4569
Identification of cardiac phase in hyperpolarized 13C cardiac MRI using multiphase 1H MRI and unitized 3D patch-based reconstruction1Advanced Imaging Research Center, UT Southwestern Medical Center, Dallas, TX, United States, 2Department of Biomedical Engineering, UT Southwestern Medical Center, Dallas, TX, United States, 3Department of Radiology, UT Southwestern Medical Center, Dallas, TX, United States
Synopsis
Keywords: Image Reconstruction, Hyperpolarized MR (Non-Gas), Cardiac phase detection
Motivation: The predetermined trigger delay may fail to acquire 13C images at an unstable heart rate and cause a misalignment between the cardiac phases depicted in structural and metabolic images.
Goal(s): Aim to exploit the volumetric PBSR algorithm to establish an automated alignment workflow to identify the actual cardiac phase for HP 13C images.
Approach: Image pairs of multiple 1H cardiac phases and single-phase 13C images will be reconstructed by 3D PBSR, and the pair with the best similarity/in-focus index will be elected.
Results: The digital phantom and an in-vivo HP 13C cardiac image demonstrated the feasibility of cardiac phase detection.
Impact: The currently proposed automated alignment workflow identifies the actual cardiac phase when the HP 13C images are acquired, and this technique will potentially benefit patients with arrhythmia or pediatric populations.
INTRODUCTION
Carbon-13 (13C) MRI with hyperpolarized (HP) [1-13C]pyruvate captures key processes of pyruvate metabolism of the heart (1, 2). By far, most human studies have been targeting to image cardiac metabolism at the end of diastole for smaller myocardial motion (3-6). For this, a trigger delay is calculated from 1H cardiac cine, assuming that the cardiac rate remains consistent during HP imaging. However, the predetermined trigger delay may fail to acquire 13C images at the aimed cardiac time frame, particularly in individuals with unstable heart rate (e.g., arrhythmia) or anxiety, risking a misalignment between the cardiac phases depicted in structural and metabolic images (7). Moreover, metabolic profiles of the heart, seen by HP [1-13C]pyruvate, are substantially affected by the cardiac cycle, in which the data are acquired (8). Previously, we developed a volumetric patch-based super-resolution (PBSR) reconstruction algorithm to enhance the spatial resolutions of HP 13C images by exploiting high-resolution compartmental information collected from 1H patches. In this study, we aim to exploit the volumetric PBSR algorithm and multiphase 1H cardiac MRI to establish an automated alignment workflow that identifies the actual cardiac phase when the HP 13C images are acquired. The underlying hypothesis is that the performance of the algorithm is optimal when 13C and 1H images are from the same cardiac phase.METHODS
Digital phantom simulation:A series of cross-sectional view cardiac digital phantoms (9) were created to simulate multiphase cardiac 1H MRI (eight cardiac phases), assuming that the 6th phase was targeted for 13C imaging (Figure 1). These multiple phases allow the myocardium volume change by +50% to -15% from the baseline (6th phase). The ground truth 13C images were also generated and aligned with the 6th phase. The volumetric PBSR reconstruction algorithm was applied to the 13C images using a predetermined optimal patch size (9). To estimate the cardiac phase, fourteen shape-from-focus operators (10) were applied to reconstructed multi-slice 13C images and evaluated (11 slices x 14 operators x 8 phases)(10). For each slice, the phase with the best similarity/in-focus index was recorded, and the most probably cardiac phase was singled out based on the votes.
In vivo cardiac imaging validation:
A set of cardiac images was acquired from a healthy volunteer (26-year-old, male) from a clinical 3T MRI scanner (GE Healthcare, Waukesha, WI, USA). Multiphase cardiac 1H MRI was acquired using the body coil (#slice = 3, #phase = 15, TE/TR/IR=1.364/3.504/250ms, voxel size=0.78´078´10 mm3). HP [1-13C]pyruvate was polarized using a 5T SPINlab DNP polarizer (GE Healthcare) and 250-mM HP [1-13C]pyruvate solution was injected as a bolus (injection rate = 5 mL/s) as previously described (3-6). Immediately after the HP injection, time-resolved [1-13C]pyruvate images were acquired from a single slice (short-axis view) every 840 ms using a multi-echo spiral imaging sequence (single shot, flip angle=5°, voxel size=10´10´30mm3). Lactate and bicarbonate images were not acquired. The ECG was recorded. A two-loop 13C Helmholtz coil was used (PulseTeq Limited, Chobham, Surrey, UK).
RESULTS and DISCUSSION
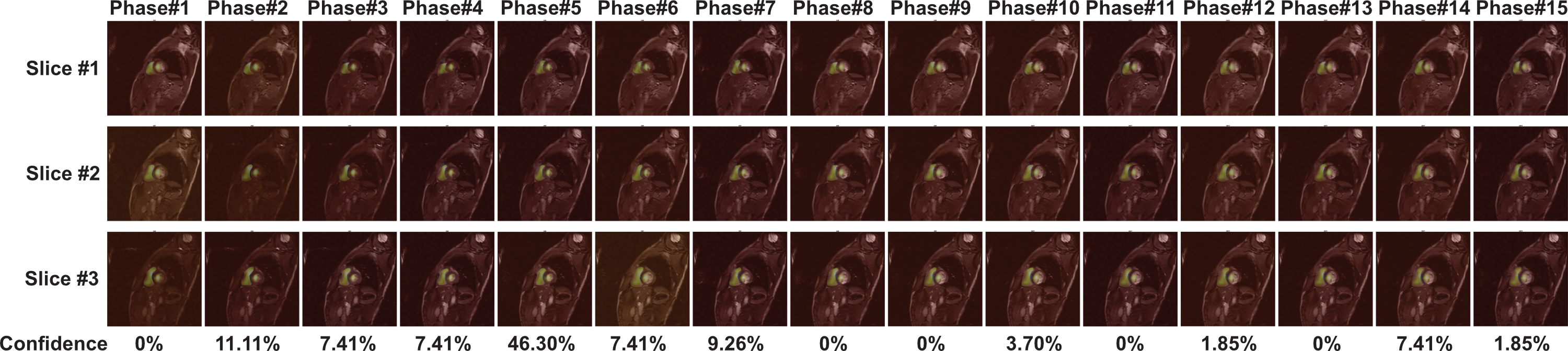
All three simulated metabolites robustly detected the correct cardiac phase and showed consistent patterns. The reconstructed images exhibited a blurring effect along the inner and outer edges of the myocardium as the volume of phase misalignment grew. [13C]Bicarbonate signals were more sensitive to phase misalignment (approximately 5% volume changes in phases 5 and 7) (Figure 2) than [1-13C]lactate (Figure 3) and [1-13C]pyruvate (Figure 4). This is likely attributed to its higher entropy (3.4807) compared to the other signals (2.7105 and 2.9746 in [1-13C]pyruvate and [1-13C]lactate, respectively). For instance, halo-like artifacts appeared when the volumetric difference exceeded 30% in phase 3. In the voting results to detect the cardiac phase, all three metabolites successfully identified phase 6 with 62.57%, 44.92%, and 49.73% of confidence for [13C]bicarbonate, [1-13C]lactate, and [1-13C]pyruvate, respectively. For the in vivo HP 13C cardiac image validation, the proposed workflow identified the accurate cardiac phase from the corresponding 1H CINE images with 46.30% confidence (Figure 5). The in vivo data suggests that the integrated voting pipeline and shape-from-focus metrics can automate the phase identification process retrospectively. This is expected to allow trigger-free cardiac metabolic imaging, improving both temporal and spatial resolutions of dynamic HP 13C cardiac imaging. This technique will benefit patients with arrhythmia or pediatric populations.CONCLUSION
We introduced multiphase 1H MRI and unitized 3D patch-based reconstruction as a tool for retrospective determination of cardiac HP 13C images, and demonstrated the performance in simulation and in a human subject. We plan to validate the performance further with additional human participants.Acknowledgements
This study was supported by the National Institutes of Health of the United States (R01 NS107409, P41 EB015908, S10 OD018468); U.S. Army Medical Research Acquisition Activity (W81XWH2210485); Muscular Dystrophy Association (MDA963281).
References
1. Golman K, Petersson JS, Magnusson P, Johansson E, Akeson P, Chai CM, et al. Cardiac metabolism measured noninvasively by hyperpolarized 13C MRI. Magn Reson Med. 2008;59(5):1005-13.
2. Schroeder MA, Cochlin LE, Heather LC, Clarke K, Radda GK, Tyler DJ. In vivo assessment of pyruvate dehydrogenase flux in the heart using hyperpolarized carbon-13 magnetic resonance. Proc Natl Acad Sci U S A. 2008;105(33):12051-6.
3. Cunningham CH, Lau JY, Chen AP, Geraghty BJ, Perks WJ, Roifman I, et al. Hyperpolarized 13C Metabolic MRI of the Human Heart: Initial Experience. Circ Res. 2016;119(11):1177-82.
4. Park JM, Reed GD, Liticker J, Putnam WC, Chandra A, Yaros K, et al. Effect of Doxorubicin on Myocardial Bicarbonate Production From Pyruvate Dehydrogenase in Women With Breast Cancer. Circ Res. 2020;127(12):1568-70.
5. Ma J, Chen J, Reed GD, Hackett EP, Harrison CE, Ratnakar J, et al. Cardiac T2 * measurement of hyperpolarized (13) C metabolites using metabolite-selective multi-echo spiral imaging. Magn Reson Med. 2021;86(3):1494-504.
6. Reed GD, Ma J, Park JM, Schulte RF, Harrison CE, Chen AP, et al. Characterization and compensation of inhomogeneity artifact in spiral hyperpolarized 13 C imaging of the human heart. Magnetic Resonance in Medicine. 2021;86(1):157-66.
7. Ferreira PF, Gatehouse PD, Mohiaddin RH, Firmin DN. Cardiovascular magnetic resonance artefacts. J Cardiovasc Magn Reson. 2013;15(1):41.
8. Ma J, Malloy CR, Pena S, Harrison CE, Ratnakar J, Zaha VG, Park JM. Dual-phase imaging of cardiac metabolism using hyperpolarized pyruvate. Magn Reson Med. 2022;87(1):302-11.
9. Sung-Han Lin JJM, Jae Mo Park, editor Volumetric patch-based image reconstruction for enhancing hyperpolarized 13C MRI with hybrid image guidance. ISMRM Annal Meeting; 2022 07-12 May 2022; London, UK.
10. Pertuz S, Puig D, Garcia MA. Analysis of focus measure operators for shape-from-focus. Pattern Recogn. 2013;46(5):1415-32.
Figures
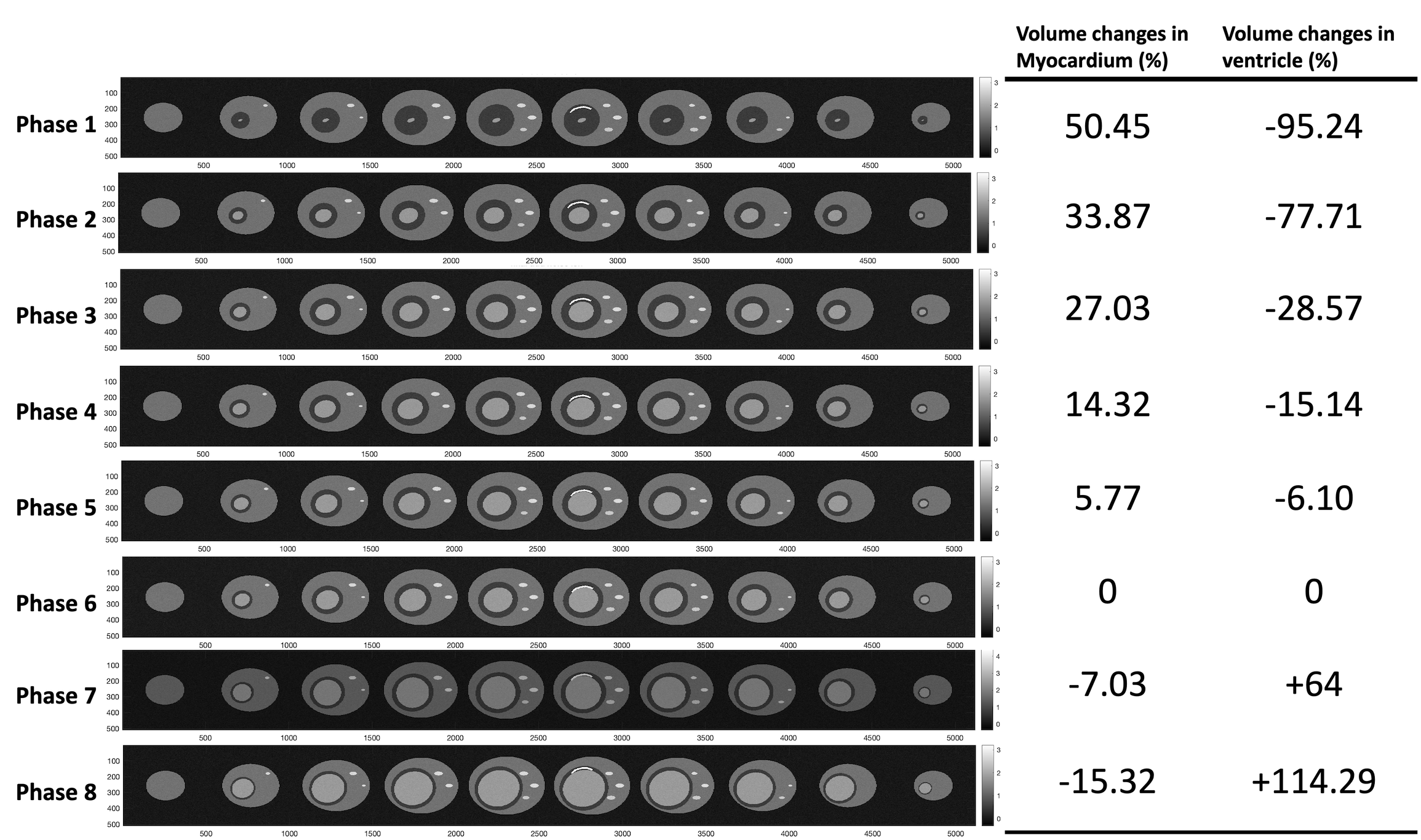
Figure 1. Multiple phase digital phantom setup. Eight distinct phases for the 1H images were simulated with up to 50.54% volume increase in myocardium and 95.24% decrease in ventricle at end-systole, compared to the baseline (phase 6). The simulated volume is set to decrease by 15.32% in myocardium and increase by 114.29% in ventricle end-diastole, compared to the baseline.

Figure 2. Reconstruction of [13C]bicarbonate phantom. The single phase [13C]bicarbonate image was paired with 8 multi-phase 1H images, and reconstructed signals exhibited a blurring effect along the inner and outer edges of the myocardium during the phase misaligned.
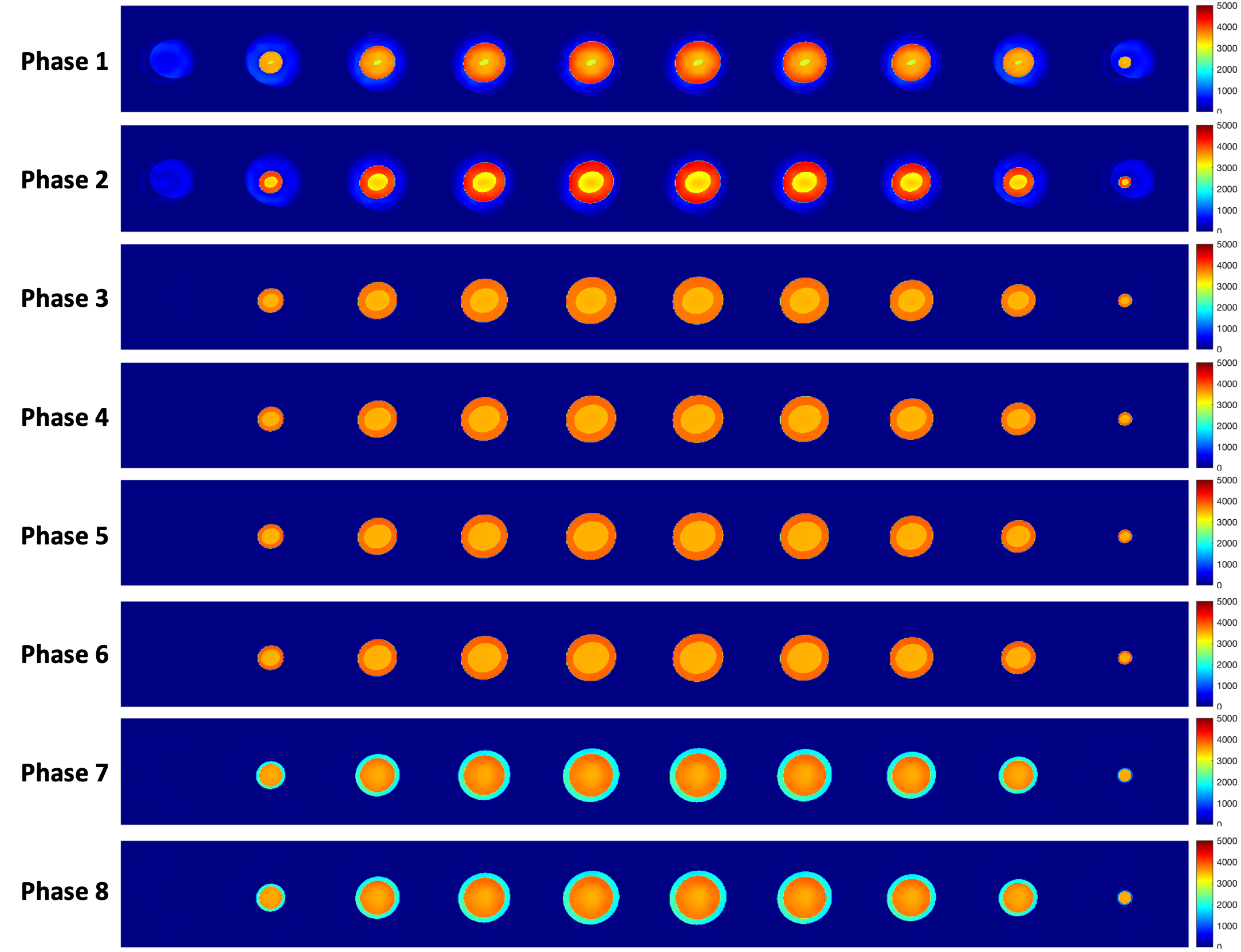
Figure 3. Reconstruction of [1-13C]lactate phantom. The single phase [1-13C]lactate image was paired with 8 multi-phase 1H images, and reconstructed signals exhibited a blurring effect along the inner and outer edges of the myocardium while the phase misaligned caused more than 30% myocardium increase, compared to the ground truth.
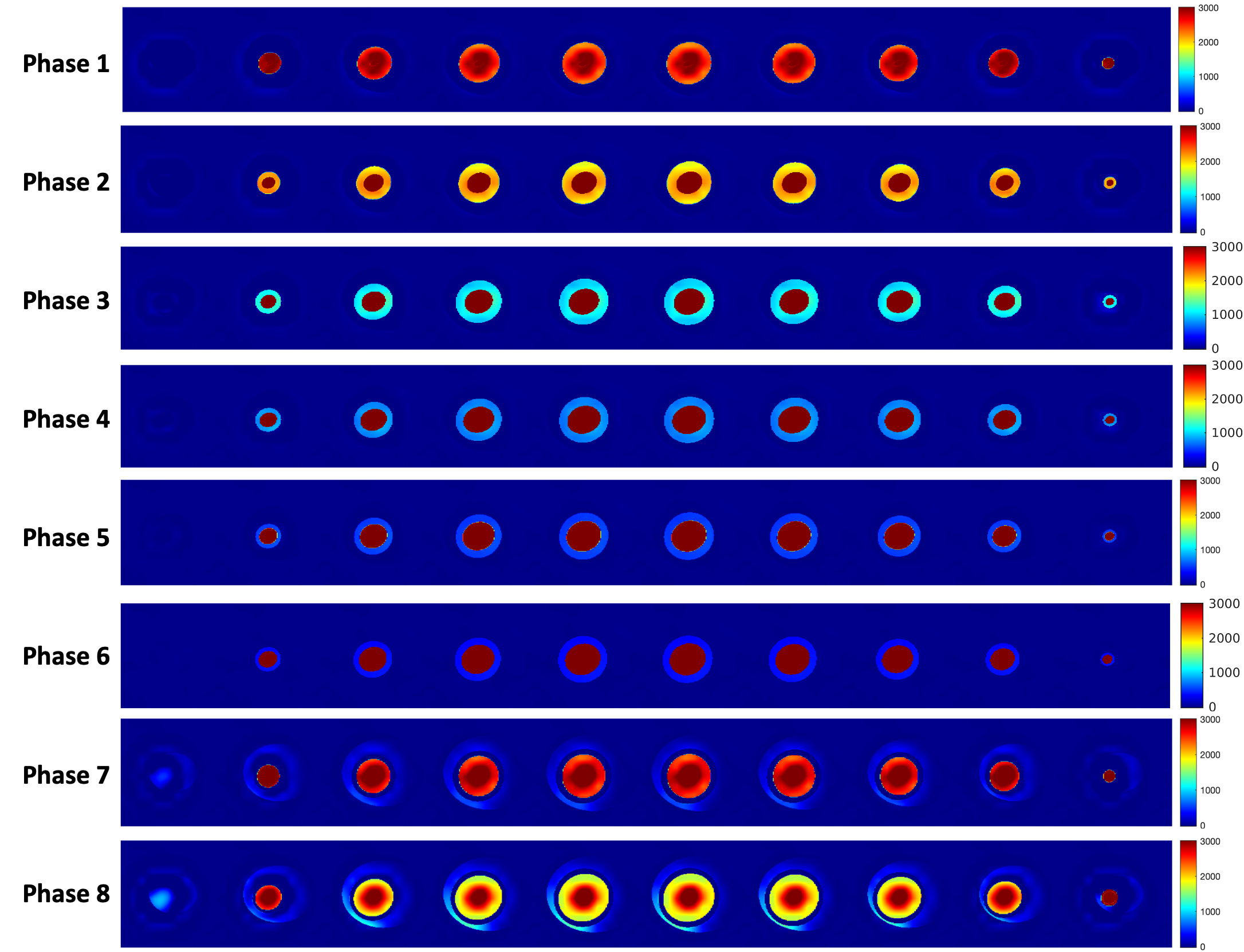
Figure 4. Reconstruction of [1-13C]pyruvate phantom. The single phase [1-13C]pyruvate image was paired with 8 multi-phase 1H images, and reconstructed signals exhibited a blurring effect around the myocardium while the phase was misaligned.