4573
Translating 3D stack-of-spirals lung water MRI from 0.55T to 1.5T1National Heart, Lung, and Blood Institute, National Institutes of Health, Bethesda, MD, United States, 2Department of Molecular Medicine and Surgery, Karolinska Institutet, Stockholm, Sweden, 3Department of Clinical Physiology, Karolinska University Hospital, Stockholm, Sweden, 4Division of Cardiology, MedStar Washington Hospital Center, Washington, DC, United States
Synopsis
Keywords: Data Acquisition, Translational Studies, Lung water, Heart Failure
Motivation: Our recently developed 0.55T MRI sequence to measure lung water dynamics has clinical utility in the evaluation of heart failure, but cardiac MRI is more widely performed at 1.5T.
Goal(s): To translate a 3D stack-of-spirals lung water MRI sequence from 0.55T to 1.5T.
Approach: We optimized sequence parameters through Bloch equation simulation, phantom experiments, and in vivo imaging in 10 healthy volunteers, acquired at two different centers.
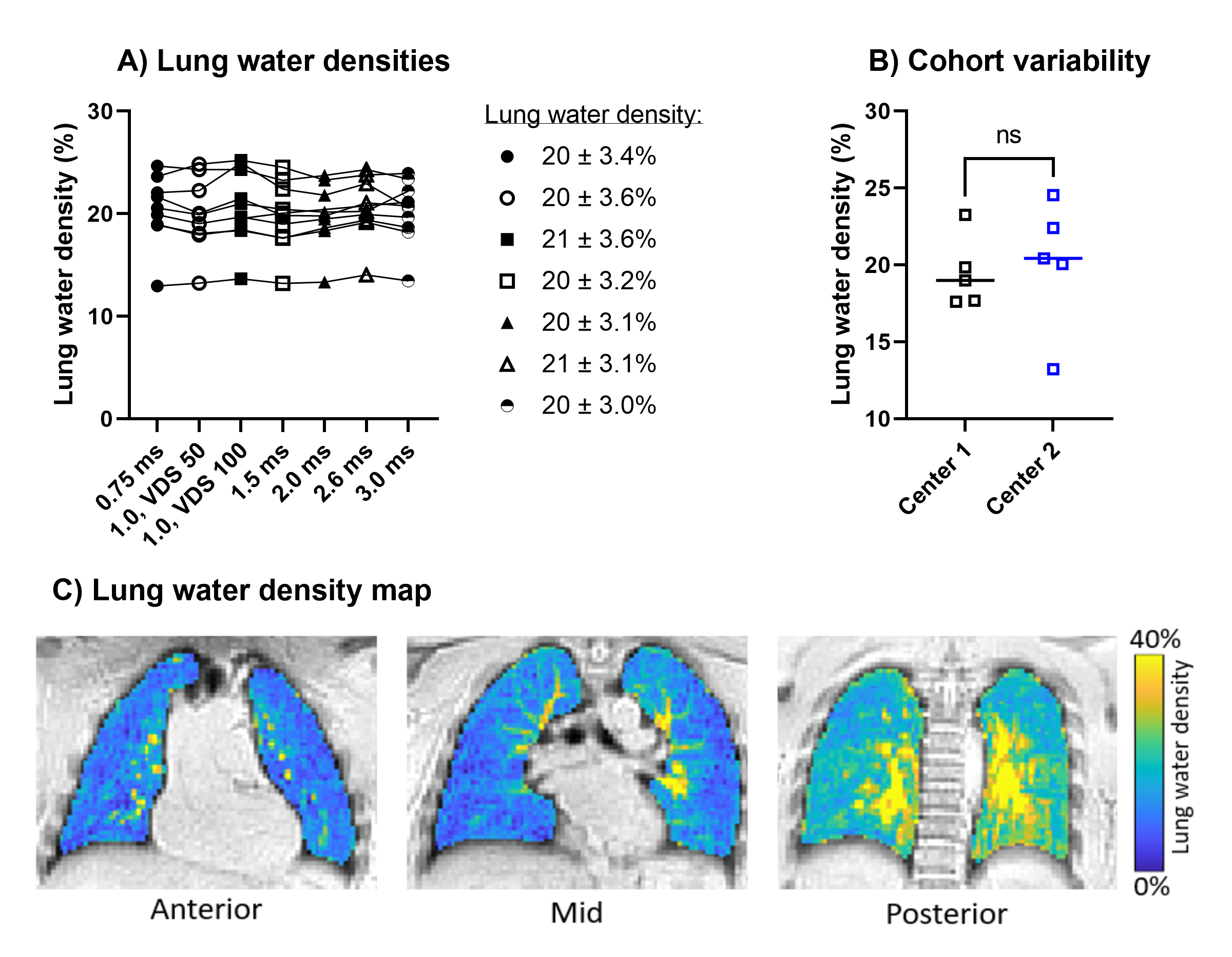
Results: The sequence parameters TE/TR/FA/readout duration=0.70ms/9.0ms/1°/1.5ms at 1.5T yielded proton density weighted images with apparent SNR 13.5±2.2, limited image blur, and quantified a lung water density 20±3.2%.
Impact: Lung water quantification has emerged as a promising method to monitor and predict outcomes in heart failure. Translation of a lung water MRI sequence from 0.55T to 1.5T enables a more widespread adoption of this tool.
Introduction
Lung water is a key feature in patients with heart failure, and MRI methods to quantify lung water have recently emerged at different field strengths1–5. We recently developed a 0.55T free-breathing respiratory-navigated 3D lung water imaging method which we used for dynamic lung water imaging during exercise stress5,6, a capability which is of clinical interest as exercise-induced lung water is an early symptom of heart failure. To enable more widespread adoption of this dynamic lung water imaging method, we sought to translate and optimize our sequence to the more conventional and widely used 1.5T field strength.Methods
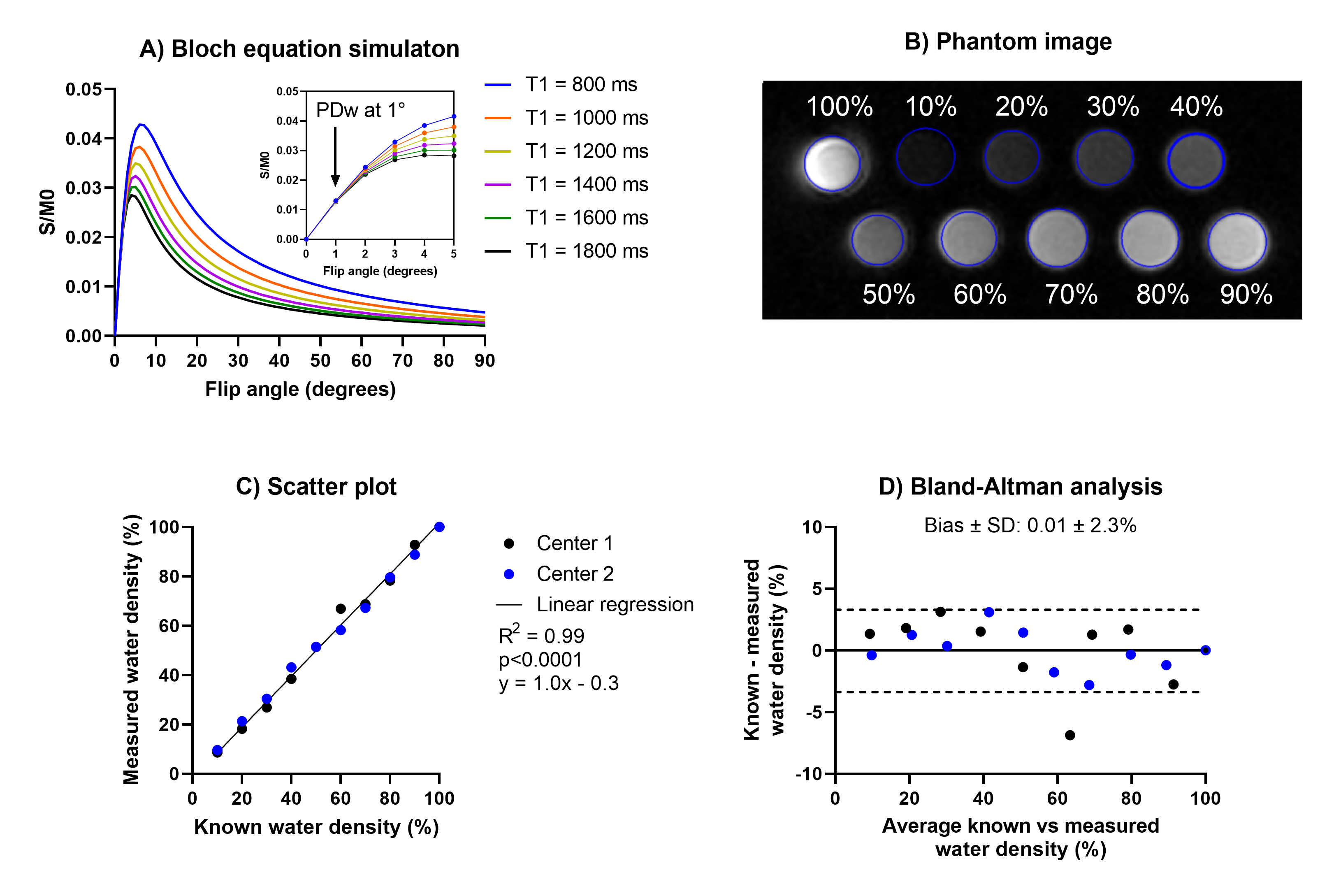
A custom 3D stack-of-spirals self-gated proton density weighted gradient echo sequence with a respiratory binned image reconstruction with gradient impulse response function (GIRF) correction which has previously been validated for 0.55T6–8 was deployed on a 1.5T scanners (MAGNETOM Sola, Siemens) at two centers. The sequence translation to 1.5T was performed in the following steps:1) We evaluated the sequence proton density weighting for TE/TR/T2*=0.7ms/5.0ms/2.64ms and flip angle range 0-90° by Bloch equation simulation with T1 values of 800-1800 ms, and by imaging an array of vials containing known concentrations of water and deuterium oxide at both centers. Proton density weighting is important for quantification purposes.
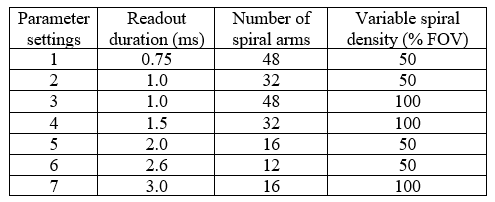
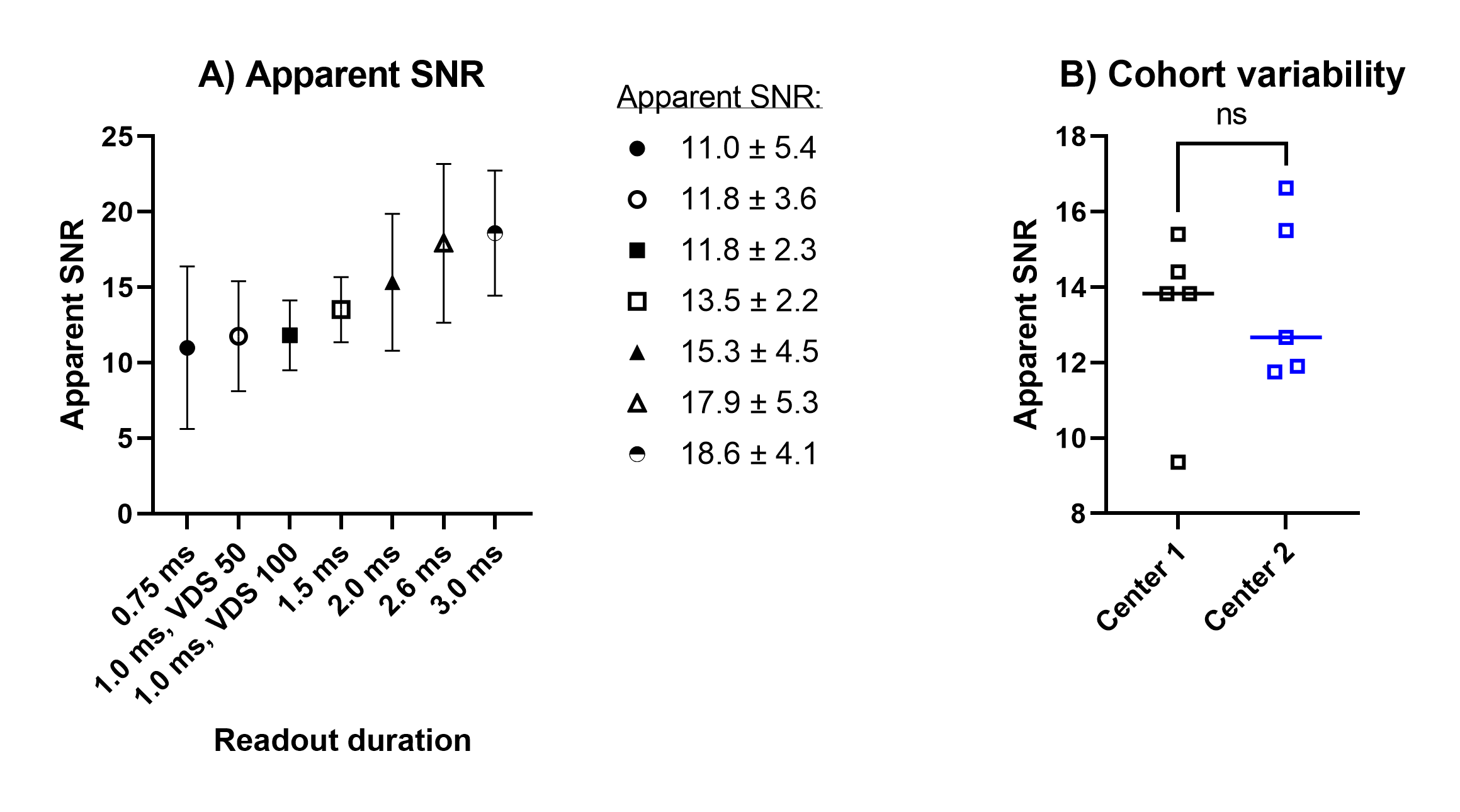
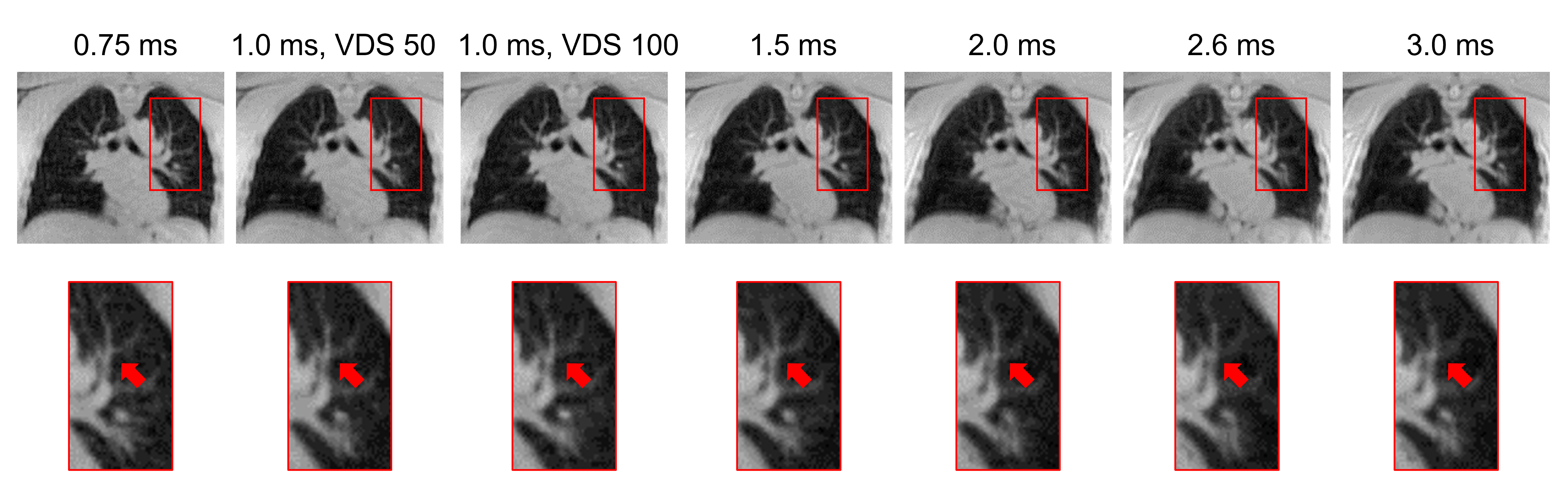
2) We imaged 10 healthy volunteers, 5 at each center, for spiral parameter optimization. We assessed the trade-off between signal-to-noise ratio (SNR) and off resonance artifacts for 7 spiral readout durations, achieved by changing the variable spiral density9 and number of spiral arms (Table 1). We calculated apparent SNR as the ratio of the mean lung parenchymal signal intensity to the standard deviation of the background signal in a central slice. Image blur and occurrence of under sampling spiral artifacts were qualitatively assessed.
3) Lung water density was quantified using an automated image processing pipeline with a neural network based lung segmentation7, and related to previously published values.
Results
Block equation simulation disclosed a signal change of 2.9% across the range of T1-values. These parameters were fixed for all subsequent imaging in this study (Figure 1A). The phantom experiment confirmed that the sequence is proton density weighted at 1.5T, with excellent correlation (R2=0.99, p<0.0001) and low bias (0.01 ± 2.3%) between known and measured water densities (Figure 1B-D).Imaging was successful in all healthy subjects (mean age 37 years, range 29-54 years, 3 male). As expected, apparent SNR increased with longer readout durations (Figure 2), and so did the observed image blur in the lungs caused by off-resonance (Figure 3). We concluded that a 1.5 ms readout is suitable in the trade-off between apparent SNR (13.5±2.2) and blurring artifacts. Global lung water densities were similar across readout durations (Figure 4), and measured 20±3.2% for readout 1.5 ms, which is in line with previously reported 1.5T values 17±2.1% by Thompson et al1 and with our measurements at 0.55T (23.1±4.0%)8. Results between both centers were comparable, with no differences in apparent SNR or lung water density.
Discussion
In this study, we translate an MRI sequence for measuring lung water from 0.55T to 1.5T, and optimize sequence parameters to ensure proton density weighting, sufficient apparent SNR, limited off resonance blurring, and confirmed the quantitative capabilities of the sequence in a phantom and in 10 healthy subjects imaged at rest, acquired at two different centers. The measured lung water densities were in parity with previously reported values from 1.5T. Further studies are warranted to test the 1.5T method on healthy subjects and patients with heart failure, both at rest and during exercise stress.Conclusion
Our 0.55T self-gated 3D stack-of-spiral lung water imaging method was successfully deployed and optimized for 1.5T at two centers, thus enabling a more widespread availability of this tool.Acknowledgements
This study was supported by the 2023 Society for Cardiovascular Magnetic Resonance Seed Grant and NHLBI DIR (Z01-HL006257, Z01-HL006213).References
1. Thompson RB, Chow K, Pagano JJ, Sekowski V, Michelakis ED, Tymchak W, et al. Quantification of lung water in heart failure using cardiovascular magnetic resonance imaging. J Cardiovasc Magn Reson 2019;21:58. doi:10.1186/s12968-019-0567-y.
2. Rocha BML, Cunha GJL, Freitas P, Lopes PMD, Santos AC, Guerreiro S, et al. Measuring lung water adds prognostic value in heart failure patients undergoing cardiac magnetic resonance. Sci Rep 2021;11:20162. doi:10.1038/s41598-021-99816-6.
3. Burrage MK, Hundertmark M, Valkovič L, Watson WD, Rayner J, Sabharwal N, et al. Energetic Basis for Exercise-Induced Pulmonary Congestion in Heart Failure With Preserved Ejection Fraction. Circulation 2021;144:1664–1678. doi:10.1161/CIRCULATIONAHA.121.054858.
4. Meadus WQ, Stobbe RW, Grenier JG, Beaulieu C, Thompson RB. Quantification of lung water density with UTE Yarnball MRI. Magn Reson Med 2021;86:1330–1344. doi:10.1002/mrm.28800.
5. Seemann F, Javed A, Khan J, Bruce C, Chae R, Yildirim K, et al. Dynamic lung water magnetic resonance imaging during exercise stress. Magn Reason Med 2023:1–18. doi:10.1002/mrm.29716.
6. Javed A, Ramasawmy R, O’Brien K, Mancini C, Su P, Majeed W, et al. Self-gated 3D stack-of-spirals UTE pulmonary imaging at 0.55T. Magn Reson Med 2022;87:1784–1798. doi:10.1002/mrm.29079.
7. Seemann F, Javed A, Chae R, Ramasawmy R, O’Brien K, Baute S, et al. Imaging gravity-induced lung water redistribution with automated inline processing at 0.55 T cardiovascular magnetic resonance. J Cardiovasc Magn Reson 2022;24:35. doi:10.1186/s12968-022-00862-4.
8. Seemann F, Javed A, Ramasawmy R, Wang H, Baute S, Campbell-Washburn AE. Free-breathing 3D lung water MRI is ready for commercial 0.55T MRI systems. Proc. Soc. Cardiovasc. Magn. Reson., 2024.
9. Tsai C-M, Nishimura DG. Reduced aliasing artifacts using variable-densityk-space sampling trajectories. Magn Reson Med 2000;43:452–458. doi:10.1002/(SICI)1522-2594(200003)43:3<452::AID-MRM18>3.0.CO;2-B.
Figures