4594
MRI Diagnosis of Lesions Presenting as Architectural Distortion on DBT: Comparison of Diagnostic Performance Using BI-RADS and Radiomics Models1First affiliated hospital of Wenzhou Medical University, Wenzhou, China, 2University of California, Irvine, Irvine, CA, United States, 3University of California, Irvine, Irvine, China
Synopsis
Keywords: Breast, Breast
Motivation: Diagnosis of lesions shown as architectural distortion (AD) on DBT is challenging, and breast MRI may help.
Goal(s): To compare the diagnostic performance of 60 cases using reading based on BI-RADS of DBT and MRI, Kaiser score, and radiomics models.
Approach: In addition to comparing the diagnostic performance, features shown on DBT and MRI, and the distribution in different MRI BI-RADS categories, were reported.
Results: The malignant rate of AD varied in associated features and MRI-RADS groups. MRI showed better diagnostic performance than DBT. When using radiomics models, the accuracy was almost the same, but the AUC of DBT+MRI fused model improved.
Impact: Diagnosis of lesions presenting as AD on DBT can be improved with more understanding of associated features, as well as the predictive features based on the supplementary MRI.
Introduction
Architectural distortion (AD) is the third most common mammographic demonstration of breast cancer, which could be the early appearance of malignancy. With the increasing use of digital breast tomosynthesis (DBT) in clinical practice, the visualization of AD has been improved. However, the accurate diagnosis of AD lesions on DBT is still challenging. A wide range of malignancy rates of AD was reported, showing a positive predictive value of 10.2% - 74.5%. Research studies have explored the diagnostic value of MRI for AD lesions, showing that breast MRI may provide additional information to make a correct diagnosis. The objectives of this study were: (1) to compare the clinical diagnosis determined from DBT and MRI, respectively; (2) to compare the diagnostic performance in different AD groups (with and without regional nodule or density, with and without suspicious microcalcifications, AD as prominent or accompanied features); (3) to apply radiomics models to compare the diagnostic performance of using MRI and DBT alone, and the combined MRI+DBT model.Methods
Sixty patients who showed AD on DBT and who also had MRI showing lesions at a corresponding location were analyzed, including 38 malignant and 22 benign. DBT images were reviewed by two radiologists to identify the suspicious area showing AD. The diagnostic performance using DBT BI-RADS (³4B), MRI BI-RADS (³4B), and MRI Kaiser Score (KS 5-11) as malignant was reported and compared. For DBT, whether there was an associated nodule or density, suspicious microcalcifications, and whether AD was the prominent or accompanied feature was evaluated. The malignancy rate in the whole group and each subgroup was compared. MRI features of 60 lesions, including the signal intensity (SI) of T2WI, characteristic T2WI, peri-lesion edema, SI of DWI, lesion morphology (mass or non-mass enhancement), margin, DCE kinetic curve, internal enhancement pattern (IEP), fibroglandular tissue (FGT) density category, and background parenchymal enhancement (BPE) were reviewed by two readers and compared. The largest 1-D dimension, 2-D tumor area on the largest slice, and ADC were measured and compared. Lastly, we applied radiomics models for the diagnosis of lesions on MRI and DBT to test the performance, and further, we combined the features extracted from MRI and DBT together to train a combined model.Results
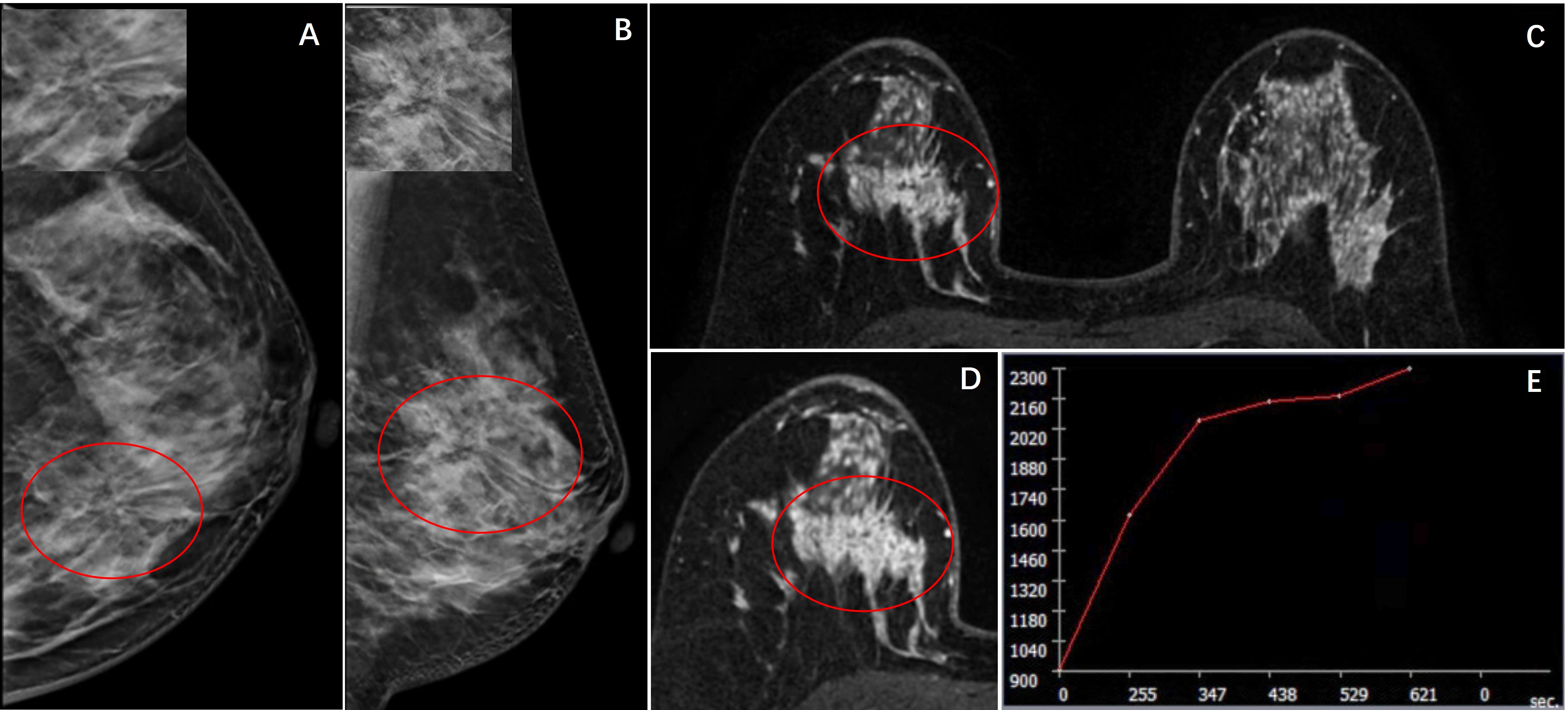
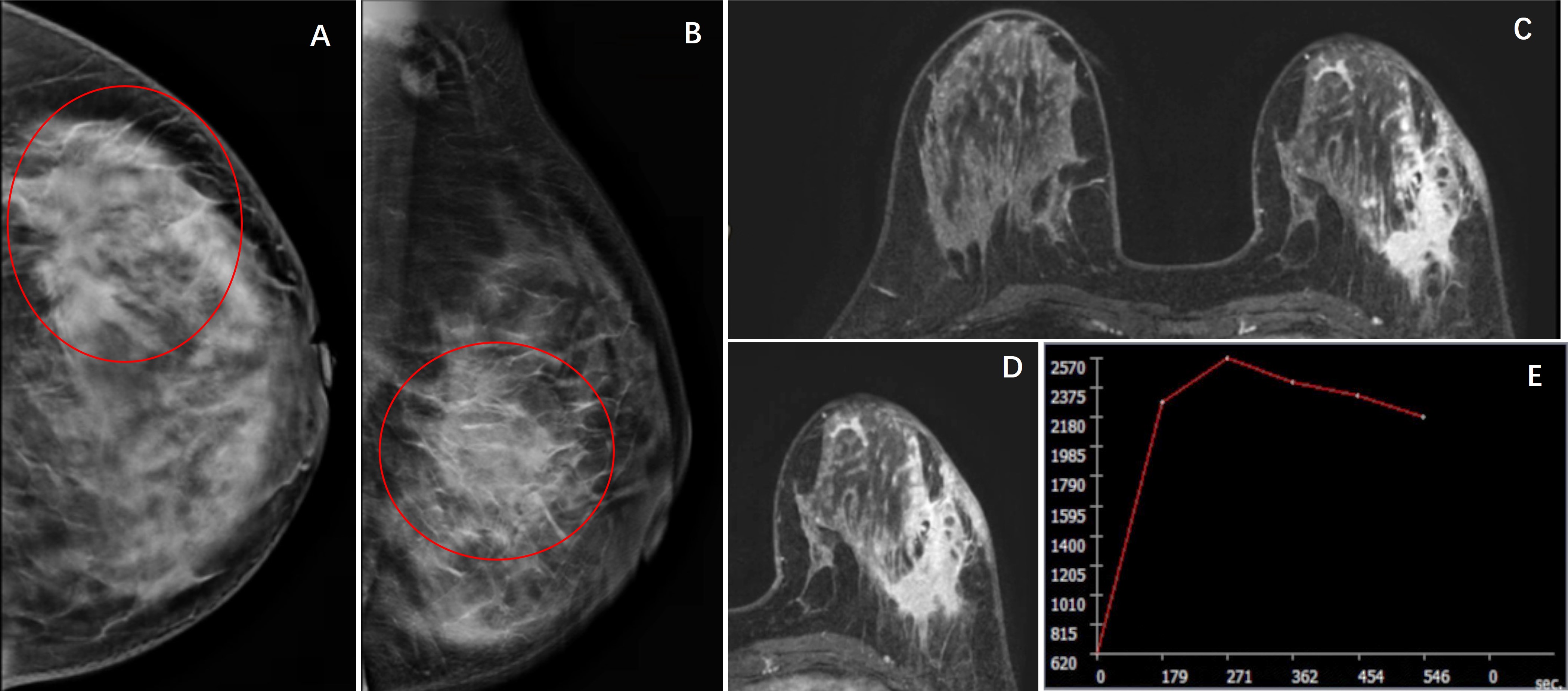
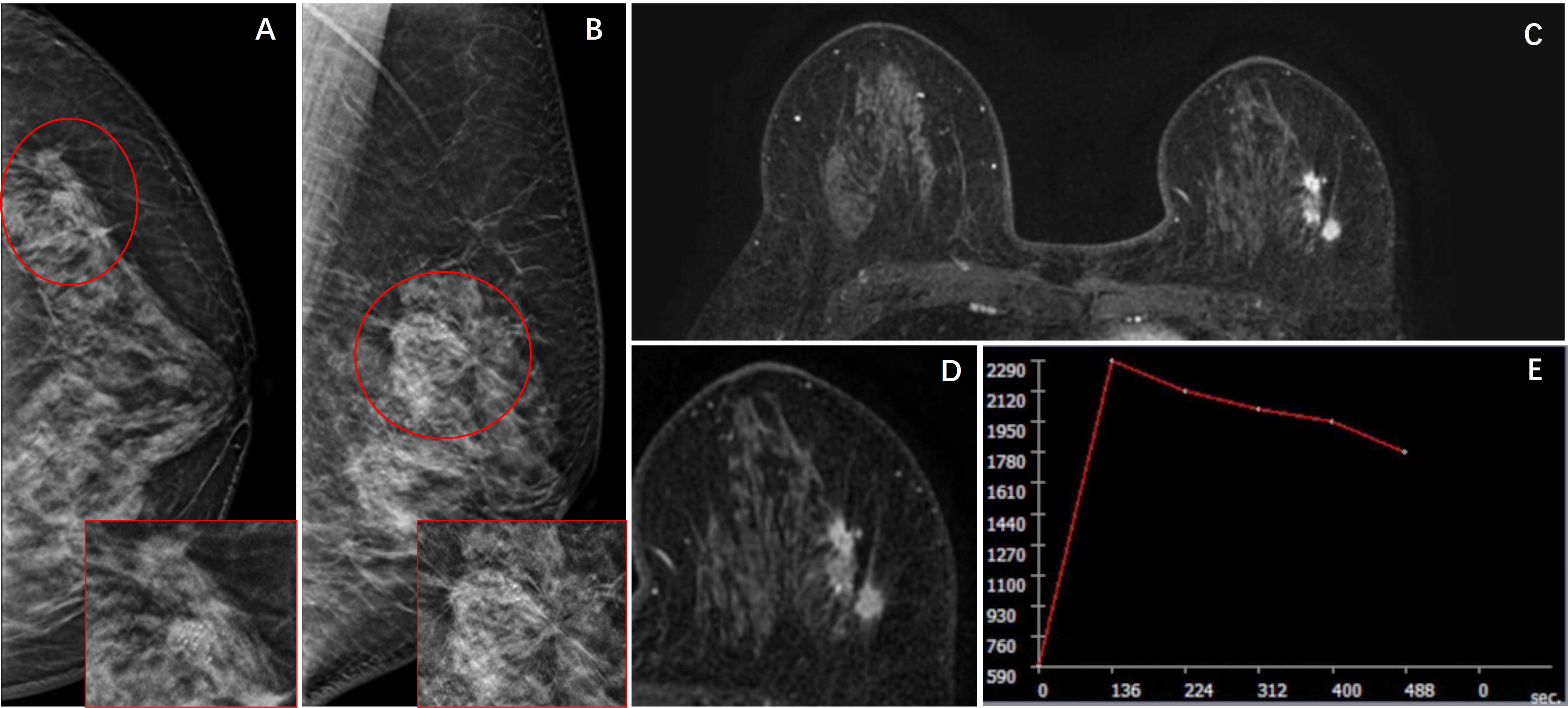
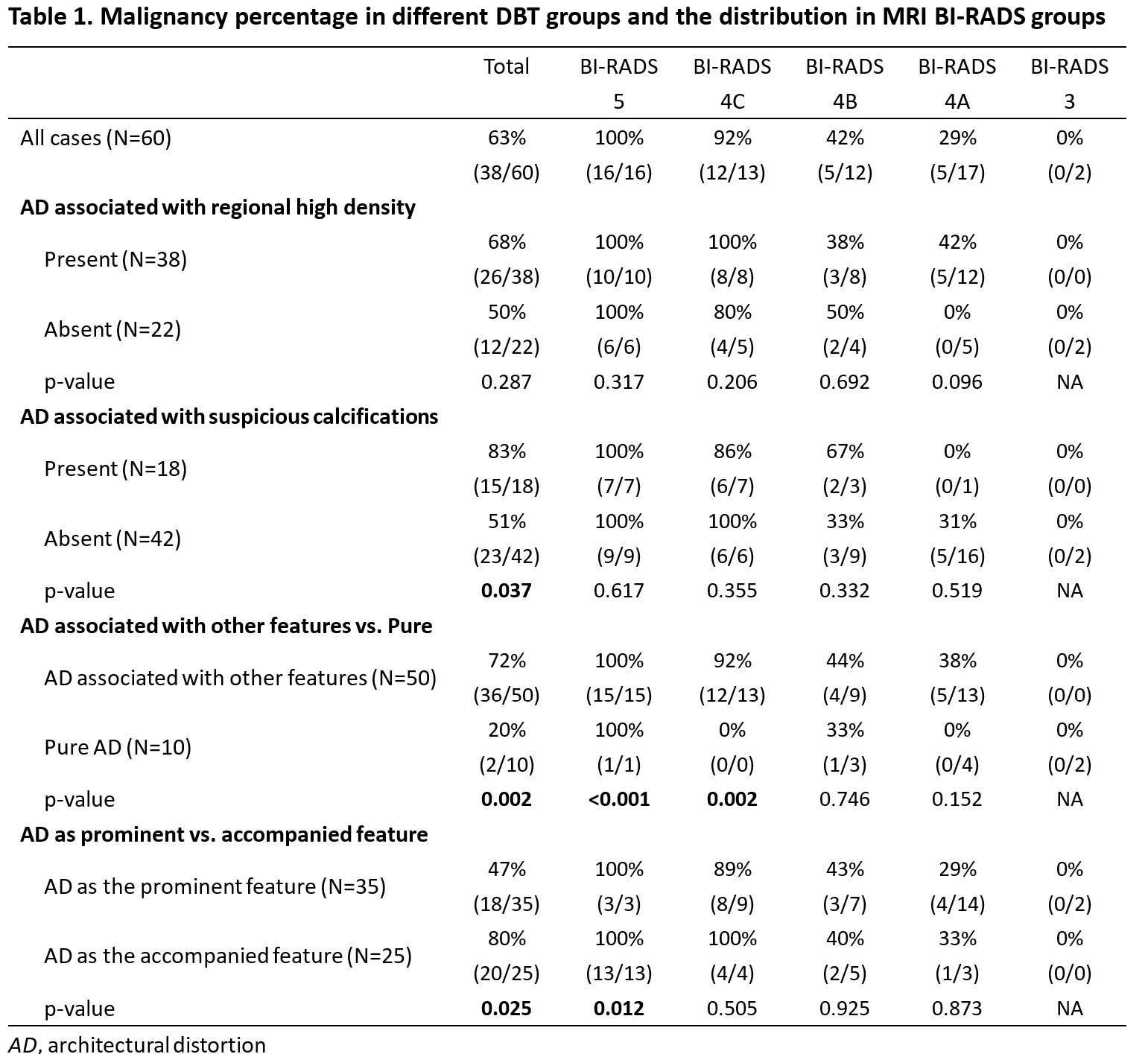
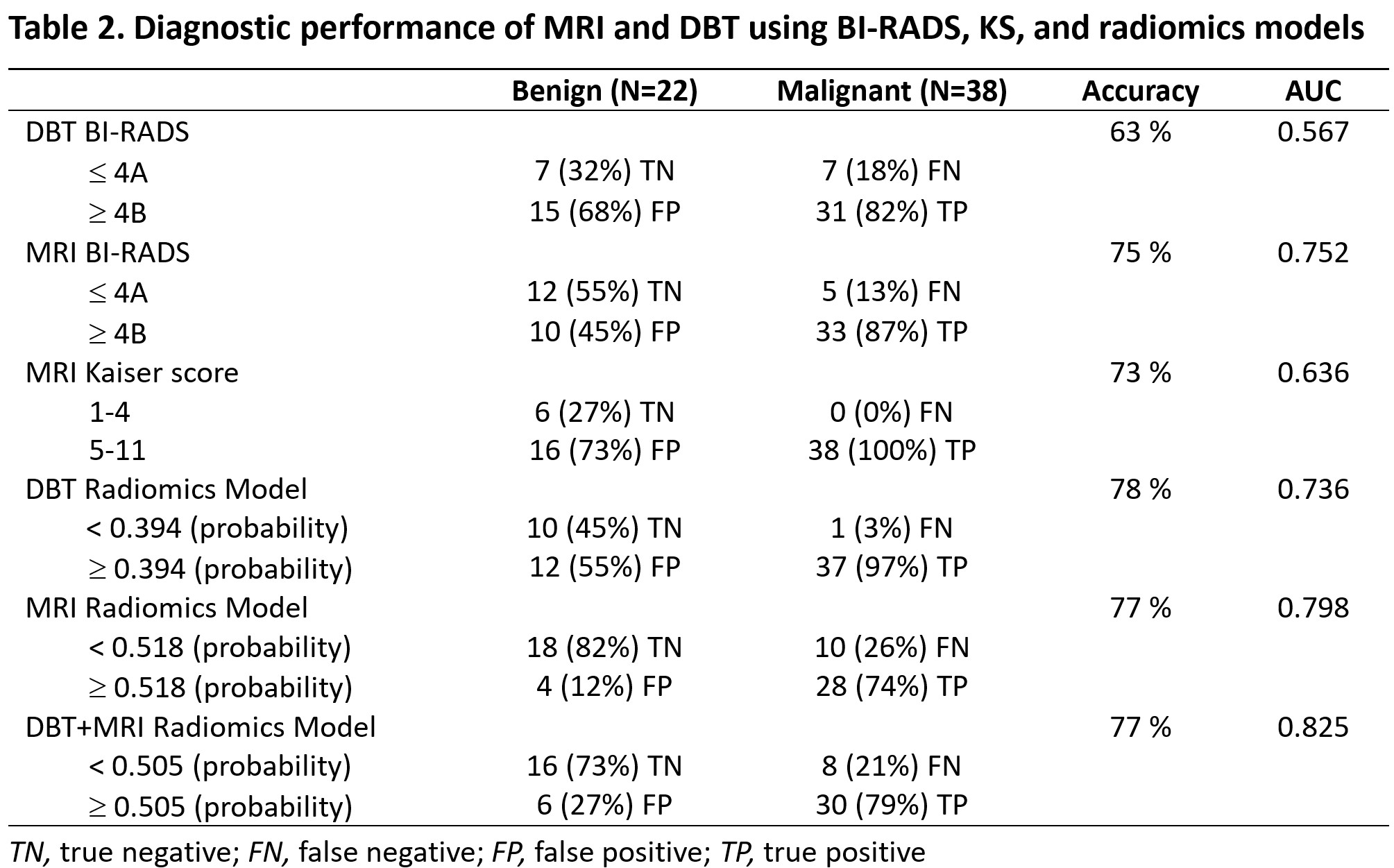
Of the 60 AD cases, 16, 13, 12, 17, and 2 cases had MRI BI-RADS of 5, 4C, 4B, 4A, and 3, with the malignant rate of 100%, 92%, 42%, 29%, and 0%, respectively (Table 1). When AD cases were associated with density or suspicious calcifications, the malignant rate was higher, and they were more likely to present as MRI BI-RADS 5 or 4C. There were only 10 cases showing pure AD, and 2 of them were malignant (20%), which was significantly lower than the 72% (36/50) in cases with other features. Three cases presenting AD on DBT are shown. The diagnostic results are summarized in Table 2. The overall accuracy was 63% based on BI-RADS of DBT, 75% based on BI-RADS of MRI, and 73% based on KS. When applying the previously developed radiomics models to test the performance, the accuracy and AUC was 78% and 0.736 for the DBT model, and 77% and 0.798 for the MRI model. When the DBT and MRI radiomics features were combined to retrain a fused model, the accuracy and AUC was 77% and 0.825.Discussion
Although AD represents a small prevalence of mammographic lesions, it is crucial to accurately diagnose when the AD lesion is detected. Our results showed the malignancy rate of AD shown as accompanied feature was significantly higher than it shown as prominent feature in whole group, so was in MRI BI-RADS 5 group. The malignant rate of different MRI BI-RADS groups didn’t show significant difference whether AD was associated with regional high density. When AD lesions were associated with suspicious calcifications, the malignant rate was significantly higher than those not. Compared with pure AD, AD with other associated features had significantly higher malignant rate, so was in MRI BI-RADS 5 and 4C groups. The results showed heterogeneous signal of T2WI, high signal intensity of DWI, washout DCE kinetic curve, non-homogeneous EPI, heterogeneously dense FGT, minimal BPE and larger area was seen more in malignant group. MRI BI-RADS (75%) and KS (73%) showed higher mean accuracy than DBT (63%). When using radiomics models to diagnose, the accuracy of DBT (78%), MRI (77%) and fused model (77%) was almost the same, but the AUC of fused model improved. MRI BI-RADS demonstrated better diagnostic performance than DBT, and it may be further improved by DBT and MRI fused radiomics model.Acknowledgements
This study was supported in part by Research Incubation Project of First Affiliated Hospital of Wenzhou Medical University (No. FHY2019085), Wenzhou Science & Technology Bureau (No. Y20210232), Zhejiang Provincial Natural Science Foundation of China (LY21F020030) and Key Laboratory of Intelligent Medical Imaging of Wenzhou (No. 2021HZSY0057).References
[1]. Gaur S, Dialani V, Slanetz PJ, et al. Architectural distortion of the breast. AJR Am J Roentgenol. 2013, 201:W662-670.
[2]. Bahl M, Lamb LR, Lehman CD. Pathologic Outcomes of Architectural Distortion on Digital 2D Versus Tomosynthesis Mammography. AJR Am J Roentgenol. 2017, 209:1162-1167.
[3]. Villa-Camacho JC, Bahl M. Management of Architectural Distortion on Digital Breast Tomosynthesis With Nonmalignant Pathology at Biopsy. AJR Am J Roentgenol. 2022, 219:46-54.
[4]. Choudhery S, Johnson MP, Larson NB, et al. Malignant Outcomes of Architectural Distortion on Tomosynthesis: A Systematic Review and Meta-Analysis. AJR Am J Roentgenol. 2021, 217:295-303.
[5]. Bahl M, Baker JA, Kinsey EN, et al. Architectural Distortion on Mammography: Correlation With Pathologic Outcomes and Predictors of Malignancy. AJR Am J Roentgenol. 2015, 205:1339-1345.
[6]. Si L, Zhai R, Liu X, Yang K, et al. MRI in the differential diagnosis of primary architectural distortion detected by mammography. Diagn Interv Radiol. 2016, 22:141-150.
[7]. Mei H, Xu J, Yao G, et al. The diagnostic value of MRI for architectural distortion categorized as BI-RADS category 3-4 by mammography. Gland Surg. 2020, 9:1008-1018.
[8]. Amitai Y, Scaranelo A, Menes TS et al. Can breast MRI accurately exclude malignancy in mammographic architectural distortion? Eur Radiol. 2020, 30:2751-2760.
Figures