4564
Deep Learning Reconstruction (DLR) in Liver MRI: Comparison of Image Quality and diagnostic efficiency of LAVA sequence1West China Hospital of Sichuan University, chengdu, China, 2GE Healthcare,MR Research, Beijing, China
Synopsis
Keywords: Image Reconstruction, Liver, Deep Learning, Liver MR, LAVA sequence
Motivation: The potential of DLR to improve the quality of liver acquisition with volume acceleration (LAVA) sequence images and its impact on lesion diagnosis has not been extensively reported.
Goal(s): This study aims to investigate the utility of DLR in liver MR by comparing the image quality and diagnostic efficacy of the original LAVA sequence in the venous phase with the DL-LAVA sequence.
Approach: The image quality and diagnostic performance of the DL-LAVA sequence were compared with the original LAVA sequence.
Results: The results revealed that the DL-LAVA sequence significantly improved the image quality of the LAVA sequence, and its diagnostic performance was superior.
Impact: The results show that DLR can significantly improve the image quality of LAVA sequence, which may improve the detection and diagnosis of liver-related lesions, providing a powerful imaging basis for prevention and treatment.
Background and Purpose
In recent years, the development of artificial intelligence and deep learning has significantly transformed the field of magnetic resonance imaging. Numerous studies have demonstrated the advantages of deep learning reconstruction (DLR) technology in improving the quality of magnetic resonance images 1-4. However, the potential of DLR to improve the quality of liver LAVA sequence images and its impact on lesion diagnosis has not been extensively reported. Therefore, this study aims to investigate the utility of DLR in liver MR by comparing the image quality and diagnostic efficacy of the original LAVA sequence in the venous phase with the DL-LAVA sequence.Methods
This is a retrospective, single-center study, which was approved by the institutional review board. The requirement for informed consent was waived. 45 patients who underwent liver LAVA enhanced examination from June 2023 to September 2023 were included. All patients' liver MR examinations were completed on a 3T MR scanner (SIGNA Premier 3T, GE Healthcare, Milwaukee, USA). A 30-channel AIRTM Anterior Array Coil (GE Healthcare, USA) was used. The venous phase LAVA scan is obtained after 180 seconds of injection of contrast medium, and the machine automatically reconstructs the original LAVA and DL-LAVA images. The LAVA sequence parameters were as follows: TR = 3.5 ms, TE = 1.3 ms, flip angle = 15°, FOV = 380 × 380 mm , slice thickness = 1.2 mm, acquisition voxel size = 1.2 × 1.7 × 2.4 mm, acceleration = 2, NEX = 1, scanning time = 15 s,DLR strength = High. Two radiologists (Reader 1 with 7 years of experience and Reader 2 with 15 years of experience) conducted subjective and objective evaluations of image quality without knowing all other patient information. The subjective evaluation of the image quality uses a 5-point Likert scale 5, including image conspicuity, artifacts, diagnostic confidence, and overall image quality. The two radiologists independently measured the signal intensity (SI) of the liver, spleen, erector spinal muscle, and subcutaneous fat at the level of the portal vein. They also measured the standard deviation (SD background) within the background air ROI located directly posterior to the spinous process at the same plane as the image noise 6. The diagram of ROI is shown in Figure 1. The average of the two radiologists' measurement results was used for objective evaluation of image quality. Objective evaluation includes SNR, CNR, and contrast, with the following calculation formulas:$$SNR=\frac{SI_{tissue}}{SD_{background}}$$
$$CNR=\frac{|SI_{tissue1}-SI_{tissue2}|}{SD_{background}}$$
$$Contrast=\frac{|SI_{tissue1}-SI_{tissue2}|}{|SI_{tissue1}+SI_{tissue2}|}$$
Based on the diagnostic findings of a senior radiologist with 30 years of experience in abdominal imaging, Reader 1 and Reader 2 independently assessed the presence or absence of lesions in the images of the 45 included patients. This assessment was conducted using the original LAVA and DL-LAVA sequences during the venous phase. Additionally, they measured the signal intensity (SI) value, as well as the maximum and minimum diameters of the largest lesion in each case. Statistical analysis was performed using SPSS 25.0 (IBM, Armonk, New York, USA). A paired Wilcoxon signed rank sum test and paired sample t-test were used to compare subjective and objective image quality and lesion size. To evaluate the diagnostic performance of the two physicians for the lesions, the receiver operating characteristic (ROC) curve was employed, and comparison was conducted using the DeLong test. P<0.05 was considered statistically significant.
Results
A total of 45 patients were included, of which 26 had lesions. The image quality of the DL-LAVA sequence was superior to that of the original LAVA (P<0.05), as shown in Figure 2. There was no statistical difference in the maximum diameter (P=0.121) and minimum diameter (P=0.911) of the largest lesion between the DL-LAVA sequence and the original LAVA, Figure 3. The AUC, sensitivity, and specificity of Reader 1 for diagnosing lesions based on the original LAVA and DL-LAVA sequences were 0.851, 80.77%, and 89.47%, respectively, and 0.890, 88.46%, and 89.47%, respectively. The AUC, sensitivity, and specificity of Reader 2 for diagnosing lesions based on the original LAVA and DL-LAVA sequences were 0.897, 84.62%, and 94.74%, respectively, and 0.916, 88.46%, and 94.74%, respectively. Detailed diagnosis results are shown in Figure 4 and Figure 5.Discussion and Conclusion
DLR can significantly improve the image quality of the LAVA sequence without affecting the diameter measurement of lesions. Furthermore, although there is no statistical difference in improving the diagnostic performance of lesions, the AUCs based on the DL-LAVA sequence were higher than those based on the original LAVA for both radiologists.Acknowledgements
None
References
1. Ueda, T, Ohno, Y, Yamamoto, K, et al. Deep Learning Reconstruction of Diffusion-weighted MRI Improves Image Quality for Prostatic Imaging. Radiology. 2022; 303 (2): 373-381.
2. van der Velde, N, Hassing, HC, Bakker, BJ, et al. Improvement of late gadolinium enhancement image quality using a deep learning-based reconstruction algorithm and its influence on myocardial scar quantification. Eur Radiol. 2020; 31 (6): 3846-3855.
3. Wary, P, Hossu, G, Ambarki, K, et al. Deep learning HASTE sequence compared with T2-weighted BLADE sequence for liver MRI at 3 Tesla: a qualitative and quantitative prospective study. Eur Radiol. 2023; 33 (10): 6817-6827.
4. Wilpert, C, Neubauer, C, Rau, A, et al. Accelerated Diffusion-Weighted Imaging in 3 T Breast MRI Using a Deep Learning Reconstruction Algorithm With Superresolution Processing: A Prospective Comparative Study. Invest Radiol. 2023. Online ahead of print.
5. Shanbhogue, K, Tong, A, Smereka, P, et al. Accelerated single-shot T2-weighted fat-suppressed (FS) MRI of the liver with deep learning-based image reconstruction: qualitative and quantitative comparison of image quality with conventional T2-weighted FS sequence. Eur Radiol. 2021; 31 (11): 8447-8457.
6. Li, H, Hu, C, Yang, Y, et al. Single-breath-hold T2WI MRI with artificial intelligence-assisted technique in liver imaging: As compared with conventional respiratory-triggered T2WI. Magn Reson Imaging. 2022; 93 175-180.
Figures
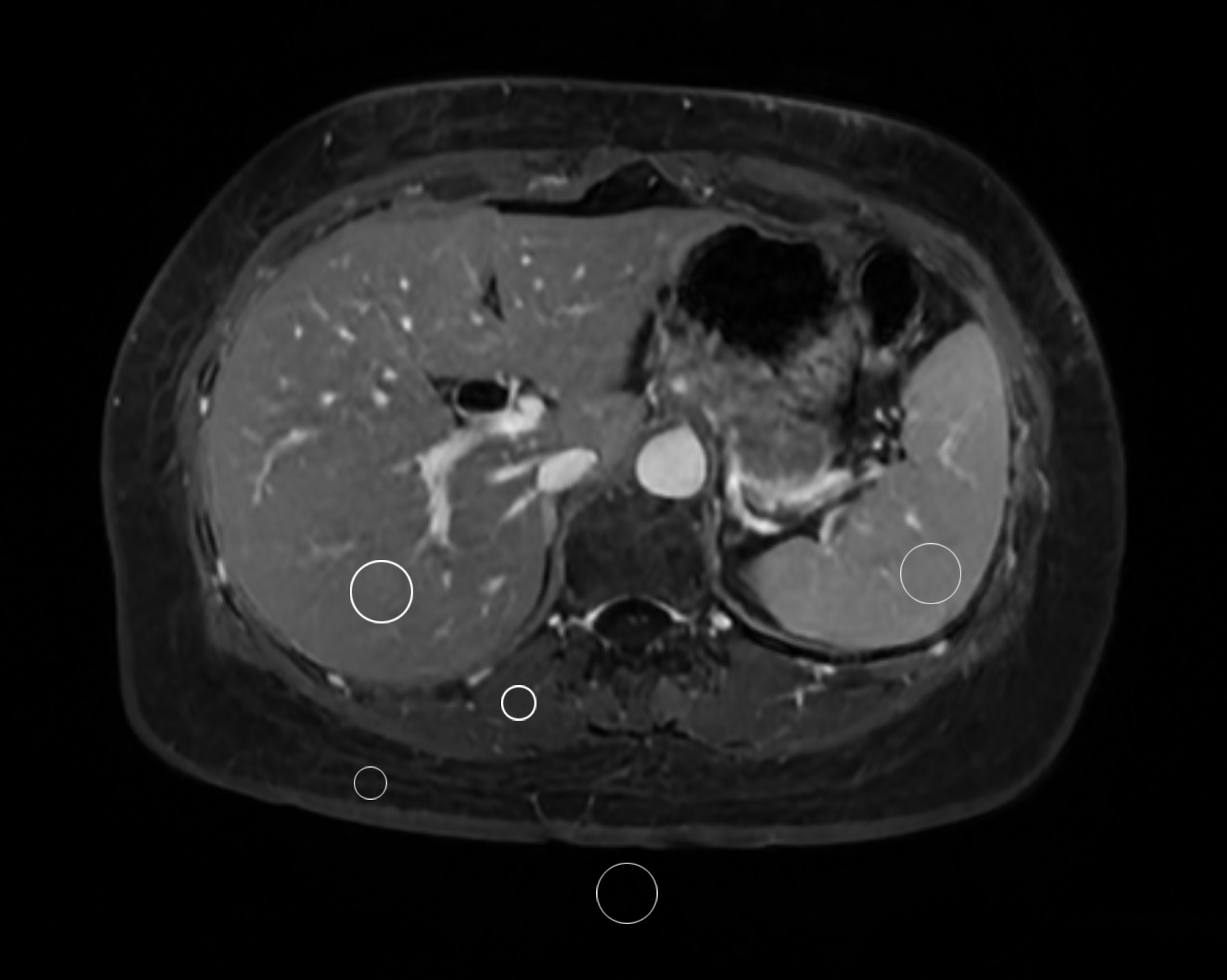
Fig.1 Schematic diagram of ROI measurement of signal intensity in the liver, spleen, erector spinal muscle, subcutaneous fat, and image noise of air.
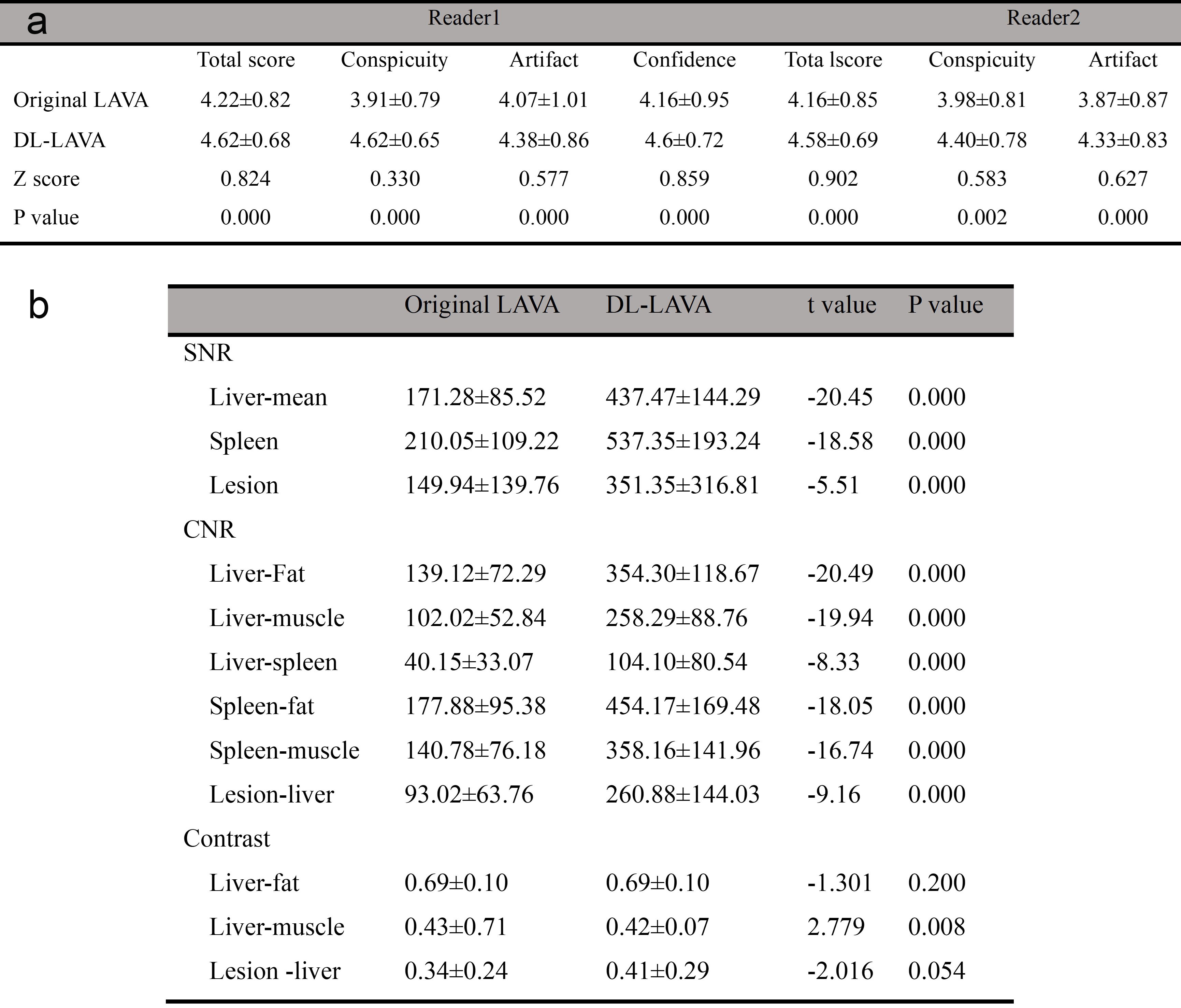
Fig.2 Comparison of subjective and objective image quality. a, Results of subjective image quality assessments by two radiologists. b, Objective image quality evaluation results.
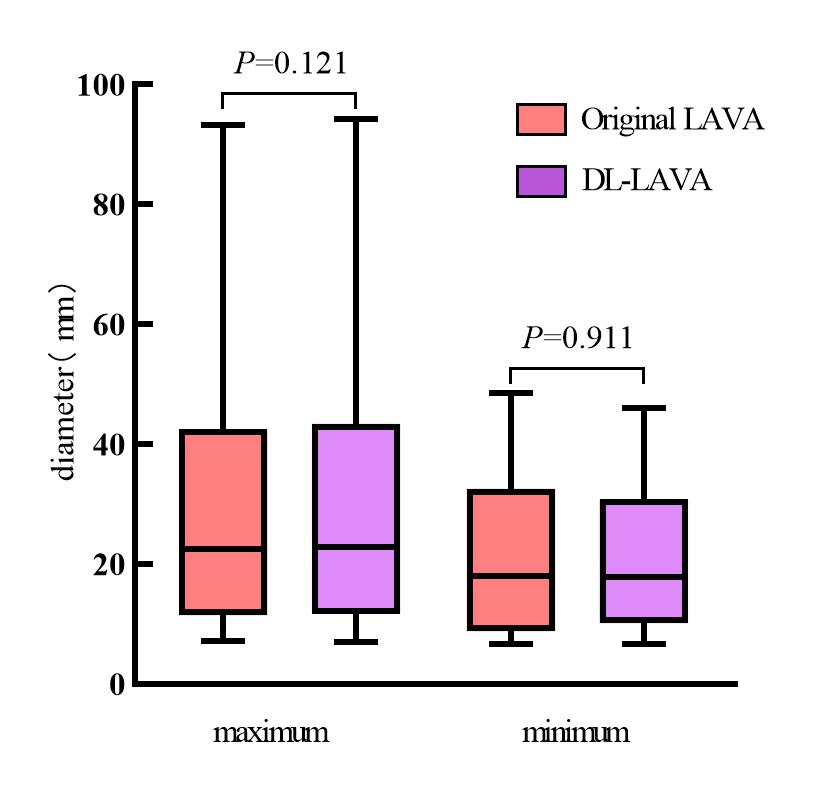
Fig.3 Comparison of the maximum and minimum diameters of the largest lesions measured on the original LAVA and DL-LAVA sequences
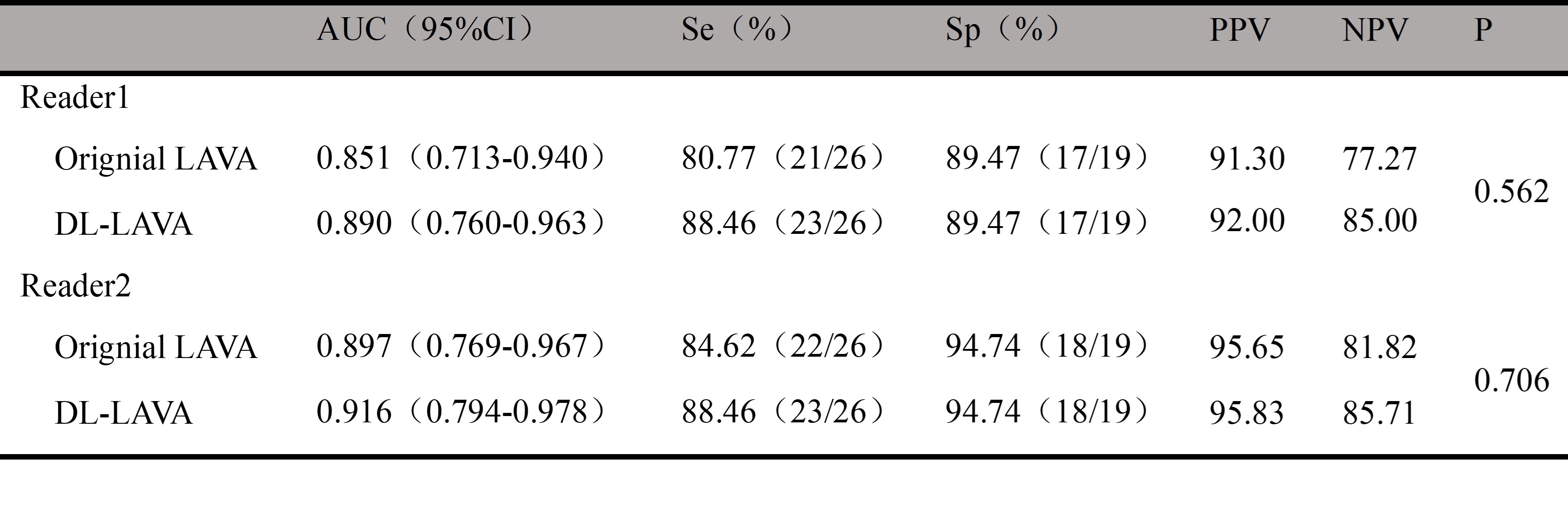
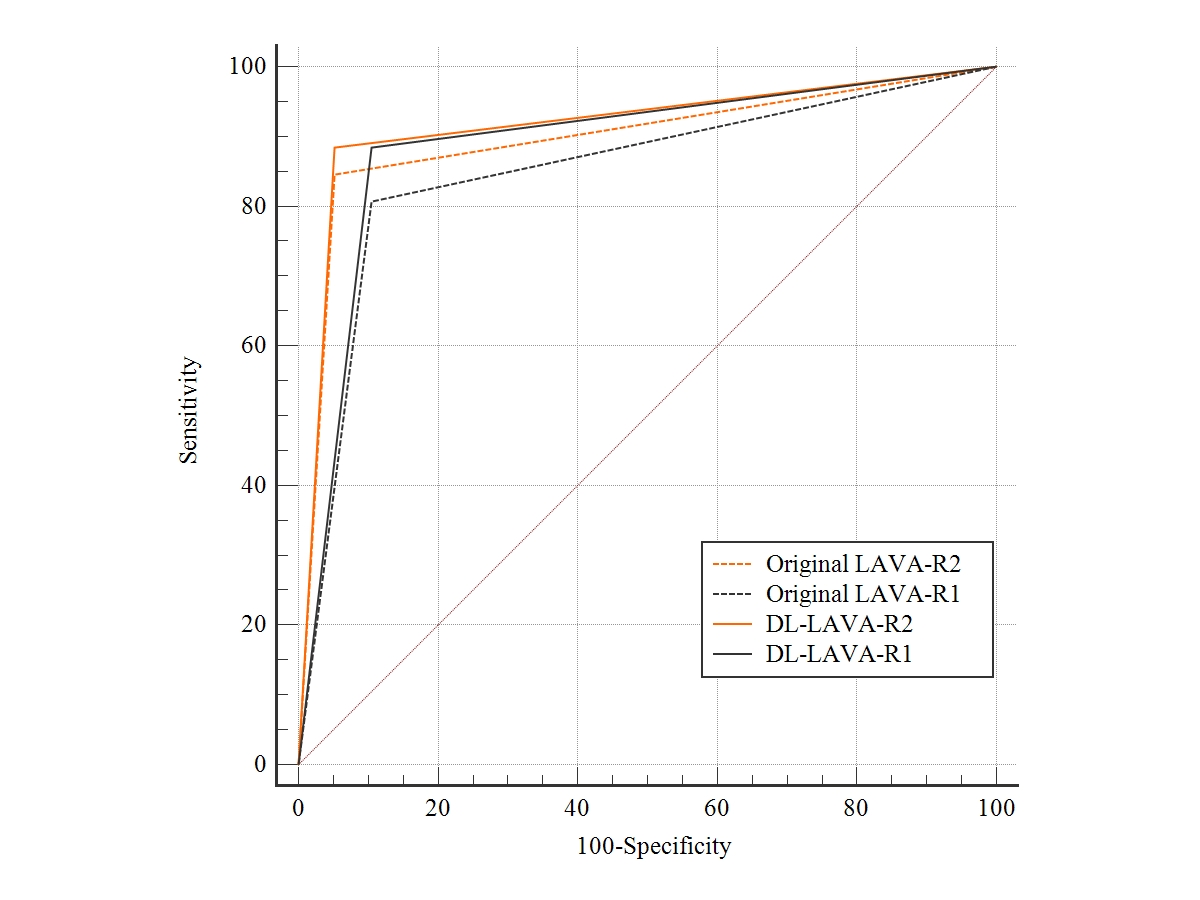
Fig.5 ROC curve of two radiologists in diagnosing lesions