4574
Compensation of Respiratory Induced Artifacts in the Lumbar Spinal Cord Using a 1D Pre-Acquisition Navigator1Philips, Nashville, TN, United States, 2Vanderbilt University Institute of Imaging Science, Vanderbilt University Medical Center, Nashville, TN, United States, 3Radiology and Radiological Sciences, Vanderbilt University Medical Center, Nashville, TN, United States, 4Biomedical Engineering, Vanderbilt University, Nashville, TN, United States, 5Philips, Rochester, MN, United States, 6Radiology, Mayo Clinic, Rochester, MN, United States, 7Philips, Cleveland, OH, United States
Synopsis
Keywords: Artifacts, Spinal Cord, Respiration, multi-echo, GRE
Motivation: Respiration induces artifacts and signal loss in axial multi-echo gradient echo imaging of the lumbar spinal cord.
Goal(s): To investigate respiration-induced field shifts in the lumbar cord and to mitigate respiration induced artifacts using a 1D phase navigator.
Approach: A 1D phase navigator, added prior to the multi-echo gradient echo readout, was used to measure and provide compensation for respiration-induced and shot-dependent phase shifts.
Results: The proposed navigator was effective in measuring field shifts and providing a substantial reduction in artifacts in the lumbar spinal cord. Navigator post-processing was simplified compared to that required for a 1D navigator post-readout.
Impact: This work demonstrates, via phantom and in-vivo experiments, self-consistent measurements of respiration-induced field shifts and proposes an approach for their compensation that could be integrated into future spinal cord studies using multi-echo gradient echo acquisitions.
Introduction
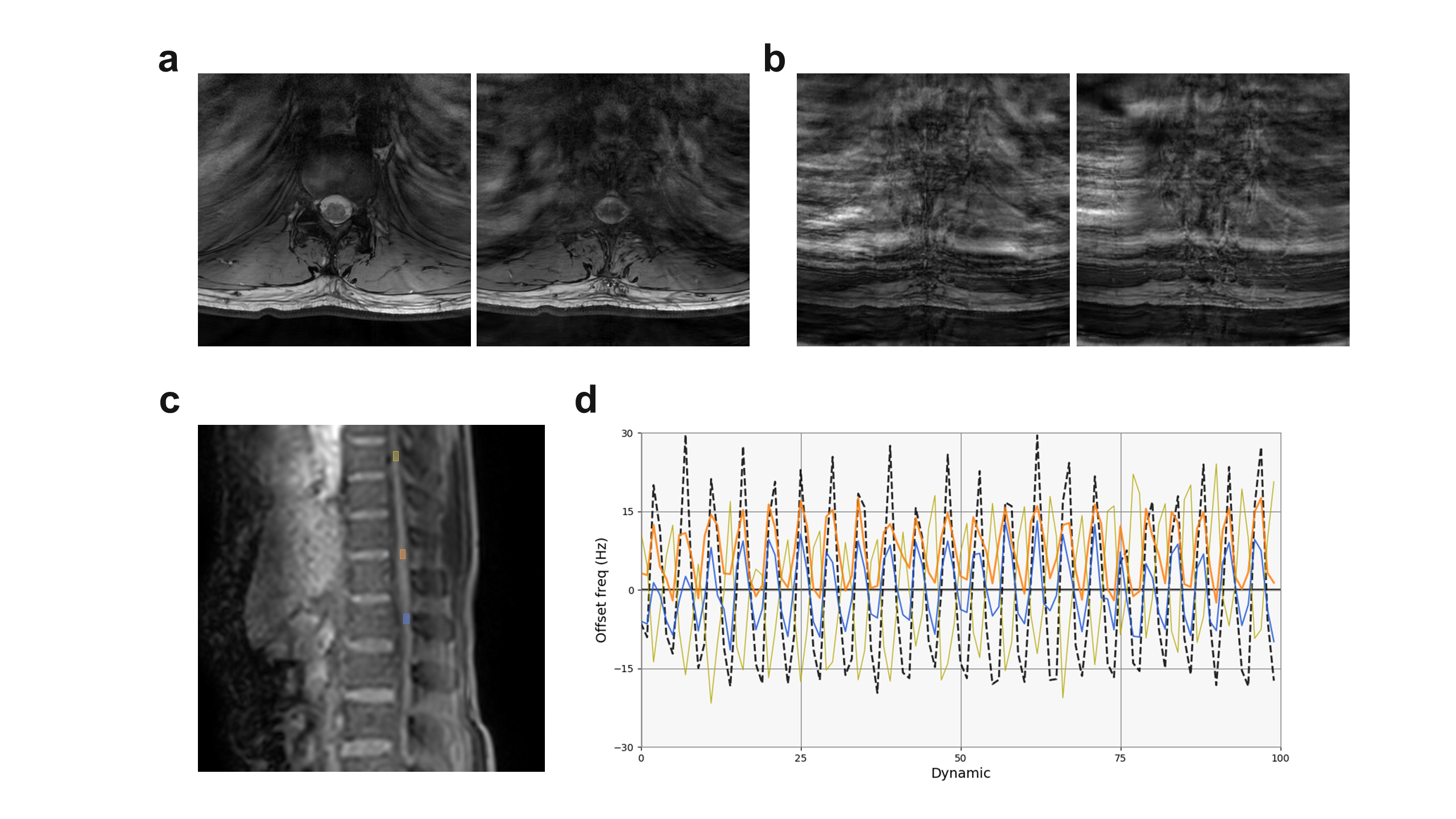
Axial multi-echo gradient echo (ME-GRE) of the spinal cord can provide high contrast between grey matter, white matter, and CSF. It has shown greater sensitivity in the detection of MS lesions1,2 and reduced CSF flow artifacts3 compared to T2 weighted TSE acquisitions. Challenges of ME-GRE in the spinal cord include relatively longer acquisition times compared to TSE and a greater prevalence of motion- and respiration-induced artifacts and signal loss. Respiration has been shown to induce field shifts as large as 74 Hz at 3T in the cervical cord4 with high spatial variability between slices. These field shifts cause shot-to-shot phase discrepancies, resulting in signal loss and motion-like ghosting artifacts that are subject and region dependent (see figure1a) and exacerbated in the thoracolumbar region, due to proximity to the lungs. A prior study investigated the use of a 1D phase navigator acquired after the ME-GRE echo train to measure and correct for respiration-induced field shifts5. Strong accumulation of phase at the navigator echo time necessitates advanced processing approaches such as spinal cord region selection and respiratory trace-guided phase unwrapping. This work proposes a similar 1D navigator echo placed prior to the ME-GRE echo-train. This simplifies the processing due to a much-reduced phase accumulation at the shorter TE of the phase navigator.Methods
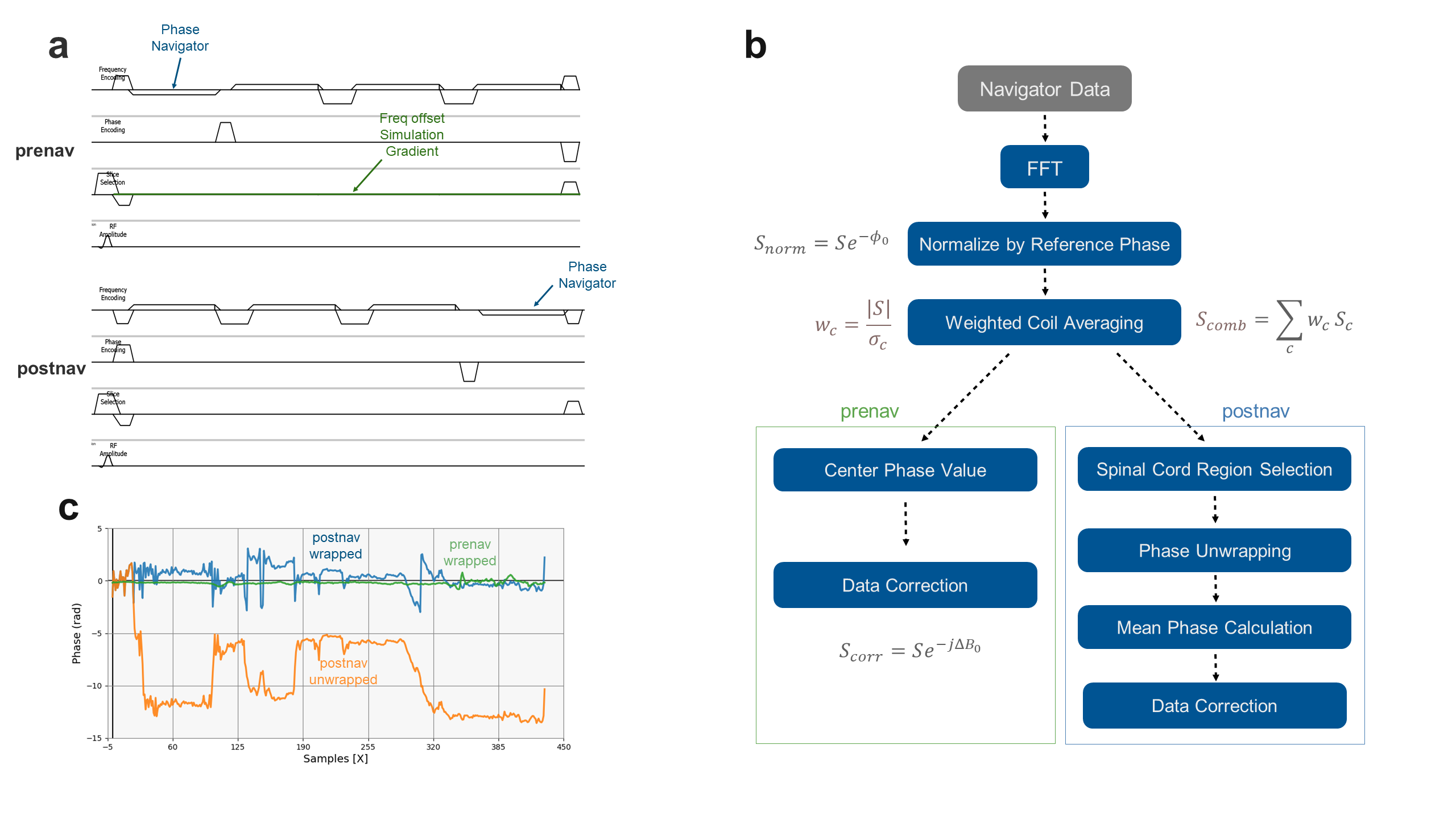
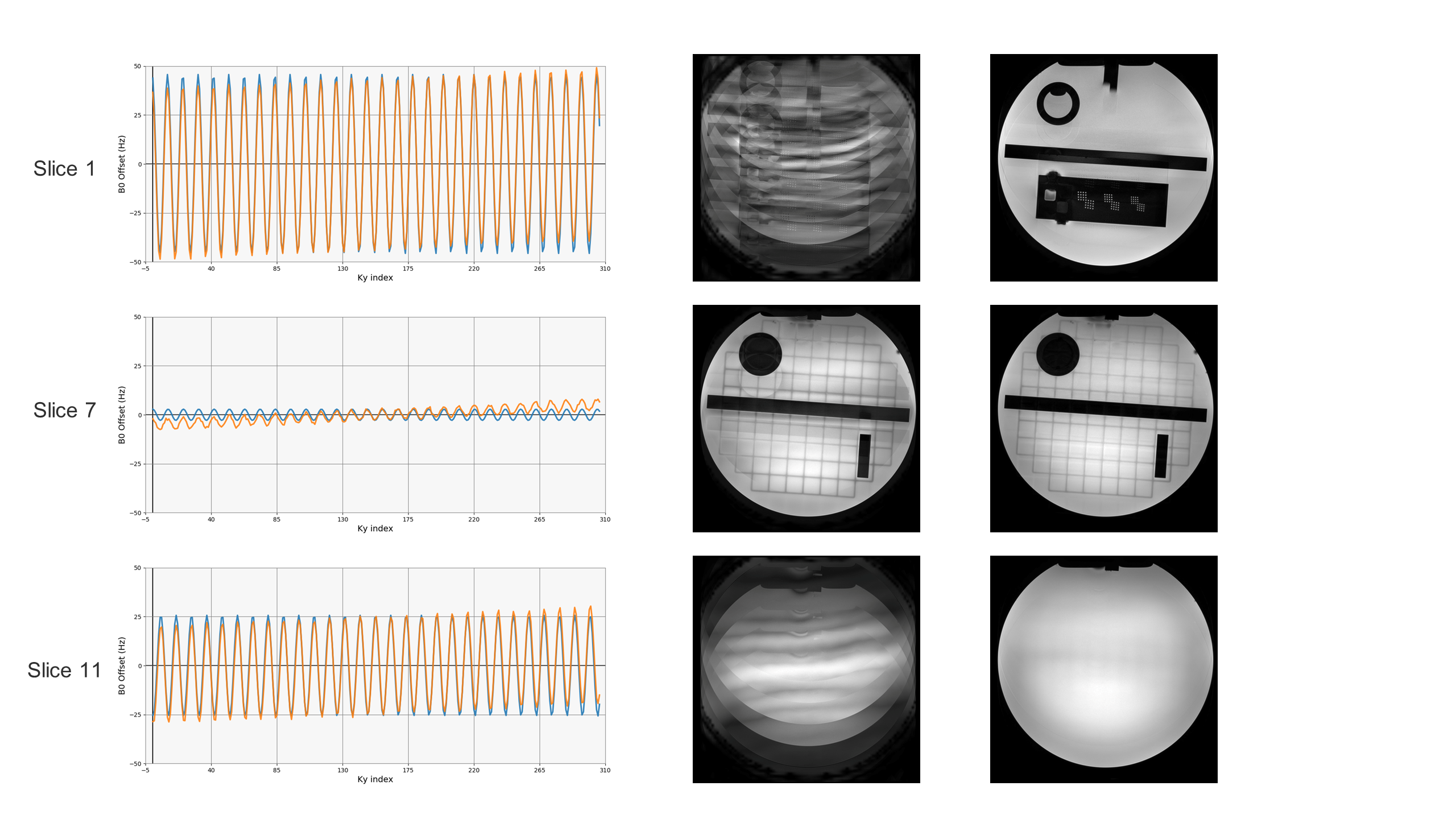
Both the proposed pre-acquisition navigator (prenav) and a comparable post-acquisition navigator (postnav) were implemented as options in the ME-GRE sequence using a modification of the vendor’s dynamic stabilization technique (see figure 2a). Profile dependent field shifts were estimated from the navigator data offline in GPI6 as illustrated in figure 2b. As shown in figure 2c, smaller phase accumulation (due to shorter TE) using prenav alleviated the need for phase unwrapping and careful region selection around the spinal cord. Estimated field shifts were imported and the correction applied in the vendor’s Recon 2.0 open reconstruction platform.A phantom experiment was designed to validate the prenav measurements and corrections. A very small amplitude Gz gradient was added just after the RF pulse and continued throughout the shot, causing a slice dependent frequency offset that was varied sinusoidally over shots with a maximum offset of 50 Hz at the furthest slice from isocenter. ME-GRE 3-echo prenav data were acquired (Philips 3.0T Achieva dStream, Best, Netherlands) in an American College of Radiology (ACR) large accreditation phantom.
Example in-vivo data were acquired in a healthy subject (Philips MR7700, Best, Netherlands) under guidance of the institutional review board and following informed consent. The range and behavior of respiratory induced field shifts were measured using a dynamic, rapid, single-slice, sagittal multi-acquisition Dixon GRE scan with ΔTE=1ms. The change in f0 with respiration was evaluated using the resulting dynamic Dixon B0 maps. ME-GRE (3-echo) data were acquired either with prenav enabled or postnav enabled in the lumbar cord during free breathing. The echo-times were minimized, leading to longer echo times for the prenav sequence.
Results
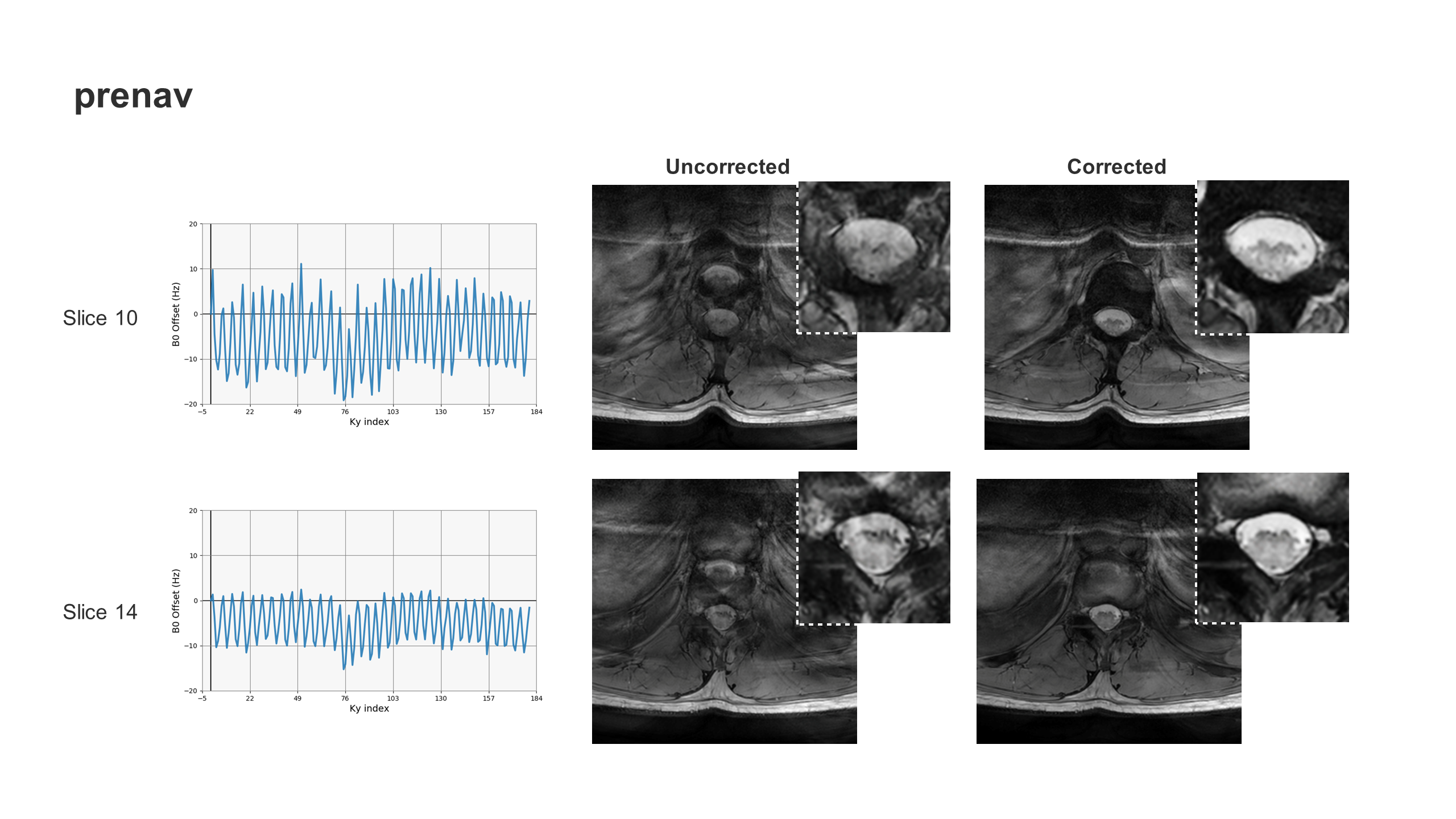
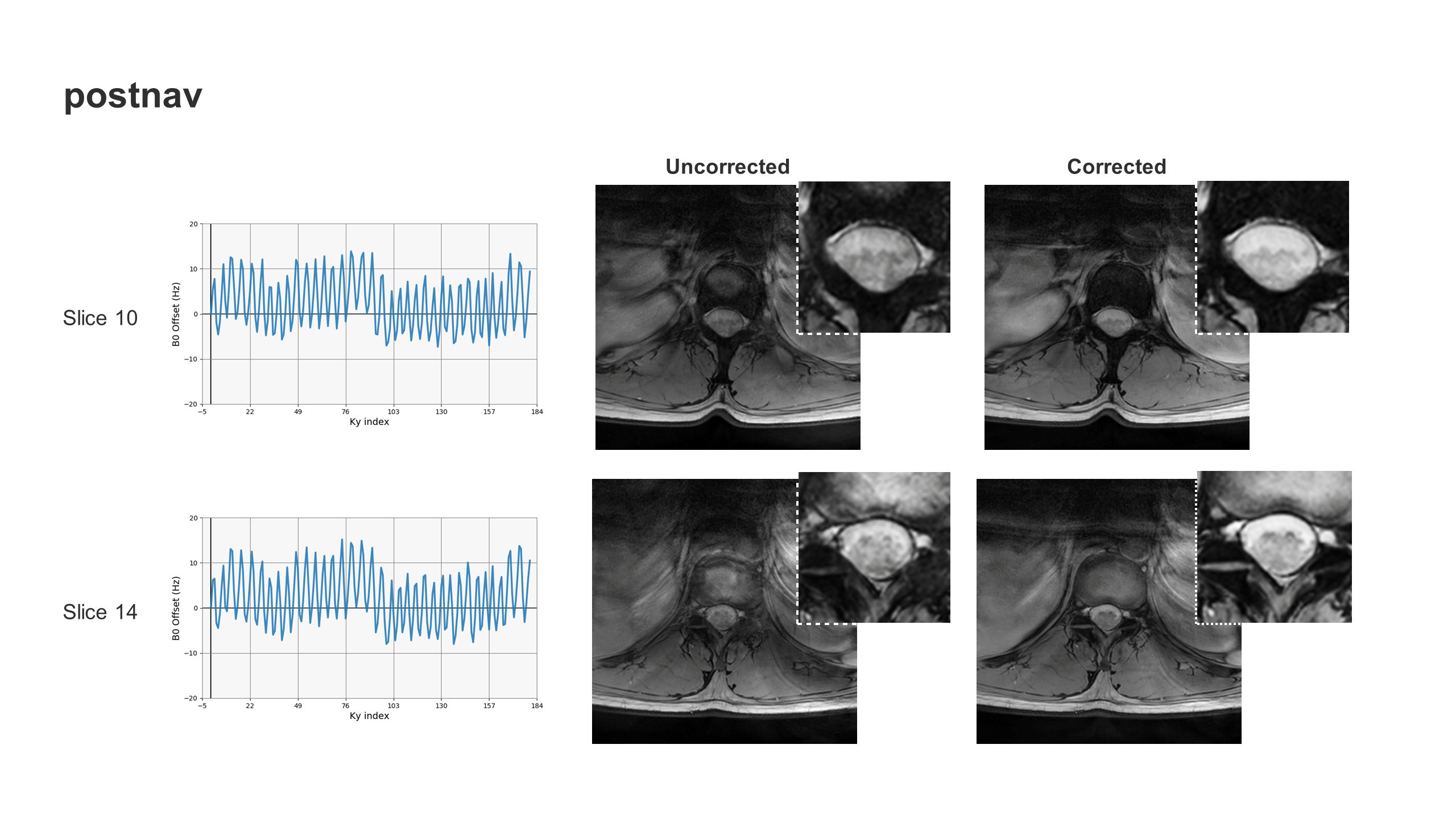
The time dependence of Δf0 at 3 different spine levels is shown in figure 1d. Variations of up to 30 Hz were observed to align with the trace from the respiratory bellows. The measured frequency offsets in the ACR phantom scan (figure 3) were consistent with the expected induced offsets and increased with slice distance from the isocenter. The resulting image artifacts were largely mitigated using the measured Δf0 values from the prenav method. Figures 4 and 5 show the measured Δf0 values in the lumbar cord of a healthy volunteer using the prenav and postnav techniques, respectively. Signal loss and artifacts in the cord were largely reduced using the proposed correction. Smaller artifacts were observed in the postnav acquisition, but noticeable improvements in image quality within the cord were observed using the correction.Discussion and Conclusion
The proposed prenav approach simplifies data processing of the navigator data, which may improve robustness. The disadvantage of the prenav approach is longer minimum TEs, but this is not a major limitation for most T2*-weighted ME-GRE acquisitions. The stronger artifacts observed in the prenav data are likely due to longer TEs compared to postnav. However, the corrected data are of high quality and, subjectively, are not worse in the spinal canal than the postnav acquisition data. Variations in Δf0 as measured by the dynamic Dixon B0 measurement were larger in regions closer to the lungs. Both this trend and the scale of the field shifts are consistent with the measured frequency values using the prenav and postnav approaches. This study provides encouraging and illustrative examples. A full comparison between the prenav and postnav approaches will require a larger sample size.Acknowledgements
The authors would like to thank Melvyn Ooi for productive conversations related to the content of this work.References
1. White M, Zhang Y, Healey K. Cervical spinal cord multiple sclerosis: evaluation with 2D multi-echo recombined gradient echo MR imaging. J Spinal Cord Med 2011; 34: 93-8.
2. Martin M, Malfair D, Zhao Y, et al. Comparison of MERGE and axial T2-weighted fast spin-echo sequences for detection of multiple sclerosis lesions in the cervical spinal cord. AJR 2012; 199: 157-62.
3. Katz HB, Quencer RM, Hinks RS. Comparison of gradient-recalled-echo and T2-weighted spin-echo pulse sequences in intramedullary spinal lesions. AJNR 1989; 10: 815-22.
4. Verma T, Cohen-Adad J. Effect of respiration on the B0 field in the human spinal cord at 3T. Magn Reson Med 2014; 72: 1629-1636.
5. Beghini L, David G, Liechti MD, et al. Optimised navigator correction of physiological field fluctuations in multi-echo GRE of the lumbar spinal cord at 3T. In Proceedings of the 2023 ISMRM & ISMRT Annual Meeting & Exhibition, Toronto, 2023. p. 3413.
6. Zwart NR, Pipe JG. Graphical programming interface: a development environment for MRI methods. Magn Reson Med 2015; 74: 1449–1460.
Figures