4593
Precision Diagnosis of BI-RADS4 Breast Lesions: A Promising Approach with DCE and 3D-MIP Parameters1First Affiliated Hospital of Dalian Medical University, Dalian, CHINA, Dalian, China, 2GE Healthcare, MR Research China, Beijing, China, Beijing, China
Synopsis
Keywords: Breast, Breast
Motivation: Breast cancer is a significant health concern for women. Accurate diagnosis of BI-RADS4 lesions is challenging, necessitating improved diagnostic indicators.
Goal(s): This study aims to enhance BI-RADS4 breast lesion diagnosis using DCE and 3D-MIP parameters, providing more precise insights.
Approach: We analyzed various parameters, identified independent factors, and combined vascular diameter difference with Slopemax for optimal diagnosis.
Results: The combination demonstrated superior diagnostic efficiency, differentiating benign from malignant lesions effectively.
Impact: This approach holds promise for early breast cancer diagnosis and improved patient care, offering clinicians a valuable tool for enhanced precision in BI-RADS4 lesion evaluation.
Introduction
Breast cancer ranks as the most prevalent malignancy among women, posing a significant threat to women's health and lives [1]. Imaging plays a pivotal role in the accurate diagnosis and treatment of breast cancer. Dynamic contrast-enhanced MRI (DCE-MRI) and maximum intensity projection (MIP) reconstruction technology offer multi-directional and multi-temporal imaging, enabling a clear and stereoscopic display of microvessel distribution around breast lesions[2]. However, differentiating benign and malignant breast lesions classified as BI-RADS4 remains challenging, necessitating more precise diagnostic indicators. This study aims to evaluate the differential diagnostic value of DCE-MRI-based intratumoral and peritumoral imaging features, with the goal of providing new insights into the early diagnosis and treatment of BI-RADS4 breast lesions.Methods
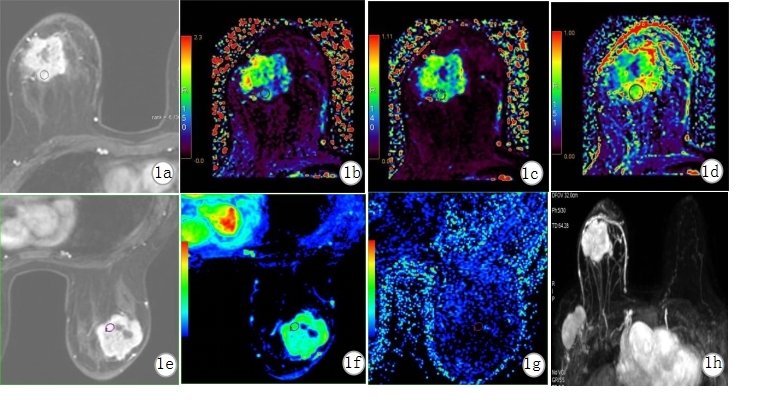
A retrospective analysis included female patients who underwent breast MRI examinations at the First Affiliated Hospital of Dalian Medical University between August 2018 and March 2023 and were categorized as BI-RADS4 with clear pathological results. A total of 102 cases were included in this study, including 43 cases of breast benign tumors and 59 cases of breast cancer confirmed by postoperative pathology.Intratumoral imaging features were assessed, encompassing DCE semi-quantitative parameters [Maximum slope of enhancement (Slopemax), Signal Enhancement Ratio (SER)], quantitative parameters [Leakage Space (Ve), Contrast Volume Transfer Constant (Ktrans), Velocity Constant (Kep)], and basic imaging features [Fibroglandular Tissue Content (FGT), Breast Background Substantial Enhancement (background parallel enhancement, BPE), time signal intensity curve (TIC) types]. Additionally, vascular information around the tumor, including AVS measurement (number of blood vessels, maximum diameter difference between affected and healthy sides of the tumor), was recorded (see Figure 1). Group comparisons were made for general information and imaging manifestations. Independent risk factors for developing BI-RADS4 breast malignancies were evaluated through logistic regression analysis. Independent sample t-tests compared differences between parameter groups. Univariate and multivariate logistic regression analyses were conducted. The diagnostic efficacy of single parameters and vascular-related indicators in distinguishing breast BI-RADS4 lesions was assessed using receiver operating characteristic (ROC) curves and area under the curve (AUC). AUC comparisons were performed using the Delong test.Results
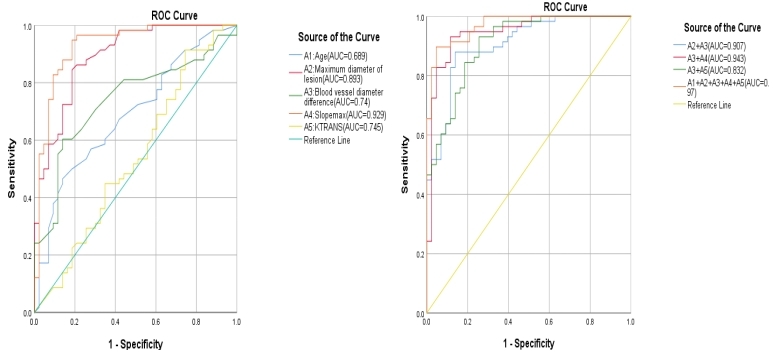
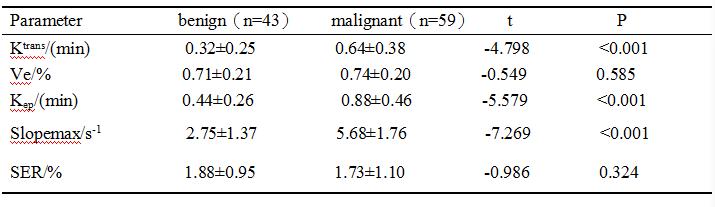
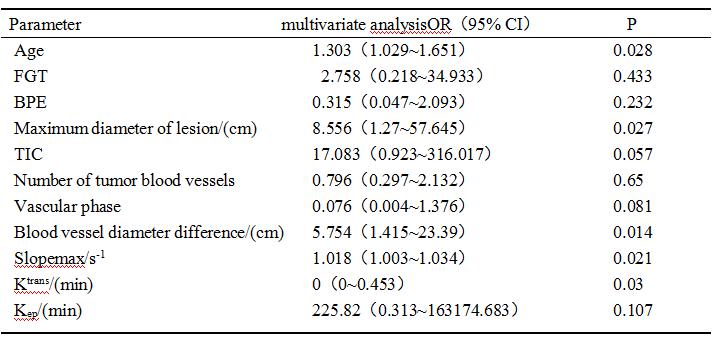
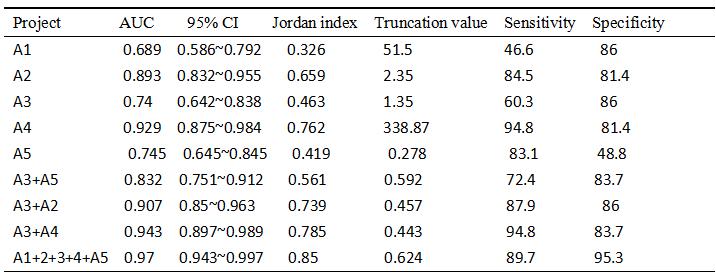
Excellent consistency was observed in parameter measurements between two observers (intraclass correlation coefficient, ICC > 0.9). Significant differences were identified between the two groups in terms of age, number of tumor vessels, difference in vessel diameter, vascular phase, Ktrans, Kep, Slopemax, TIC type, BPE, and FGT (P < 0.05), while SER and Ve did not exhibit statistically significant differences (P > 0.05). Refer to Table 1 for comprehensive details. Multivariate logistic regression analysis revealed that Ktrans, Slopemax, vascular diameter difference, age, and maximum lesion diameter were independent factors influencing differential diagnosis between the two groups. Slopemax exhibited the highest advantage ratio, with a corresponding AUC of 0.929, sensitivity of 94.8%, and specificity of 81.4%. See Table 2 for additional insights. When comparing the maximum lesion diameter, Slopemax, and Ktrans with the difference in vessel diameter using a combined model, the combined model of vascular diameter difference and Slopemax demonstrated the highest diagnostic efficacy (AUC 0.943), with sensitivity and specificity of 94.8% and 83.7%, respectively, surpassing the Slopemax model (AUC 0.929), with a statistically significant difference (P < 0.05). The AUC value of the combined model of vascular diameter difference and maximum lesion diameter was 0.907, while the AUC value of the vascular diameter difference and Ktrans combined model was 0.832, higher than the Ktrans model (AUC 0.745), though the differences in AUC between the combined models were not statistically significant (P > 0.05). Refer to Table 3 and Figure 2 for comprehensive details.Discussion and conclusion
In conclusion, this study highlights the value of combining DCE parameters with 3D-MIP parameters in improving the diagnostic accuracy of BI-RADS4 breast lesions.DCE-MRI can be used to evaluate angiogenesis and cell proliferation in BI-RADS4 breast cancer patients [3,4]. Key independent factors, including Ktrans, Slopemax, vascular diameter difference, age, and maximum lesion diameter, contribute to the differentiation of benign and malignant breast lesions within this category. Notably, the combination of vascular diameter difference and Slopemax exhibited the highest diagnostic efficiency, surpassing individual parameter models. These findings hold promise for enhancing early diagnosis and differential diagnosis of BI-RADS4 breast cancer.Furthermore, it is important to recognize the ongoing challenges in standardizing lesion classification, which still relies on the expertise of imaging specialists [6-8].Leveraging imageomics and multi-parameter joint imaging techniques could further unlock the potential and value of 3D-MIP vascular parameters in the early diagnosis and differentiation of BI-RADS4 breast cancer. These advances have the potential to significantly impact the field of breast cancer diagnosis and treatment, ultimately benefiting patients' outcomes and well-being.Acknowledgements
This study was supported by the Natural Science Foundation of Liaoning Province (2020-MS-266), 2022 Teaching Reform of Continuing Education of Liaoning Adult Education Society (LCYJGZXYB22100), University-level teaching reform research general project of Dalian Medical University (DYLX21036), and 2022 General Project of "Peak Climbing Plan" of Dalian city key specialty of medicine(2022DF042).References
[1] Çetinkaya E, Yıldız Ş, Otçu H, et al. The value of adjacent vessel sign in malignant breast tumors[J]. Diagn Interv Radiol, 2022,28(5):463-469. DOI:10.5152/dir.2022.211228.[2] Onishi N, Kataoka M, Kanao S, et al. Ultrafast dynamic contrast‐enhanced mri of the breast using compressed sensing: breast canSER diagnosis based on separate visualization of breast arteries and veins[J]. J Magn Reson Imaging, 2018,47(1):97-104. DOI:10.1002/jmri.25747.[3] Tsai WC, Chang KM, Kao KJ. Dynamic Contrast Enhanced MRI and Intravoxel Incoherent Motion to Identify Molecular Subtypes of Breast CanSER with Different Vascular Normalization Gene Expression[J]. Korean J Radiol,2021,22(7):1021-1033. DOI:10.3348/kjr.2020.0760.[4] Chang L, Lan H. Effect of Neoadjuvant Chemotherapy on Angiogenesis and Cell Proliferation of Breast CanSER Evaluated by Dynamic Enhanced Magnetic Resonance Imaging[J/OL]. Biomed Res Int,2022,2022:3156093 [2022-10-16]. https://pubmed.ncbi.nlm.nih.gov/35915805/. DOI:10.1155/2022/3156093[5] Ao F, Yan Y, Zhang ZL, et al. The value of dynamic contrast-enhanced magnetic resonance imaging combined with apparent diffusion coefficient in the differentiation of benign and malignant diseases of the breast[J]. Acta Radiol,2022,63(7):891-900. DOI:10.1177/02841851211024002.[6] Houkin K, Nakayama N, Kuroda S, et al. Novel magnetic resonance angiography stage grading for moyamoya disease[J]. SERebrovasc Dis, 2005, 20(5): 347-354. DOI:10.1159/000087935. [7] Hackenberg A, Battilana B, Hebeisen M, et al. Preoperative clinical symptomatology and stroke burden in pediatric moyamoya angiopathy: Defining associated risk variables[J]. Eur J Paediatr Neurol, 2021, 35: 130-136. DOI:10.1016/j.ejpn.2021.10.007. [8] Kamada C, Hirano T, Mikami T, et al. Additional Revascularization Using Multiple Burr Holes for PCA Involvement in Moyamoya Disease[J/OL]. J Stroke SERebrovasc Dis, 2021, 30(8) [2022-05-10]. https://doi.org/10.1016/j. jstrokeSERebrovasdis.2021.105852. DOI:10.1016/j.jstrokeSERebrovasdis. 2021.105852Figures