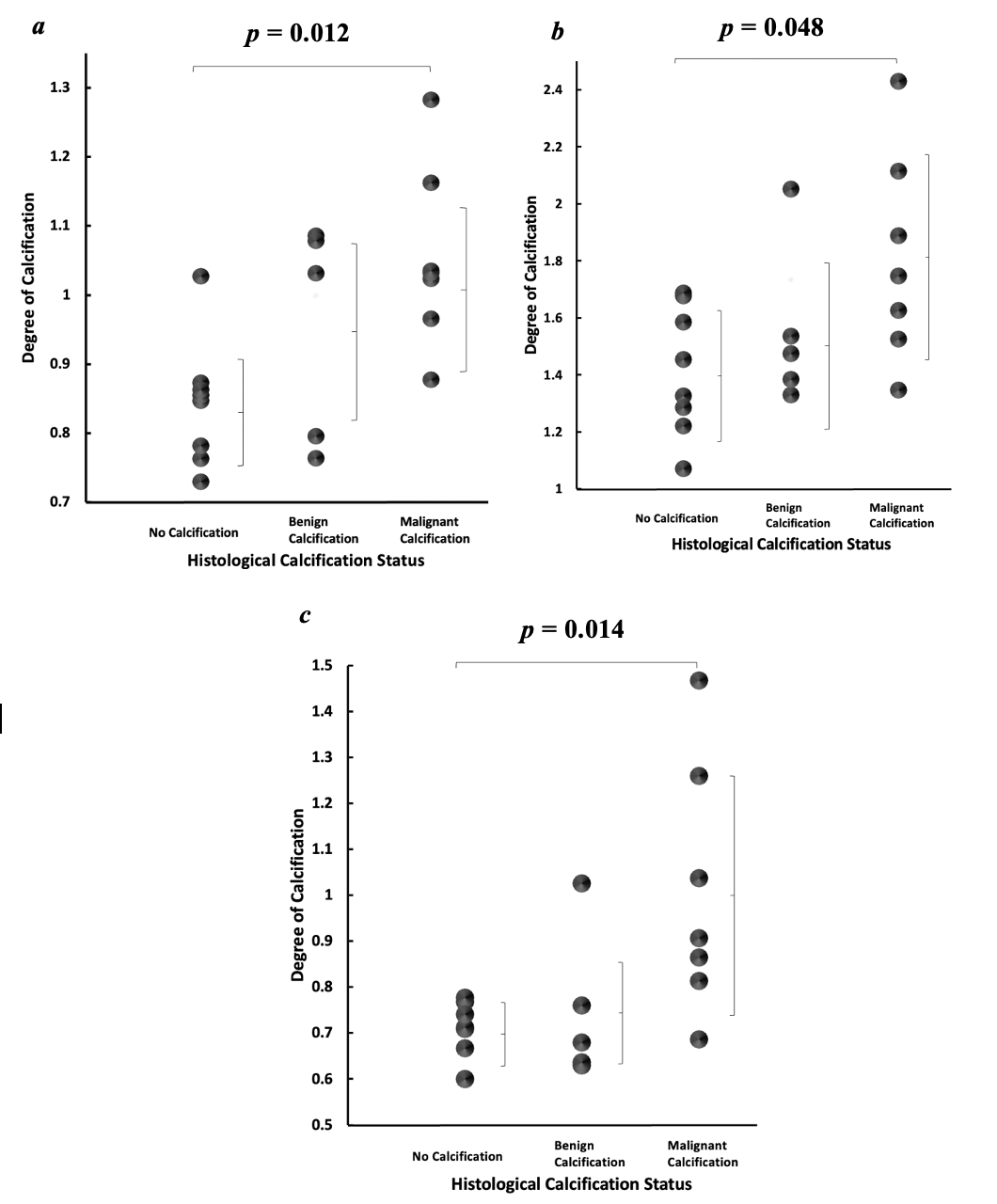
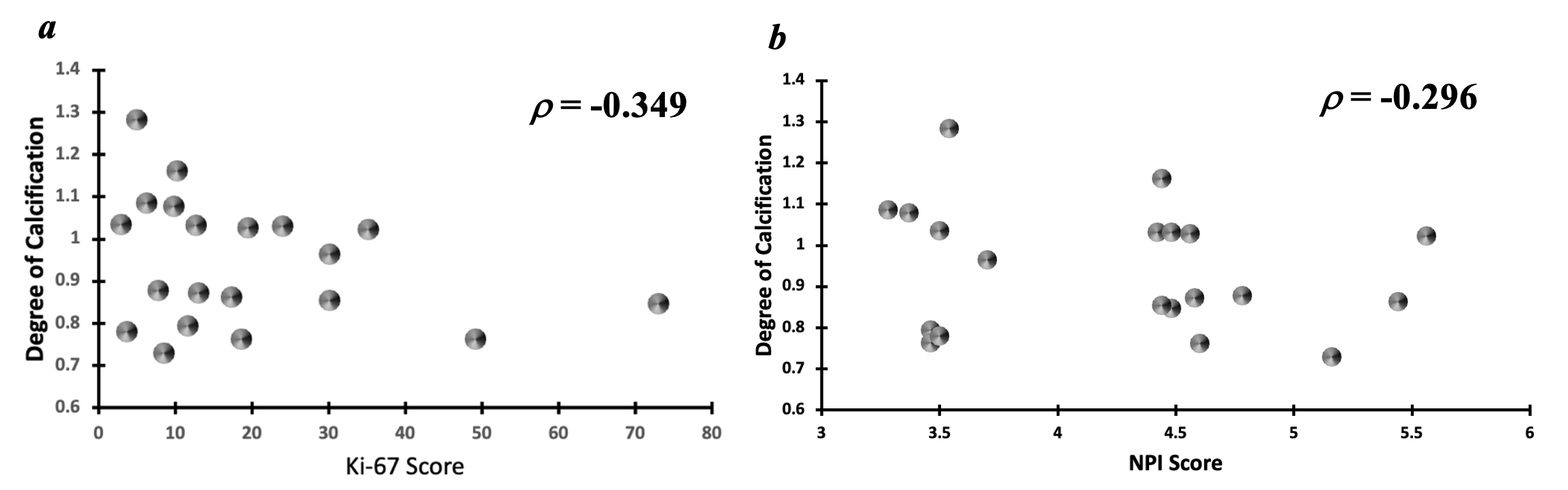
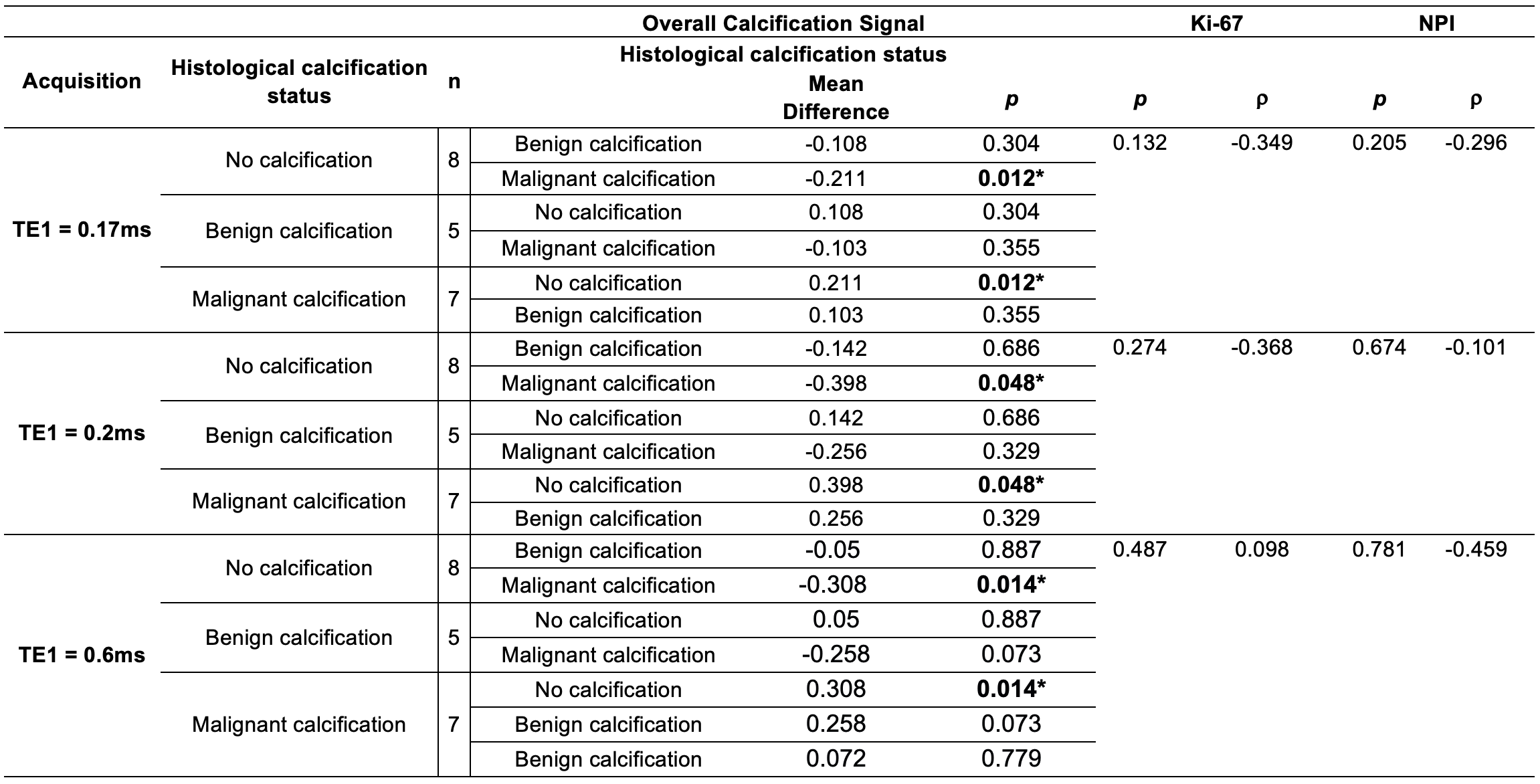
There was a significant difference (p = 0.012) in the degree of calcification between specimens with malignant calcification (1.054 ± 0.132) and specimens with no calcification (0.842 ± 0.091) for images acquired at TE1 of 0.17 ms (Table1). There was a significant difference in the degree of calcification between specimens with malignant calcification and specimens with no calcification for images acquired at TE1 of 0.2 ms (p = 0.048) and TE1 of 0.6ms (p = 0.014) (Figure 2). There was no significant difference (p = 0.355) in the degree of calcification between specimens with malignant calcification (1.054 ± 0.132) and benign calcification (0.951 ± 0.158) across all acquisitions. There was no significant correlation between the degree of calcification against NPI and Ki-67 scores (Figure 3).Discussion
UTE enhances the detection of short T2* species and may have potential in the detection of solid-state signal from calcifications in breast tumours. Although UTE showed a potential in sensitivity to calcified tumours, further work is required for non-invasive differentiation of calcification classes. Malignant calcifications and benign calcifications are typically associated with different chemical composition crystal structures. Nonetheless, benign calcifications can possess crystal structures with the same chemical composition as malignant calcifications, which introduces challenges in the differentiation of solid state signals5. No correlation between histologic calcification classes and NPI and Ki-67 scores was found, although it is reported to have an association with calcified tumours6,7.Conclusion
Tumours with malignant calcification may be differentiated from tumours without calcification using UTE imaging.Acknowledgements
This work was funded by the NHS Grampian Endowment Research Fund. Yazan Ayoub’s PhD study is supported by the Elphinstone PhD Scholarship.References
1. DeSantis CE, Ma J, Gaudet MM, Newman LA, Miller KD, Goding Sauer A, Jemal A, Siegel RL. Breast cancer statistics, 2019. CA Cancer J Clin. 2019 Nov;69(6):438-451.2. Baker, R. et al. New relationships between breast microcalcifications and cancer. British Journal of Cancer, (2010); 103 (7), 1034–1039.
3. Bennani-Baiti, B. & Baltzer, P. A. MR Imaging for Diagnosis of Malignancy in Mammographic Microcalcifications: A Systematic Review and Meta-Analysis. Radiology. (2017); 283 (3), 692–701.
4. Du J, Bydder M, Takahashi AM, Carl M, Chung CB, Bydder GM. Short T2 contrast with three-dimensional ultrashort echo time imaging. Magn Reson Imaging. (2011);29(4):470-82
5. Morgan M, Cooke M, Mc Carthy G, Microcalcifications Associated with Breast Cancer: An Epiphenomenon or Biologically Significant Feature of Selected Tumors? Journal of Mammary Gland Biology and Neoplasia, Vol. 10, No. 2, (2005); 181:187
6. Mun HS, Shin HJ, Kim HH, Cha JH, Kim H. Screening-detected calcified and non-calcified ductal carcinoma in situ: differences in the imaging and histopathological features. Clin Radiol. 2013 Jan;68(1):e27-35.
7. Qiu X, Mei J, Yin J, Wang H, Wang J, Xie M. Correlation analysis between expression of PCNA, Ki-67 and COX-2 and X-ray features in mammography in breast cancer. Oncol Lett. 2017 Sep;14(3):2912-2918.
Figures
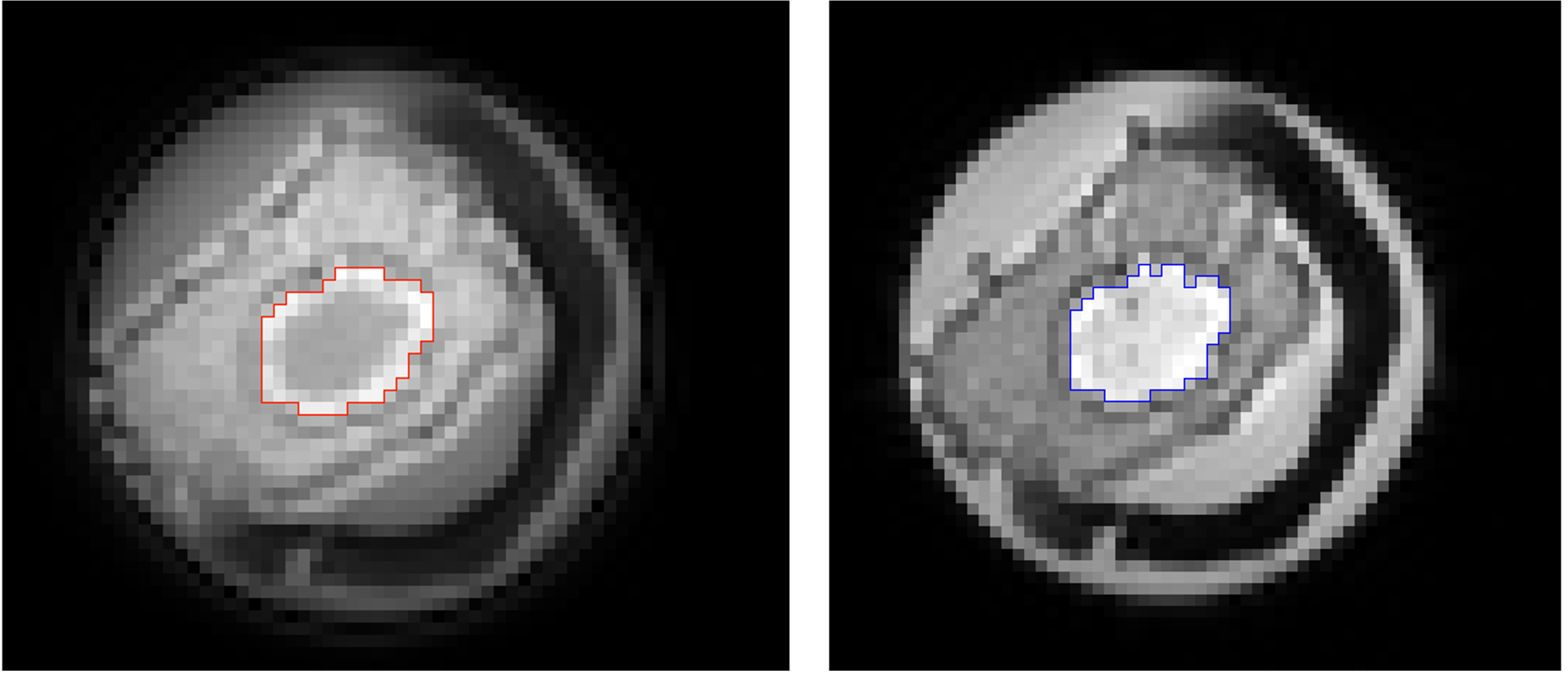
Figure 1: Delineation of whole tumour region on dual echo UTE image:(A) Time of Echo 1 (TE1) at 0.17ms and (B) Time of Echo 2 (TE2) at 4.6ms