4566
Measurement of 3D abdominal magnetic transfer ratio under a single breath-hold using 3D segmented EPI: a preliminary study1MR Research Collaboration Team, Siemens Healthineers Ltd., Shanghai, China, 2Siemens Healthcare Pty Ltd., Brisbane, Australia, 3Department of Radiology, Fudan University, Shanghai, China, 4Application Developments, Siemens Shenzhen Magnetic Resonance Ltd., Shenzhen, China
Synopsis
Keywords: Quantitative Imaging, Body
Motivation: Three-dimensional magnetic transfer ratio (MTR) measurement of the abdomen could be challenging due to the impact of motion.
Goal(s): To validate if the 3D abdominal MTR could be measured under a single breath-hold using a 3D segmented EPI sequence.
Approach: This study applied a 3D segmented EPI sequence with in- and through- plane accelerations to achieve 3D MTR measurement under a single breath-hold.
Results: Three-dimensional MTR could be measured in a breath-hold of 17~18s, where 8s for a MT-on acquisition and 8s for a MT-off acquisition and a second or two for the system adjustment.
Impact: Three-dimensional abdominal MTR measurement could be feasible in a single breath-hold using 3D EPI sequence. The gastrointestinal motility was noticed even at a time interval of 8s, which could impact the stability of the MTR measurement.
Introduction
Magnetization transfer (MT) preparation pulse has been utilized to detect the protons exchanged between two compartments, i.e., free water and macromolecular-bounded water 1. The signal intensity changes between MT preparation pulse on (MT-on) and off (MT-off) are defined as MT ratio (MTR), which has been applied in investigating neurodegeneration 2, evaluating tumor treatment response 3, and characterizing the degree of Crohn disease 4. Pixel-by-pixel calculation of MTR is sensitive to multiple sources of motions including cardiac, respiratory, and gastrointestinal motility of abdominal organs. Breath-holding (BH) is an intuitive way to avoid breathing artefact, which allows for a single slice MTR measurement using the conventional GRE acquisition 5. MT-prepared 3D seg-EPI sequence in combination with in- and through-plane acceleration strategy 6 may be possible for a 3D abdominal MTR measurement in a single breath-hold. However, the susceptibility artifact using large EPI factors could be associated with image distortions. Thus, this study aims to evaluate the feasibility of the abdominal MTR measurement in a single BH via optimizing the MT-prepared 3D seg-EPI sequence.Methods
A research segmented 3D-EPI sequence was employed in this study. The EPI factor and other imaging parameters were adjusted to achieve an acquisition time of 8s per measurement for the 3D abdominal volume, while keeping susceptibility artifact low. The measurement was performed two times, i.e., once with MT preparation and another time without MT preparation. Including another one or two seconds of system adjustment time at the beginning of the MT-off measurement, the total acquisition took 17~18s, which can be accommodated in a single breath-hold. Imaging parameters were: FOV = 359x265 mm2, matrix size = 176x130x32, reconstructed voxel size = 2x2x5mm3, acceleration factor = 2x2, EPI factor = 5, FA = 16°, bandwidth = 2185Hz/pixel. The experiment was performed on a 3T MRI scanner (MAGNETOM Prisma, Siemens Healthineers, Erlangen, Germany) using an anterior 18-ch body coil and a posterior spine coil. Four healthy volunteers were enrolled for two experiments: a) the MTR acquisition (MT-on and MT-off pair) were performed twice on two volunteers in a time interval of ~5 mins; b) In additional to a MTR acquisition, to study the impact of gastrointestinal motility, MT-on acquisitions were repeated twice in a single breath-hold on another two volunteers, with one of them scanned with stomach full. The MTR was calculated offline via (MT_off – MT_on)/MT_off x100% using MATLAB (v2017A, Natick, MA, USA).Results
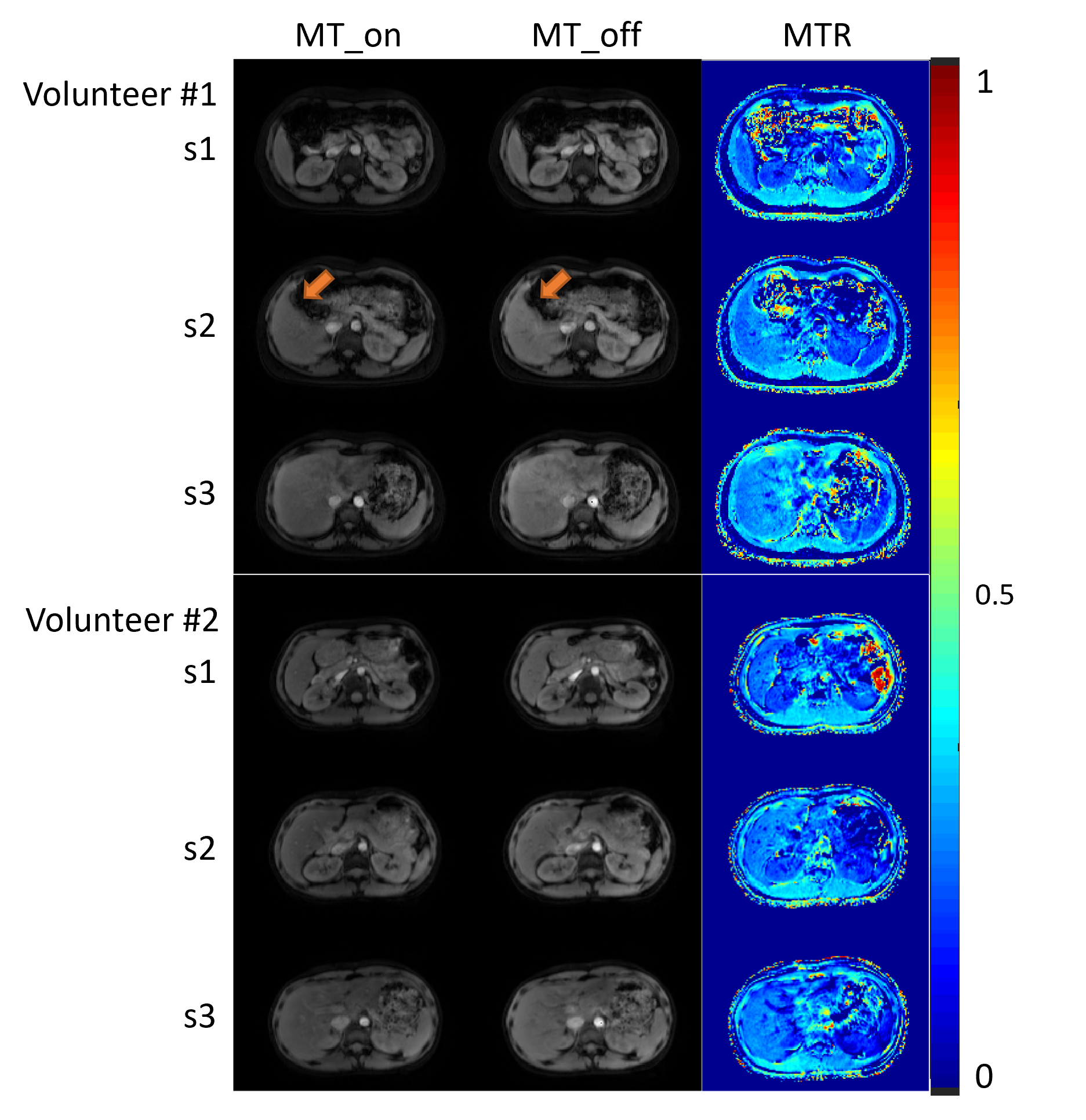
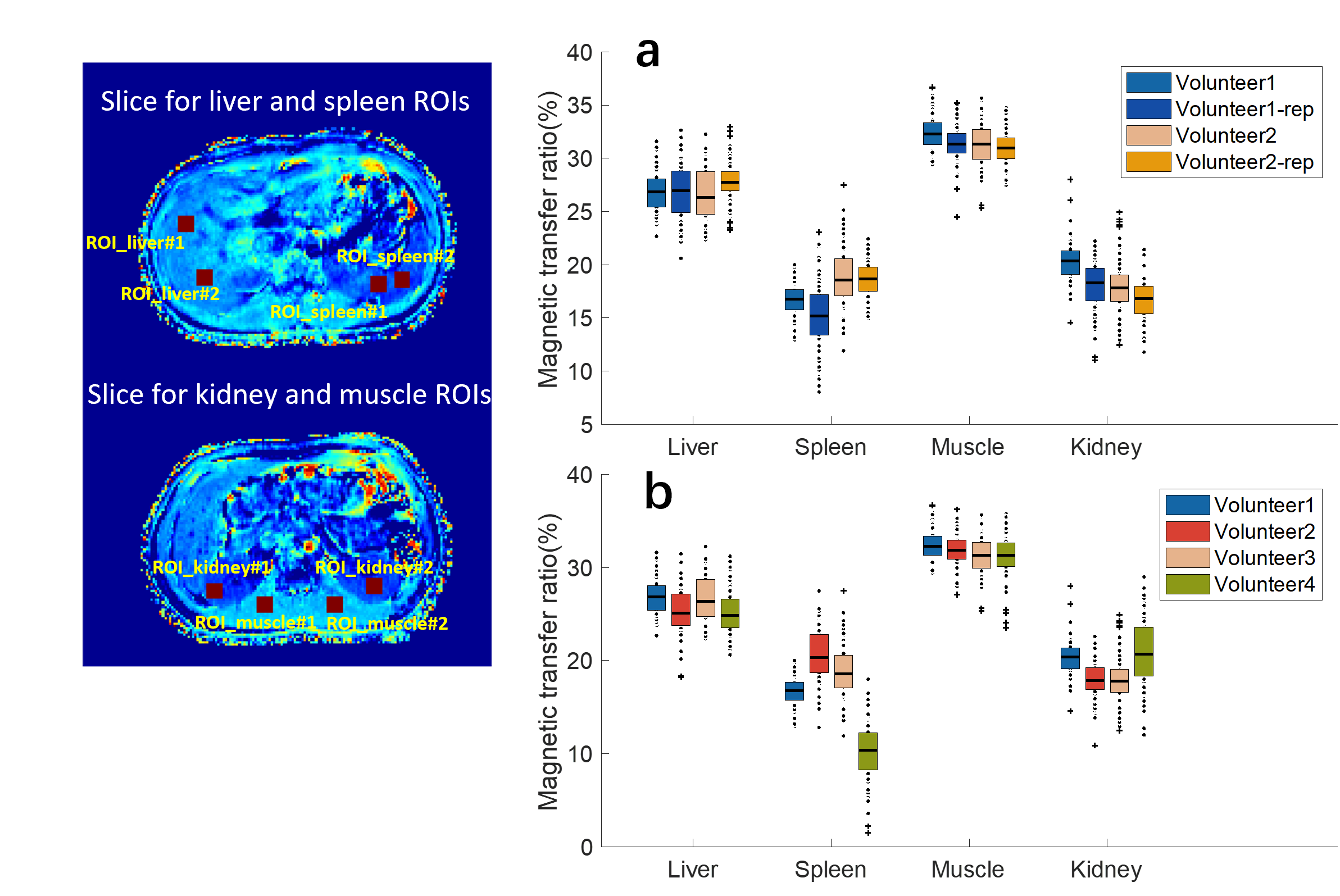
Figure 1 shows the results from two volunteers. Minor susceptibility artefact could be noticed at the interface between liver and intestinal gas from s2 of volunteer#1.Figure 2 shows the box plots of the calculated MTRs over the selected. The intra-subject MTRs are more repeatable in liver and muscle than in spleen and kidney (Figure 2a). Inter-subject MTRs also show good stability of liver and muscle, while MTRs of spleen and kidney vary significant, especially for volunteer#4 (Figure 2b).
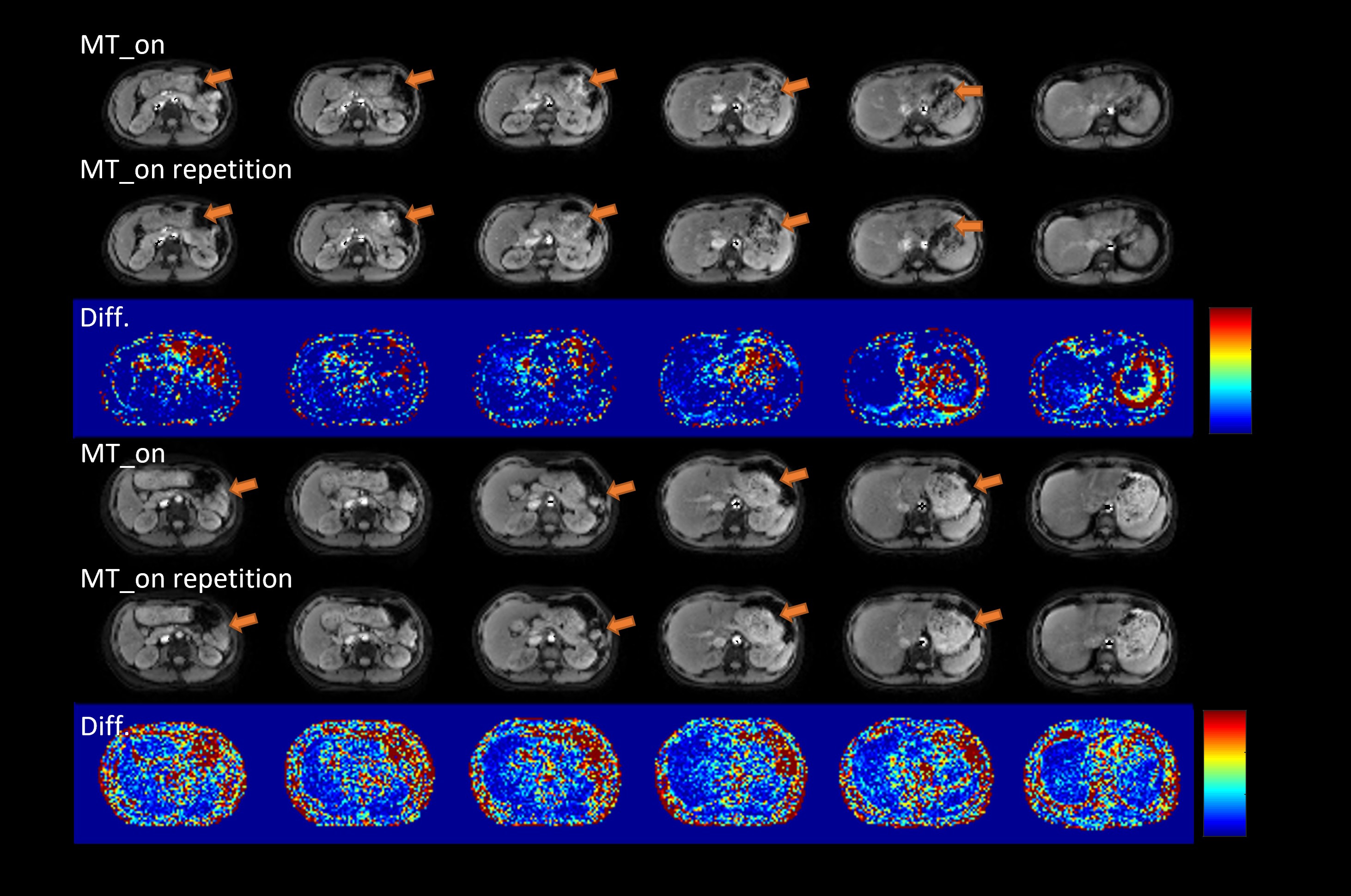
The difference maps of the two MT-on data in a single BH after normalization by the first MT-on image are shown in Figure 3. Gastrointestinal motility could be detected at both volunteers pointed by the arrows, although the stomach of volunteer#4 is much fuller than volunteer#3 (seeing images at the last three columns in Figure 3). The difference map indicates volunteer#3 performed more stable results than volunteer#4.
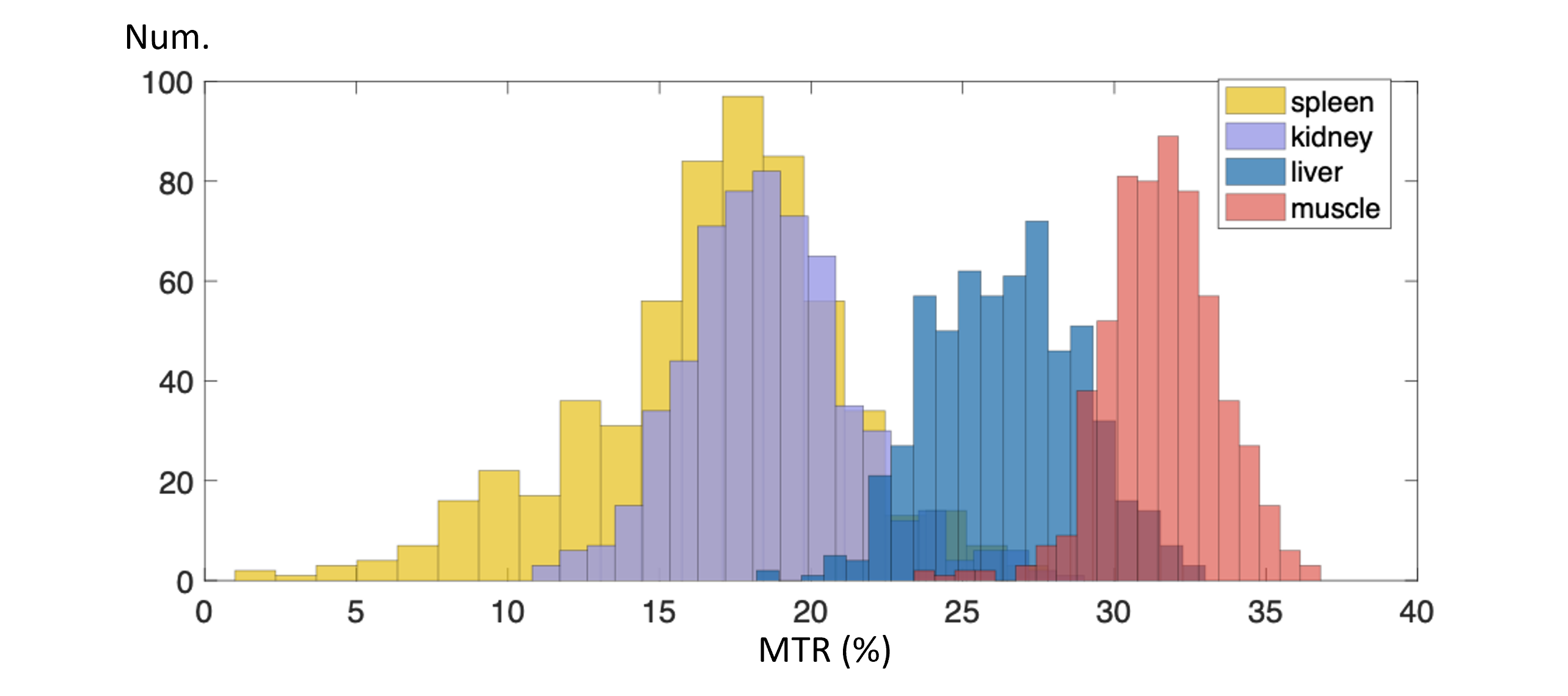
Figure 4 shows the histogram of MTR measured in liver, muscle, kidney and spleen from four volunteers. Muscle shows the highest MTR among all the organs. MTR values are summarized in Table.1.
Discussions
The study evaluated the feasibility of using the 3D segmented EPI for whole abdominal MTR measurement in a single breath-hold. Four volunteer data showed relatively stable MTR values at muscle and liver (spleen and kidney MTRs are more variable). Inconsistent partial volume effect may have contributed to the variability, because the manually chosen ROIs contain different volumes of the renal cortex and medulla.To limit the total MTR scan time, EPI factor of 5 was used at the cost of slightly increased susceptibility impacts, while minor image distortion could be noticed at the interface between liver and intestinal gas.
The gastrointestinal motility could be detected between two MT-on measurements even at an effective time interval of 8s, suggesting strict motion management at gastrointestinal tract. Imaging with the full stomach may degrade the stability of MTR measurement.
Conclusion
The preliminary results demonstrated the feasibility of using a MT pulse prepared segmented 3D EPI acquisition for abdominal MTR measurement in a single breath-hold. This study found gastrointestinal motility between two MT-on acquisitions even at a time interval of 8s.Acknowledgements
No acknowledgement found.References
1. Grossman RI, Gomori JM, Ramer KN, Lexa FJ, Schnall MD. Magnetization transfer: theory and clinical applications in neuroradiology. Radiographics. 1994 Mar;14(2):279-90. doi:10.1148/radiographics.14.2.8190954.
2. Liu Y, Li J, He N, Chen Y, Jin Z, Yan F, Haacke EM. Optimizing neuromelanin contrast in the substantia nigra and locus coeruleus using a magnetization transfer contrast prepared 3D gradient recalled echo sequence. Neuroimage. 2020 Sep;218:116935. doi: 10.1016/j.neuroimage.2020.116935.
3. Martens MH, Lambregts DM, Papanikolaou N, Alefantinou S, Maas M, Manikis GC, Marias K, Riedl RG, Beets GL, Beets-Tan RG. Magnetization transfer imaging to assess tumour response after chemoradiotherapy in rectal cancer. Eur Radiol. 2016 Feb;26(2):390-7. doi: 10.1007/s00330-015-3856-3.
4. Li XH, Mao R, Huang SY, Sun CH, Cao QH, Fang ZN, Zhang ZW, Huang L, Lin JJ, Chen YJ, Rimola J, Rieder F, Chen MH, Feng ST, Li ZP. Characterization of Degree of Intestinal Fibrosis in Patients with Crohn Disease by Using Magnetization Transfer MR Imaging. Radiology. 2018 May;287(2):494-503. doi: 10.1148/radiol.2017171221.
5. Rosenkrantz AB, Storey P, Gilet AG, Niver BE, Babb JS, Hajdu CH, Lee VS. Magnetization transfer contrast-prepared MR imaging of the liver: inability to distinguish healthy from cirrhotic liver. Radiology. 2012 Jan;262(1):136-43. doi: 10.1148/radiol.11111043.
6. Jin Jin, Monique Tourell, Pascal Sati, Sunil Patil, Kecheng Liu, John A. Derbyshire, Fei Han, et al. “Segmented 3D EPI with CAIPIRINHA for Fast, High-Resolution T2*-Weighted Imaging.” In Proc. Annu. Meeting ISMRM, 2021.
Figures