4595
Development and external validation of a combined clinical-mammographic-MRI model for differentiating benign and malignant NME breast lesions1General Hospital of Ningxia Medical University, Yinchuan, China
Synopsis
Keywords: Breast, Breast, Clinical, Mammography, MRI, Nonmass enhancement breast lesions
Motivation: Differential diagnosis of nonmass enhancement (NME) breast lesions is difficult.
Goal(s): A combined clinical-mammographic-MRI based on DWI model can distinguish benign and malignant NME lesions.
Approach: We retrospectively enrolled consecutive female patients with NME breast lesions who underwent pretreatment MG and breast MRI as the development cohort and prospectively collected eligible candidates as an internal validation group and an external validation group at our centre. A combined discriminatory model was developed through multivariable logistic regression and was validated internally and externally.
Results: The combined model incorporating mammography, MRI, and clinical variables showed good discriminability in the development, internal validation, and external validation cohorts.
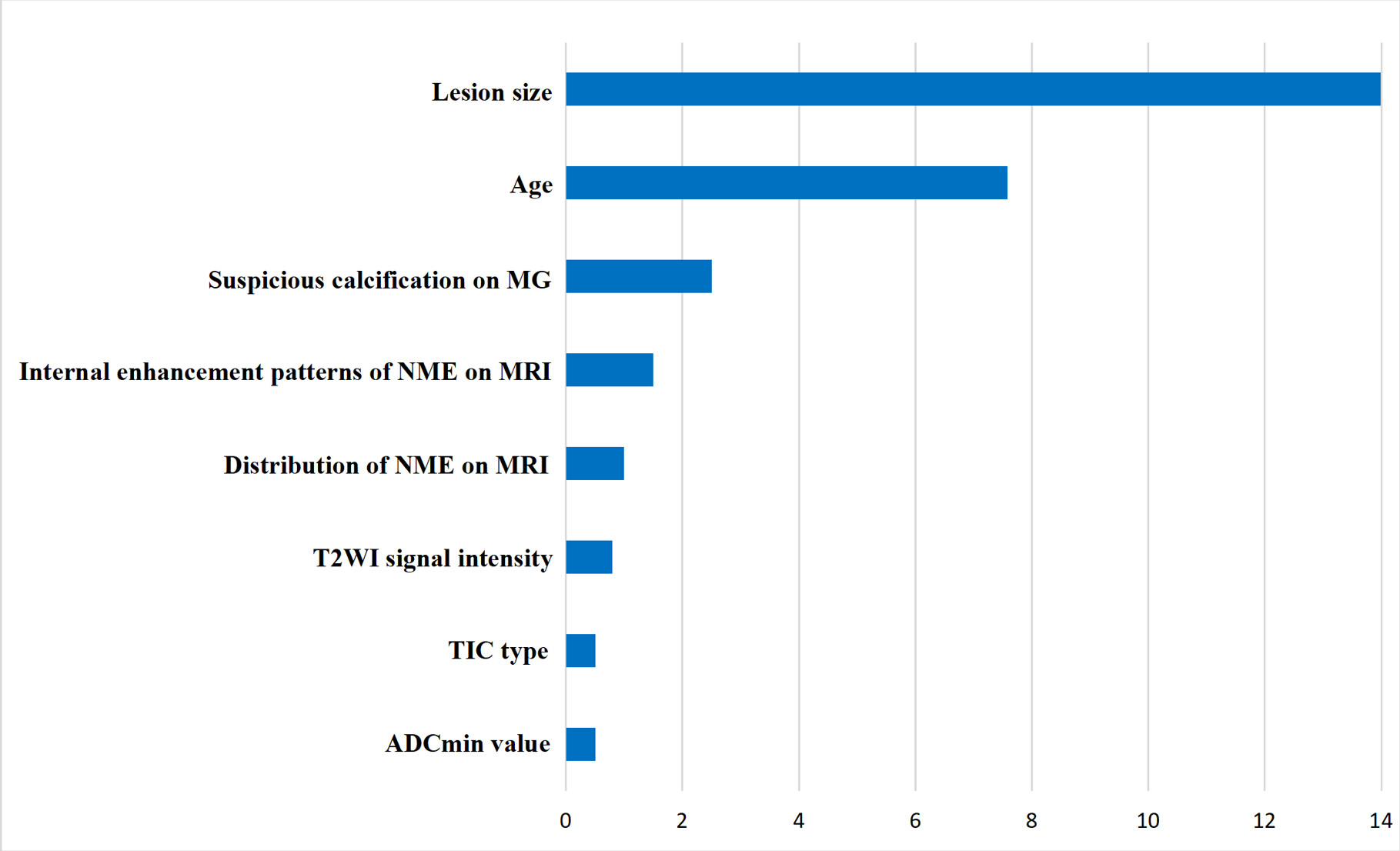
Impact: Based on SHAP analysis, suspicious calcification on mammography and internal NME patterns were significant contributors to the performance of the model, and radiologists and clinicians should improve their awareness of complementary mammography to improve diagnostic performance in classifying NME lesions.
Introduction
According to the 5th edition of the Breast Imaging Reporting and Data System lexicon (BI-RADS) [1], a nonmass enhancement (NME) is defined as a small or large enhanced region without a space-occupying effect on breast magnetic resonance imagine (MRI). NME lesions account for 17.8% of breast lesions. Although NME lesions are the main manifestations of ductal carcinoma in situ (DCIS), they can also be found in invasive cancer and benign lesions, especially mastitis [2]. Some 54% and 46% of NME lesions are diagnosed as breast cancer and benign breast lesions, respectively, and there is significant morphologic overlap between the two [1-2].Among all breast imaging modalities, MRI offers the highest sensitivity in detecting cancer, but the high sensitivity is accompanied by a specificity of only 72% [3]. Imbriaco et al [4] reported that NME lesions are the major cause of false-positive breast MRI findings and that with MRI functional imaging, the apparent diffusion coefficient (ADC) and kinetic enhancement patterns, which are more related to masses, are insufficient for characterizing NME lesions [5]. Additionally, MRI may be false negative due to cognitive errors that result in the misinterpretation or mischaracterization of the margins and shapes of abnormalities as benign [6]. A poor display of calcification is another major drawback of MRI [7]. Therefore, using only MRI for the differential diagnosis of NME lesions is challenging and necessitates further imaging, tissue sampling, or follow-up examinations to make a clear diagnosis.Ultrasound (US) is an important tool in the screening and diagnosis of breast cancers. Its sensitivity to tiny calcifications is lower than that of mammography, it suffers from shortcomings in the diagnosis of DCIS, and an accurate diagnosis is difficult because of overlapping features of malignant and benign breast NMEs [2].Compared with MRI and US, mammography is widely recommended for early breast cancer detection, and it can decrease breast cancer mortality by 20% - 40% because of its extreme sensitivity to suspicious calcifications, which is helpful for evaluating NME breast lesions [8]. Numerous studies have demonstrated [9] that suspicious calcifications are present in 51% of malignant nonmass findings, versus 2% of benign nonmass findings. The malignancy of a nonmass finding is consistently associated with suspicious calcifications.NME lesions are a popular topic of research. In this issue of Radiology, den Dekker et al [7] report that clinical information has been combined with conventional MRI to investigate NME lesions to reduce the false-positive rate of MRI. However, few studies have investigated NME lesions using mammography and conventional MRI to improve diagnostic performance. Therefore, the purpose of our study was to develop and validate a combined model to differentiate benign from malignant NME lesions of various pathological types by combining mammography, MRI and clinical features. External validation and evaluation were performed in NME patients with intravoxel incoherent motion (IVIM) sequence to explore the feasibility of generalizing the based on diffusion weighted imaging (DWI) combined model to MRI with IVIM.Methods
We retrospectively enrolled consecutive female patients pathologically confirmed or followed up with NME breast lesions who underwent pretreatment MG and breast MRI between January 2018 and April 2022 as the development cohort (n = 501, DWI) and prospectively collected eligible candidates between May 2022 and October 2023 as an internal validation group (n = 195, DWI) and an external validation group (n = 58, IVIM) at our centre. Clinical, mammographic, and MRI data were collected. A combined discriminatory model was developed through multivariable logistic regression and was validated internally and externally.Results
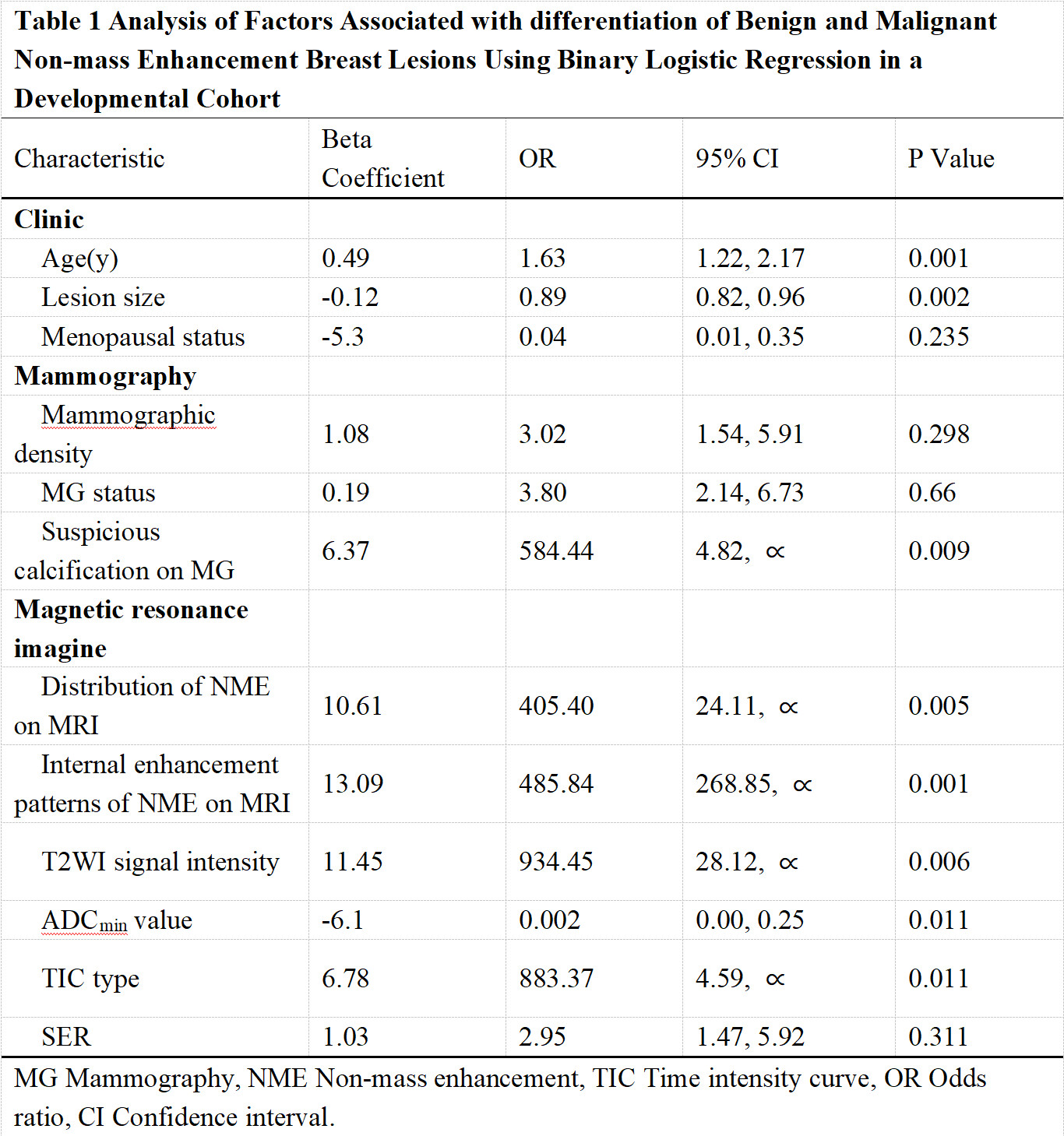
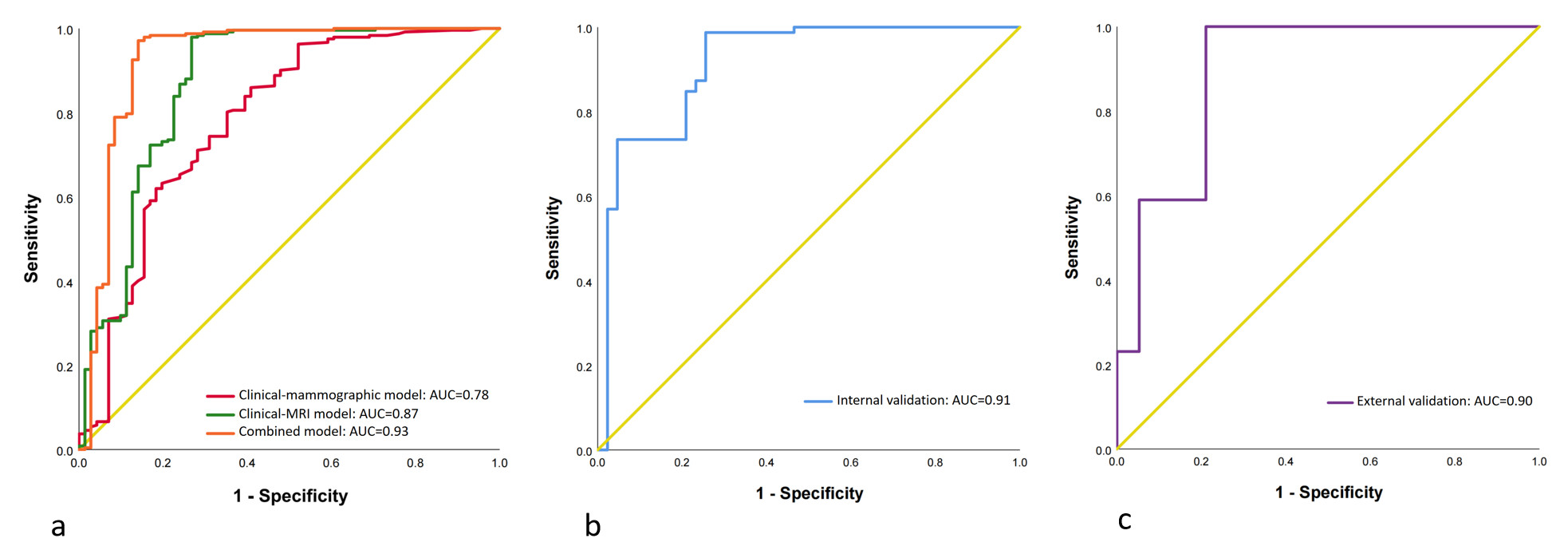
Age, lesion size, suspicious calcification on MG, distribution of NME and internal NME patterns on MRI, T2WI signal intensity, ADCmin and TIC type were independently associated with the differentiation of NME breast lesions (Table 1) (Fig.1). The combined model incorporating mammography, MRI, and clinical variables showed good discriminability in the development, internal validation, and external validation cohorts (AUC = 0.93, 95% CI: 0.88, 0.98; AUC = 0.91, 95% CI: 0.86, 0.97; and AUC = 0.90, 95% CI: 0.79, 0.99, respectively) (Fig.2). The combined model had excellent calibration capacity in all three cohorts (mean absolute error = 0.02, 0.026 and 0.021, respectively).Conclusions
A combined clinical-mammographic-MRI based on DWI model can distinguish benign and malignant NME lesions. It could be generalized to MRI with IVIM.Acknowledgements
This study thanks the support from Key research and development (R&D) project of the Ningxia Hui Autonomous Region (NO. 2022BEG03166); Ningxia Natural Science Foundation (NO. 2023AAC03611); New Master Training Program of General Hospital of Ningxia Medical University (NO.YKDZY2022013).References
1. Spak DA, Plaxco JS, Santiago L et al (2017) BI-RADS® fifth edition: A summary of changes. Diagn Interv Imaging 98:179-1902.
2.Wang L, Chang L, Luo R et al (2022) An artificial intelligence system using maximum intensity projection MR images facilitates classification of non-mass enhancement breast lesions. Eur Radiol 32:4857-48673.
3. Mann RM, Hooley R, Barr RG et al (2020) Novel approaches to screening for breast cancer. Radiology 297:266-285
4. Imbriaco M (2021) Reducing false-positive screening MRI rates in women with extremely dense breasts. Radiology 301:293-2945.
5. Avendano D, Marino MA, Leithner D et al (2019) Limited role of DWI with apparent diffusion coefficient mapping in breast lesions presenting as non-mass enhancement on dynamic contrast-enhanced MRI. Breast Cancer Res 21:1366.
6. Korhonen KE, Zuckerman SP, Weinstein SP et al (2021) Breast MRI: false-negative results and missed opportunities. Radiographics 41:645-6647.
7. den Dekker BM, Bakker MF, de Lange SV et al (2021) Reducing false-positive screening MRI rate in women with extremely dense breasts using prediction models based on data from the DENSE trial. Radiology 301: 283-2928.
8. Duffy SW, Tabár L, Yen AM et al (2020) Mammography screening reduces rates of advanced and fatal breast cancers: Results in 549,091 women. Cancer 126:2971-29799.
9. Horvat JV, Keating DM, Rodrigues-Duarte H et al (2019) Calcifications at digital breast tomosynthesis: imaging features and biopsy techniques. Radiographics 39:307-318
Figures