4565
Single-shot and multi-shot cardiac diffusion MRI in vivo using high-amplitude gradient of 200mT/m1Boston Children's Hospital, Boston, MA, United States, 2CREATIS UMR 5220, U1206, Lyon, France, 3Radiology department, Centre Hospitalier Universitaire de Saint-Étienne, Saint-Etienne, France, 4Siemens Healthcare SAS, Courbevoie, France, 5Siemens Healthcare GmbH, Erlangen, Germany
Synopsis
Keywords: Data Acquisition, Diffusion Tensor Imaging, Cardiac Diffusion Tensor Imaging
Motivation: High gradient hardware has the potential to reduce TE and improve SNR for Cardiac diffusion tensor imaging (cDTI) for both single-shot (SS-EPI) and multi-shot EPI (MS-EPI) approaches. However, gradient amplitude and slew rate can be limited due to Peripheral and Cardiac Nerve stimulation (PNS/CNS).
Goal(s): To compare Gmax=200mT/m and Gmax=80mT/m systems for cDTI.
Approach: Healthy volunteers (n=3) were imaged on both systems using SS-EPI and MS-EPI. PNS/CNS and diffusion parametric mapping were compared.
Results: Equivalent diffusion parameters were found for all acquisitions and systems. At Gmax=200mT/m, MS-EPI used the hardware system efficiently due to reduced PNS but remained limited by CNS.
Impact: In this work, we studied hardware limitations due to PNS/CNS for two high-gradient systems for SS-EPI and MS-EPI. MS-EPI reduces image distortions due to B0 inhomogeneities, improves SNR compared to SS-EPI, and used the most efficiently the hardware system.
Purpose
Diffusion-weighted imaging (DWI) is usually acquired using a single-shot spin-echo echo planar imaging (SS-EPI) sequence which is severely affected by image distortion due to B0 inhomogeneities1. Previous works have demonstrated that first & second-order (M0M1M2) motion-compensated diffusion encoding waveforms can be used to enable ghosting-free multi-shot EPI (MS-EPI) and reduce image distortion2. M0M1M2 waveforms are also required to compensate for cardiac motion and enable cardiac diffusion tensor imaging (cDTI). However, M0M1M2 designs lead to increased TE for an equivalent b-value compared to traditional diffusion encoding waveforms and rely on gradient hardware performance to maintain a low TE3-5. The newest generation of whole-body gradient hardware allows a maximum gradient intensity of up to 200mT/m. High gradient hardware has the potential to reduce TE and improve SNR for cDTI, however maximum gradient amplitude and slew rate are usually limited due to the risk of peripheral and cardiac nerve stimulation (PNS/CNS). In this work, high (80mT/m) and very high-performance gradient systems (200mT/m) were compared for cDTI. PNS, CNS and TE obtained with both SS-EPI, and MS-EPI were analyzed in healthy volunteers.Methods
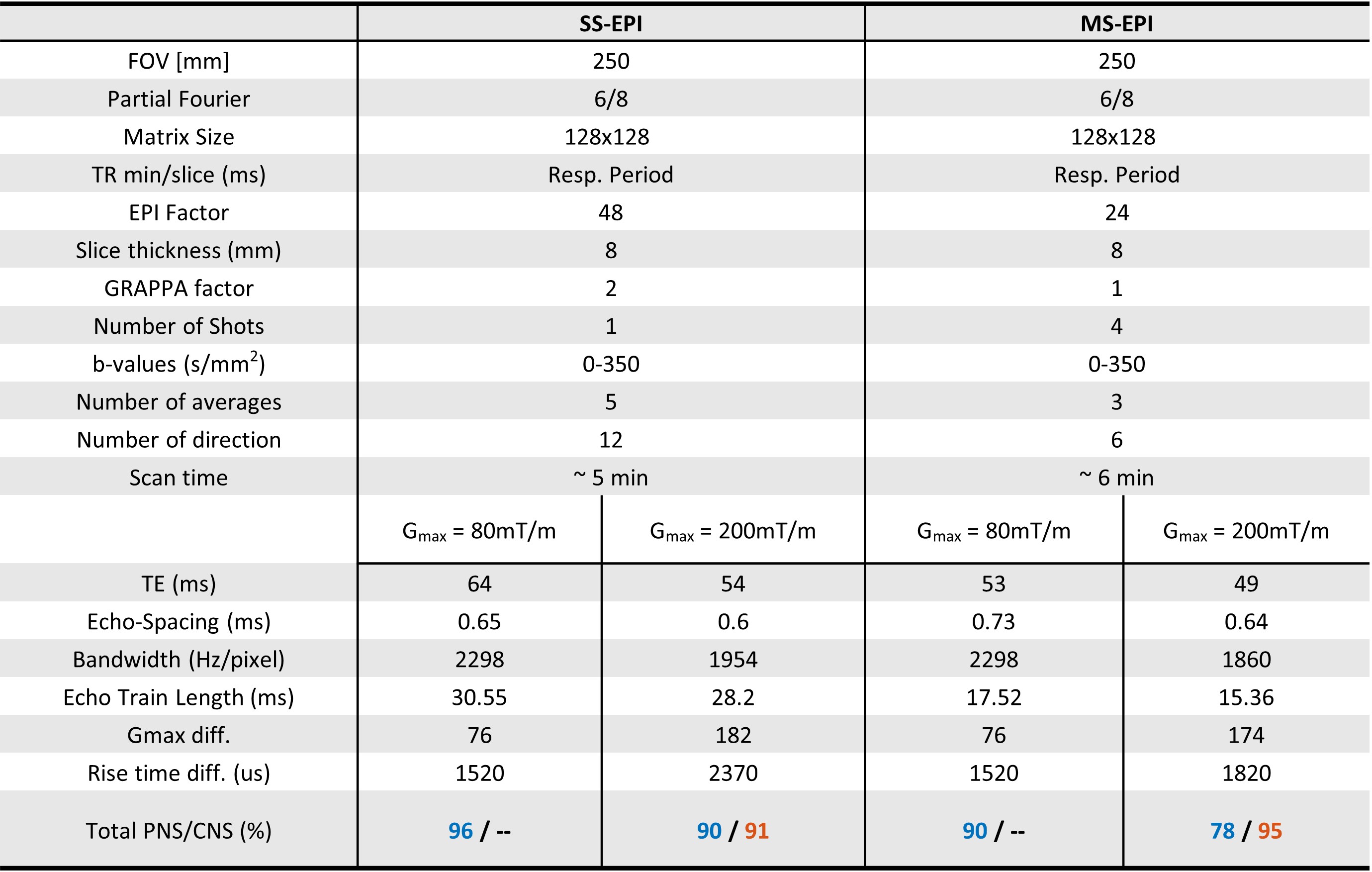
Data AcquisitionHealthy volunteers (N=3) were scanned at 3T on a high-performance scanner (MAGNETOM Prisma, Gmax=80mT/m, SRmax=200mT/m/s, Siemens Healthcare, Erlangen, Germany) and very high-performance scanner (MAGNETOM Cima.X, Gmax=200mT/m, SRmax=200mT/m/s, Siemens Healthcare, Erlangen, Germany) following written informed consent. In each scanner, two sets of cDTI images were acquired per volunteer using prototype diffusion SS-EPI and MS-EPI sequences with first and second-order (M0M1M2) motion-compensated diffusion encoding waveforms3,4. One short-axis slice was acquired in mid-systole using ECG-gating and in expiratory using a navigator triggering6. For each acquisition, the sequence parameters were manually adjusted to reduce the TE while maintaining the PNS/CNS below the limit. Sequence parameters are detailed in Table 1.
Post-processing and analysis
Inline in-plane non-rigid image registration was performed across b-values, diffusion directions, and averages. Signal averaging and tensor fitting were performed offline in Matlab (MathWorks, Natick, MA). Fraction of anisotropy (FA) and mean diffusivity (MD) were measured after manual segmentation of the left ventricle (LV). SNR was calculated across diffusion direction and averages. FA, MD and SNR were reported as mean values ± SD across the LV. PNS was simulated offline by using the same sequence parameters using the vendor’s PNS model. A CNS model in place for the Gmax=200mT/m system was also simulated and analyzed.
Results
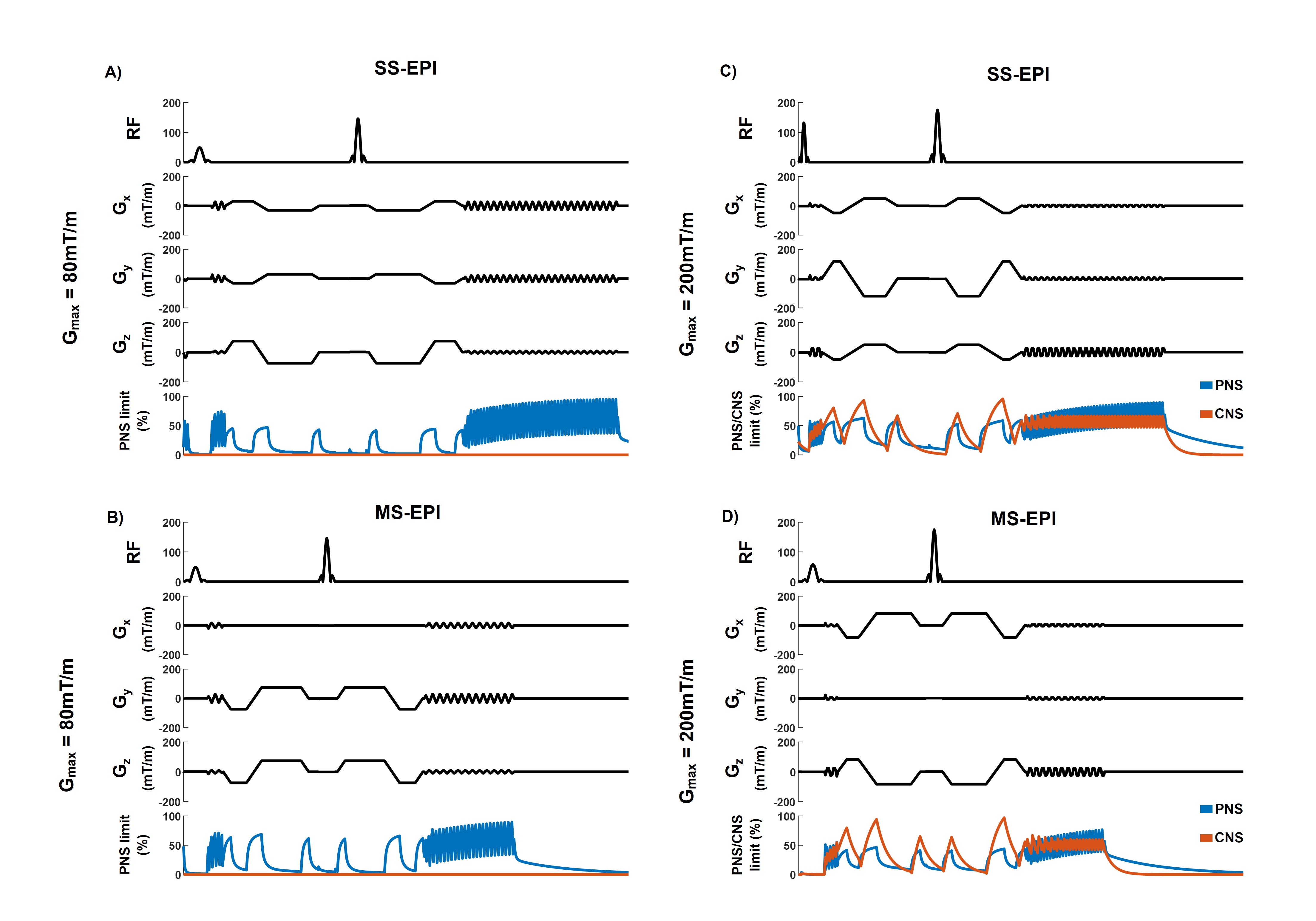
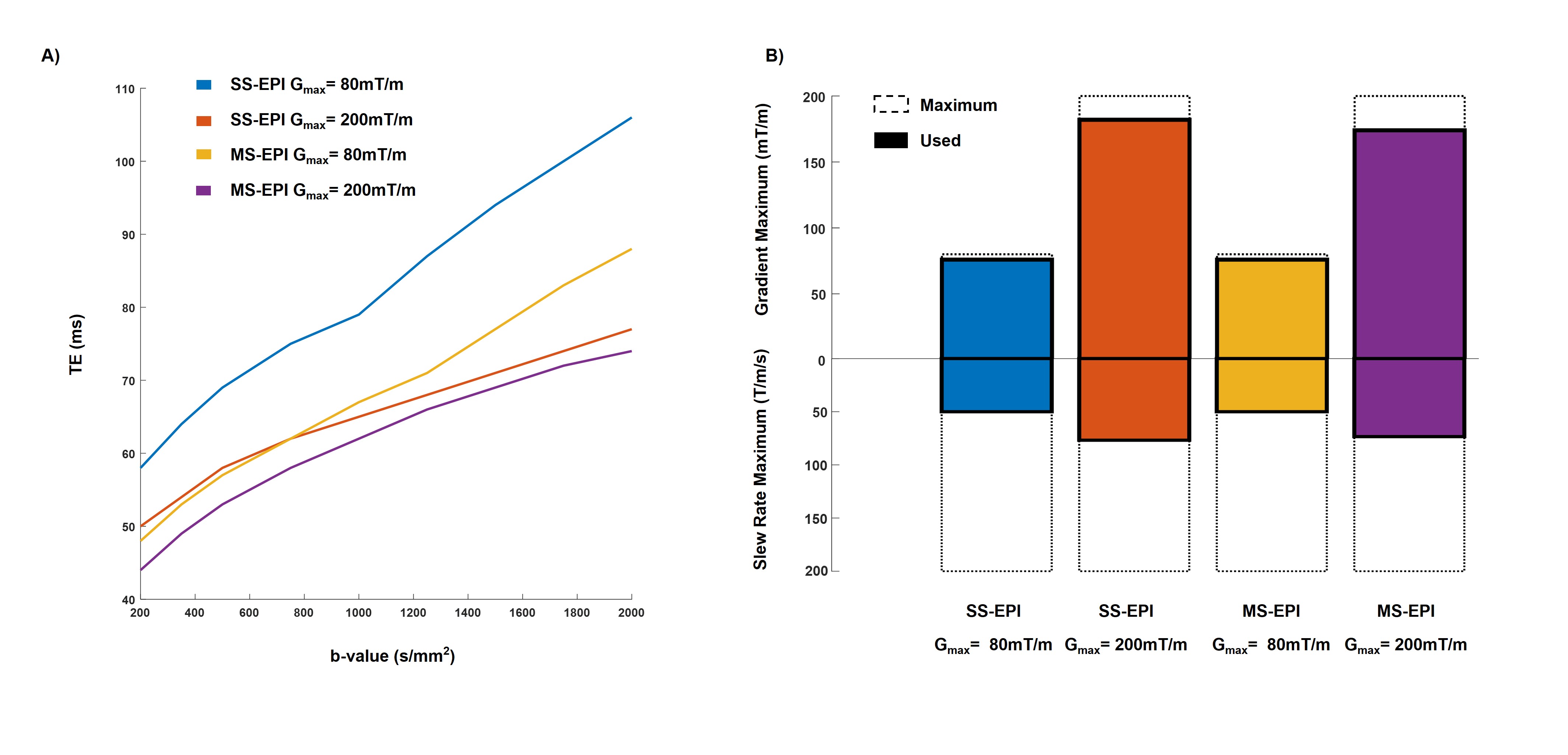
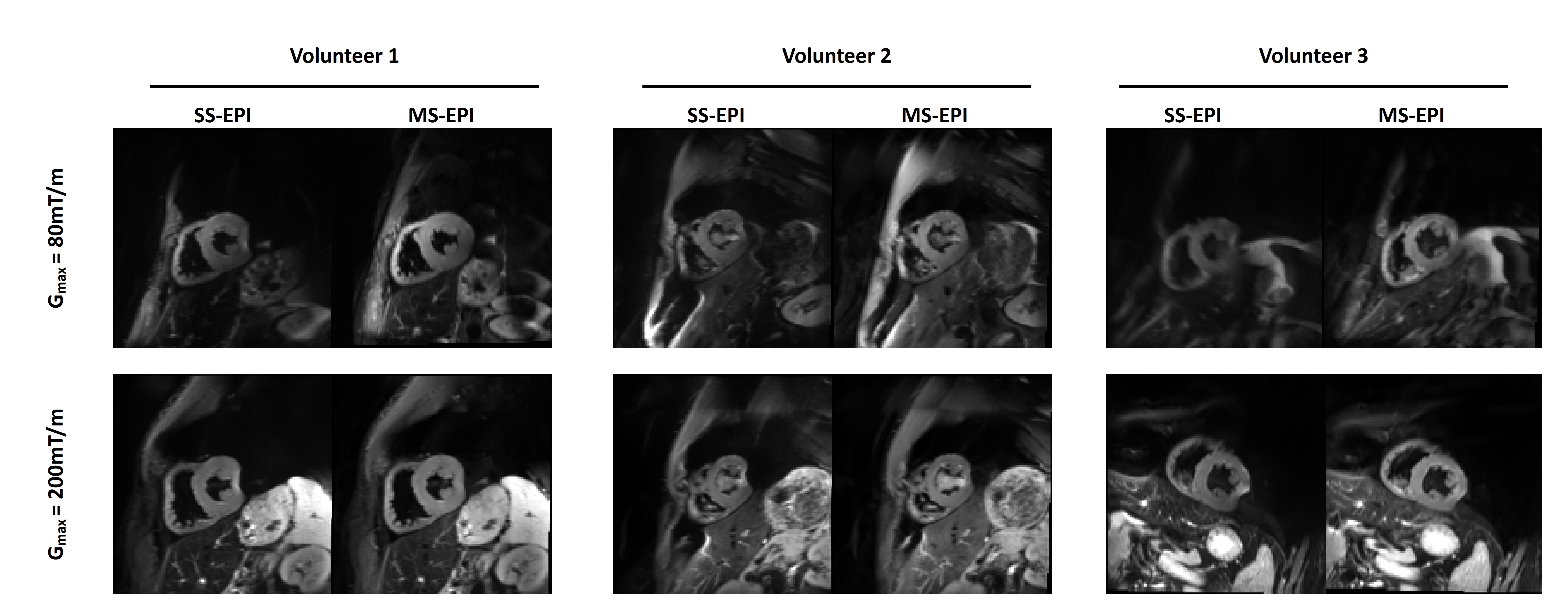
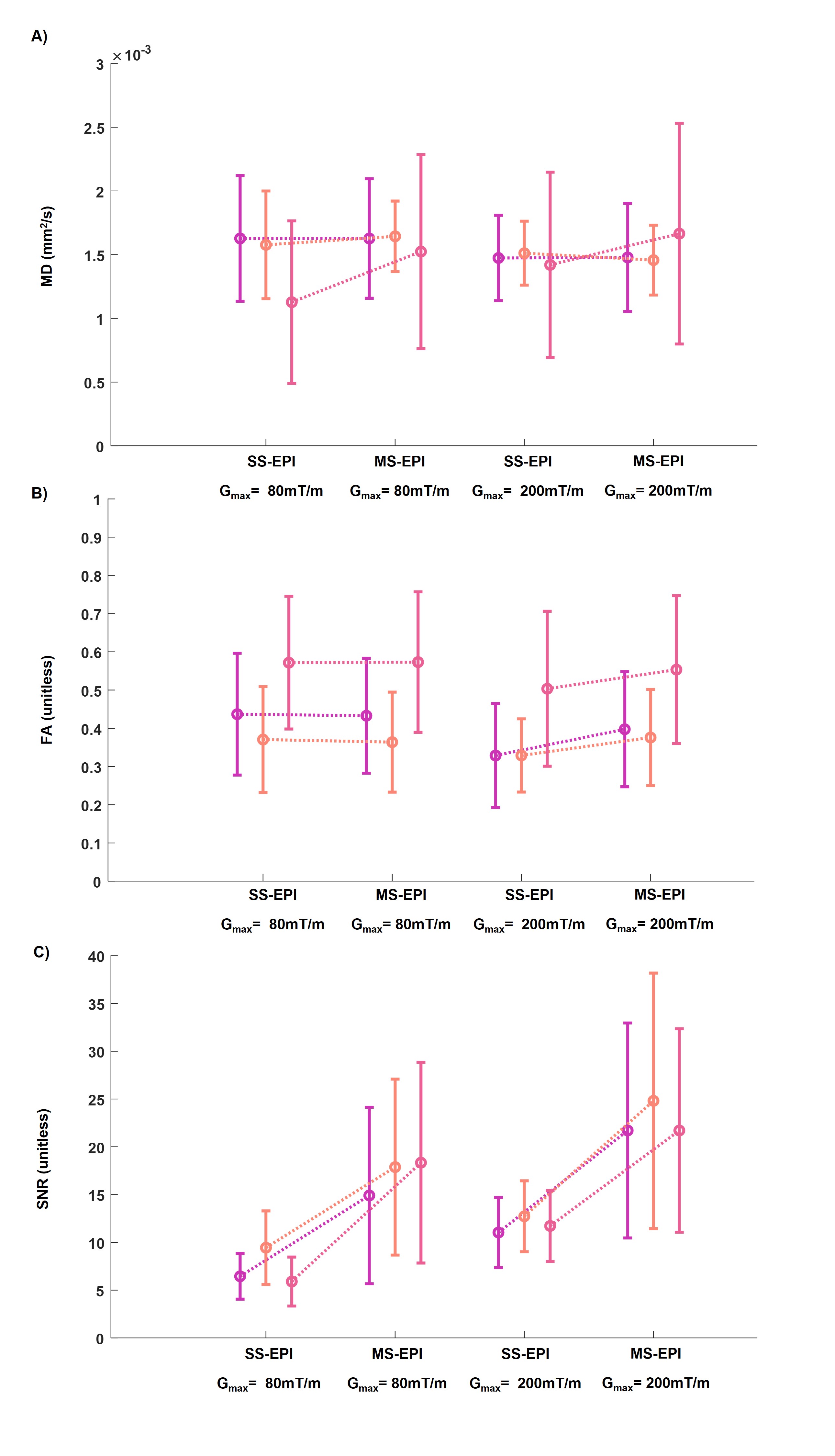
Sequence diagrams and corresponding PNS and CNS stimulation for SS-EPI and MS-EPI for Gmax=80mT/m and Gmax=200mT/m systems are shown in Figure 1. As shown in Table 1, for a b-value of 350s/mm2, Gmax=200mT/m system allows a significant reduction of TE by 10ms and 4ms compared to the Gmax=80mT/m system, for SS-EPI and MS-EPI respectively. As shown in Figure 2-A, for higher b-values the TE difference is amplified between systems. Both systems’ performances are limited, mainly by reducing the diffusion gradients SR (Figure 2-B). CNS limit mainly impact the diffusion preparation while PNS limits is reached due to EPI long echo train-length. For the MS-EPI sequence at Gmax=200mT/m, CNS is the main limiting factor.An example of cDTI trace images for SS-EPI and MS-EPI for both systems for three volunteers is shown in Figure 3. Different levels of distortion are observed between systems for a given volunteer due to setup difference since the scans have been performed with one week interval. The reduction of image distortion from SS-EPI to MS-EPI is clearly visible in the lateral region in both systems. MD, FA, and SNR for all volunteers and all scans are reported in Figure 4. Overall, no differences were observed between MD and FA between SS-EPI and MS-EPI across systems and volunteers. For the Gmax=80mT/m system, the SNR was doubled from 7.3±1.9 to 17.0±1.9, from SS-EPI to MS-EPI respectively. For the Gmax=200mT/m system, SNR is also doubled from 11.8±0.8 to 22.7±1.8, from SS-EPI to MS-EPI respectively.
Discussion
In this work, cardiac diffusion imaging using SS-EPI and MS-EPI were studied for two systems with maximum gradient of Gmax=80mT/m and Gmax=200mT/m. Equivalent MD and FA across all acquisitions and systems. MS-EPI was found to significantly reduce image distortions due to B0 inhomogeneities and improve SNR compared to SS-EPI. At Gmax=200mT/m, MS-EPI used the most efficiently the hardware system and reduced the overall PNS but remained limited by CNS. MS-EPI in combination with high performance gradients are a promising perspective to increased structural resolution and reduced diffusion time.Acknowledgements
No acknowledgement found.References
1. Bammer R. Basic principles of diffusion-weighted imaging. Eur. J. Radiol. 2003
2. Moulin et al. Prospective correction of multi-shot diffusion imaging using motion compensation and dual-speed EPI. Proc. ISMRM 2022 London.
3. Aliotta et al. Convex Optimized Diffusion Encoding (CODE) Gradient Waveforms for Minimum Echo Time and Bulk Motion–Compensated Diffusion-Weighted MRI. MRM 2017.
4. Stoeck et al. Second-Order Motion-Compensated Spin Echo Diffusion Tensor Imaging of the Human Heart. MRM 2016
5. Welsh et al. Higher-Order Motion-Compensation for In Vivo Cardiac Diffusion Tensor Imaging in Rats. IEEE TMI 2015
6. Moulin et al. Probing cardiomyocyte mobility with multiphase cardiac diffusion tensor MRI. PlosOne 2020.
Figures