4563
Cardiac Simultaneous Multi-Slice Multimapping based on Locally Low-Rank and Sparsity Constraints: Method Development and Validation1Shanghai Jiao Tong University, Shanghai, China
Synopsis
Keywords: Quantitative Imaging, Quantitative Imaging
Motivation: Simultaneous Multi-Slice (SMS) Multimapping can considerably improve the scan efficiency by acquiring myocardial T1 and T2 maps of 3 short-axis slices in 1 breath-hold.
Goal(s): To propose an accurate, precise, and reproducible SMS-Multimapping method.
Approach: A locally low-rank and sparsity-based reconstruction algorithm was developed to reduce noise and aliasing artifacts. Validation was performed in phantoms and 10 healthy subjects, where the method was compared with standard MOLLI/bSSFP T2 mapping and Multimapping.
Results: Despite the 6-fold reduction of scan time, the proposed method shows good accuracy, reasonable precision, and acceptable reproducibility in its regional myocardial T1 and T2 measurement.
Impact: The proposed method transforms a scan of 6 breath-holds down to a single breath-hold scan. Once employed, the method can greatly improve the patient comfort and efficiency of myocardial parametric mapping.
Introduction
Cardiac T1 and T2 mappings are clinically used to quantitatively evaluate myocardial fibrosis and edema1–3. However, the application of T1 and T2 mappings in 3 short-axis slices requires at least 6 breath-holds. Multimapping4 has been recently developed to acquire T1 and T2 maps in one breath-hold. A combination of Simultaneous Multi-Slice (SMS)5 and Multimapping can further reduce the scan time to one breath-hold; however, the combined in-plane and through-plane accelerations could cause a severely ill-conditioned reconstruction problem6–9. Here we propose an SMS-Multimapping sequence and a Locally Low-Rank (LLR)10–12 and Sparsity12,13 based reconstruction algorithm LLRS to both improve the scan efficiency and maintain the mapping quality. We compared the method with MOLLI, bSSFP T2 mapping, and Multimapping in 10 healthy subjects in terms of regional accuracy, standard deviation, and reproducibility.Methods
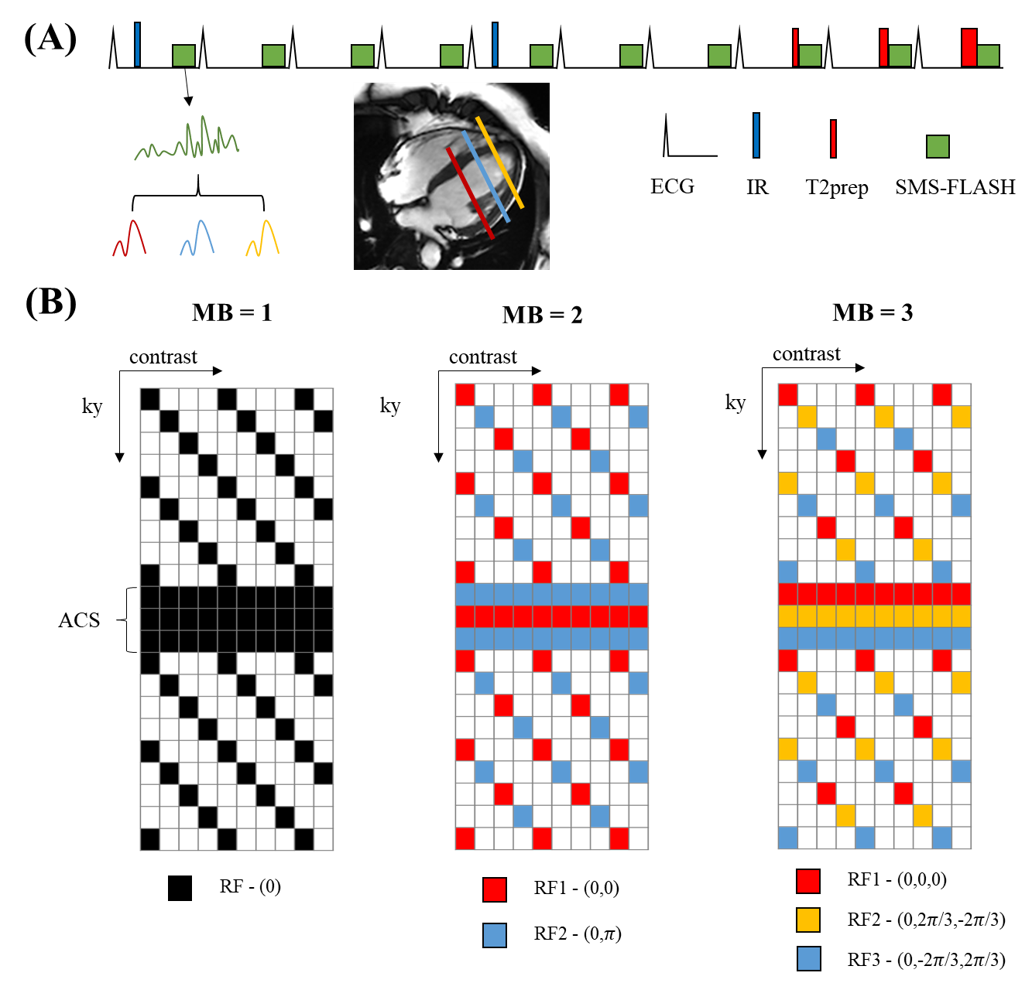
Fig. 1A shows the design of the SMS-Multimapping sequence. Similar to Multimapping, the sequence uses 10 heartbeats to generate 10 images of variable T1 and T2 weightings. However, unlike Multimapping, the SMS-Multimapping sequence uses FLASH readouts with multiband RF excitations to excite 2-3 slices simultaneously. Fig. 1B shows a schematic of the k-space sampling trajectory, which is based on the previously published SUPER-CAIPIRINHA14 sampling pattern. For multiband factors of 1, 2, and 3, the total acceleration rate is roughly 4, 8, and 12, respectively. The cost function for the underlying reconstruction problem is formulated as a sum of the data-fidelity term, LLR term, and sparsity term:$$\min _{\boldsymbol{x}} \frac{1}{2}\|\boldsymbol{y}-\boldsymbol{D F} \boldsymbol{E} \boldsymbol{x}\|_F^2+\alpha \sum_{i=1}^{N_v}\left\|\boldsymbol{B}_{i} \boldsymbol{x}\right\|_*+\beta\|\boldsymbol{W} \boldsymbol{x}\|_1$$
where $$$\boldsymbol{y}$$$ is the acquired k-space data, $$$\boldsymbol{D}$$$ the undersampling operator, $$$\boldsymbol{F}$$$ the Fourier transform, $$$\boldsymbol{E}$$$ the coil sensitivity encoding, $$$\boldsymbol{x}$$$ the multislice multi-contrast images, $$$\left \| ⋅ \right \|_{F}$$$the matrix Frobeneous norm, $$$\left \| ⋅ \right \|_{*}$$$ the nucleus norm, $$$\alpha$$$ and $$$\beta$$$ the regularization weights, $$$W$$$ is the wavelet transform, and $$$\boldsymbol{{B}} _{i}$$$ the block-extraction operator, which takes a block of voxels centered at the ith voxel to form the Casorati matrix. The above inverse problem is solved by the ADMM15 algorithm. After the reconstruction of $$$x$$$, mapping is performed by dictionary matching. The dictionary is generated by Bloch Equation simulation of the SMS-Multimapping sequence for a T1 range of [200ms:1ms:2500ms] and a T2 range of [1ms:1ms:150ms].
SMS-Multimapping was validated via phantom and in vivo imaging. Scans were performed in a 3T scanner (uMR790, United Imaging Healthcare, Shanghai, China) with a 24-channel spine coil and 12-channel torso coil. Ten healthy subjects (4 females, age 23±3 years) were imaged after the subjects provided written informed consent. Among the 10 subjects, 3 had a repeated scan a week later, enabling a preliminary evaluation of the scan-rescan reproducibility. Acquisition parameters for SMS-Multimapping were FOV/matrix size/flip angle/TR/TE/bandwidth/slice thickness/acquisition window=360×270mm2/192×138/5°/4.10ms/1.73ms/400Hz/pixel/8mm/201ms.
Results
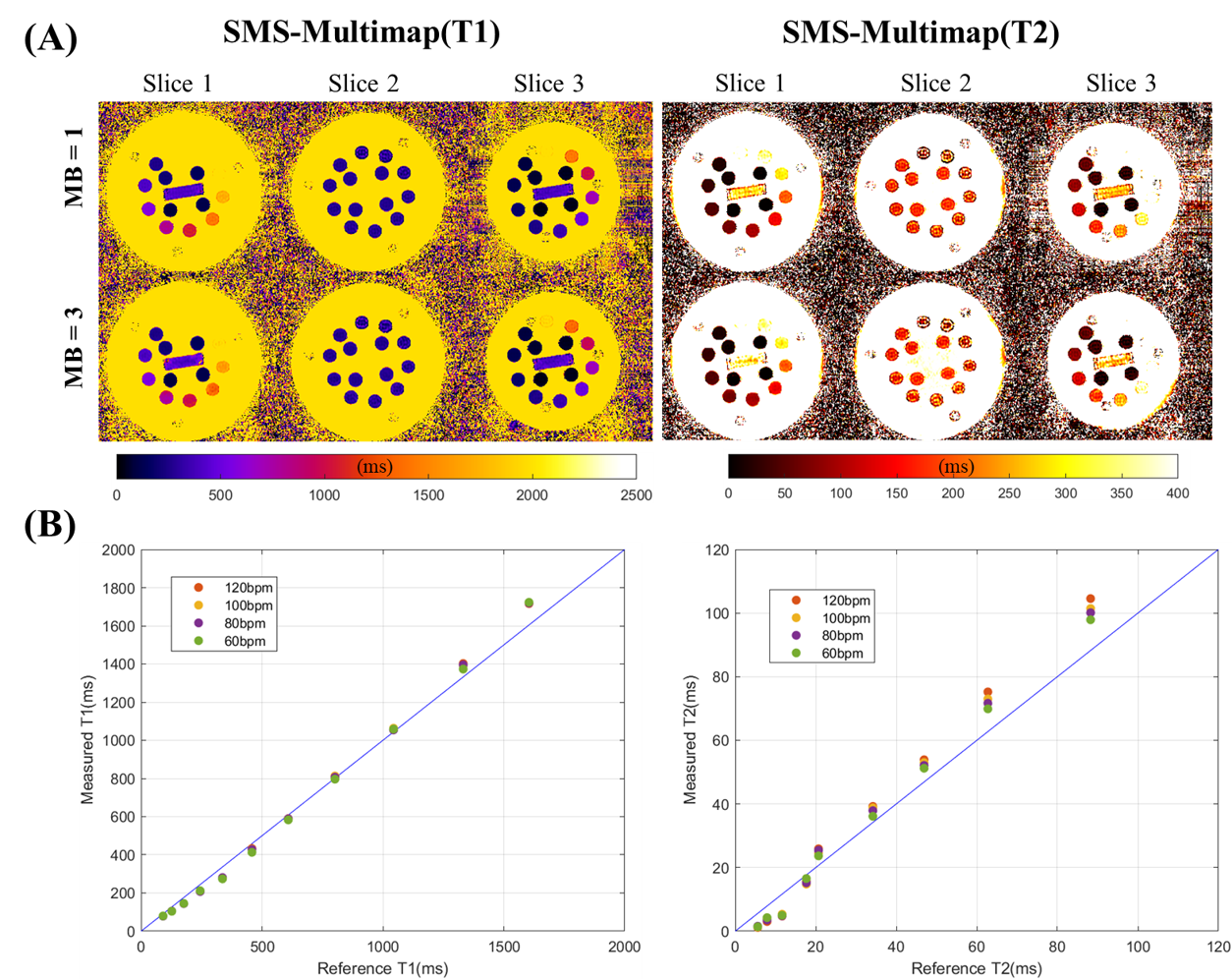
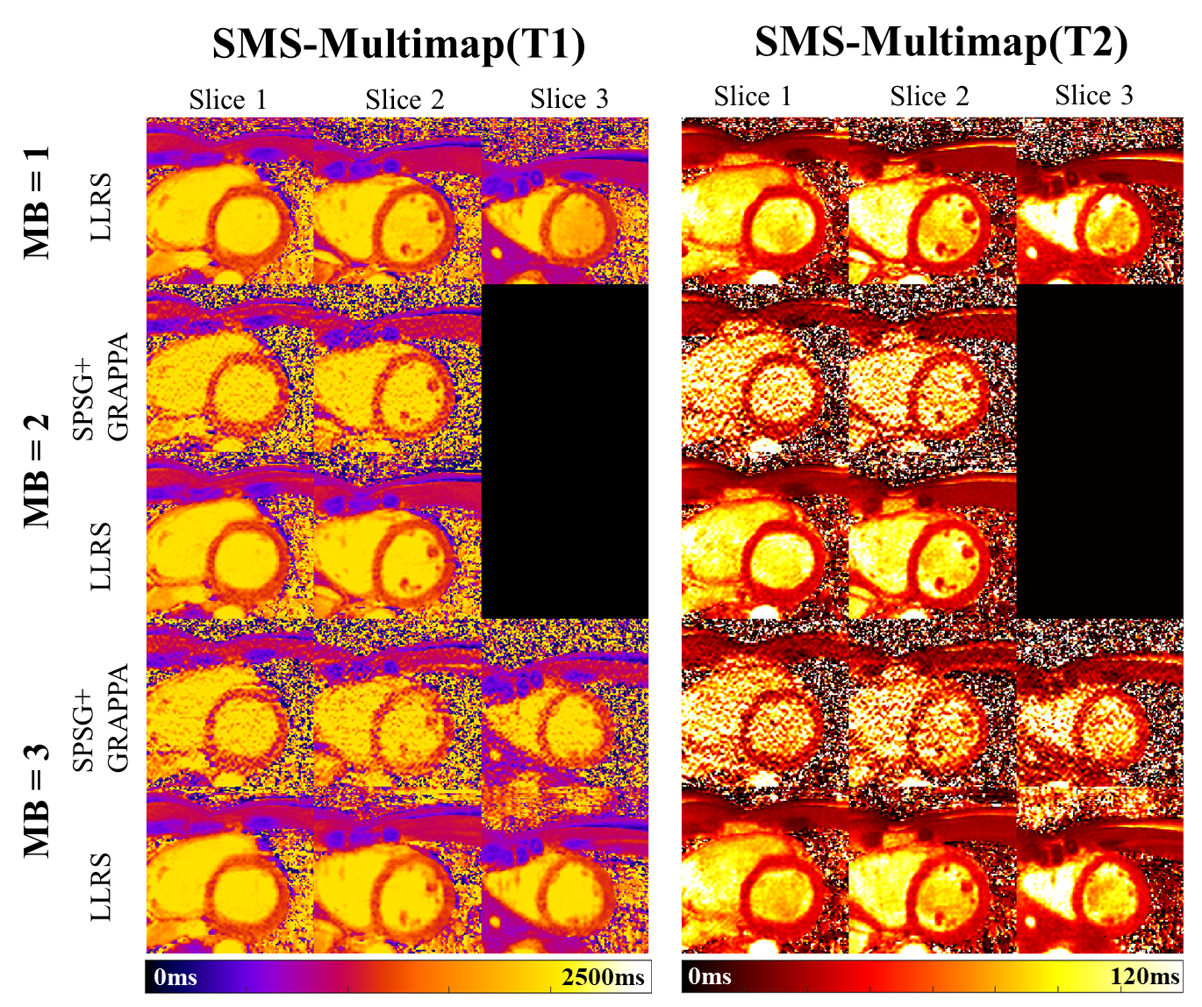
Fig. 2A shows the phantom reconstructions. Visual inspection showed a consistent quality between multiband factor=1 vs multiband factor=3. Fig. 2B shows that the T1 and T2 values measured by SMS-Multimapping (MB=3) agreed well with those measured by spin echo imaging, although errors slightly increased for larger T1, T2, and heart rates.Fig. 3 shows the in vivo reconstruction of one subject. The use of LLRS reconstruction substantially reduced the noise and aliasing artifacts compared with SPSG+GRAPPA5, which was commonly used in other SMS applications5.
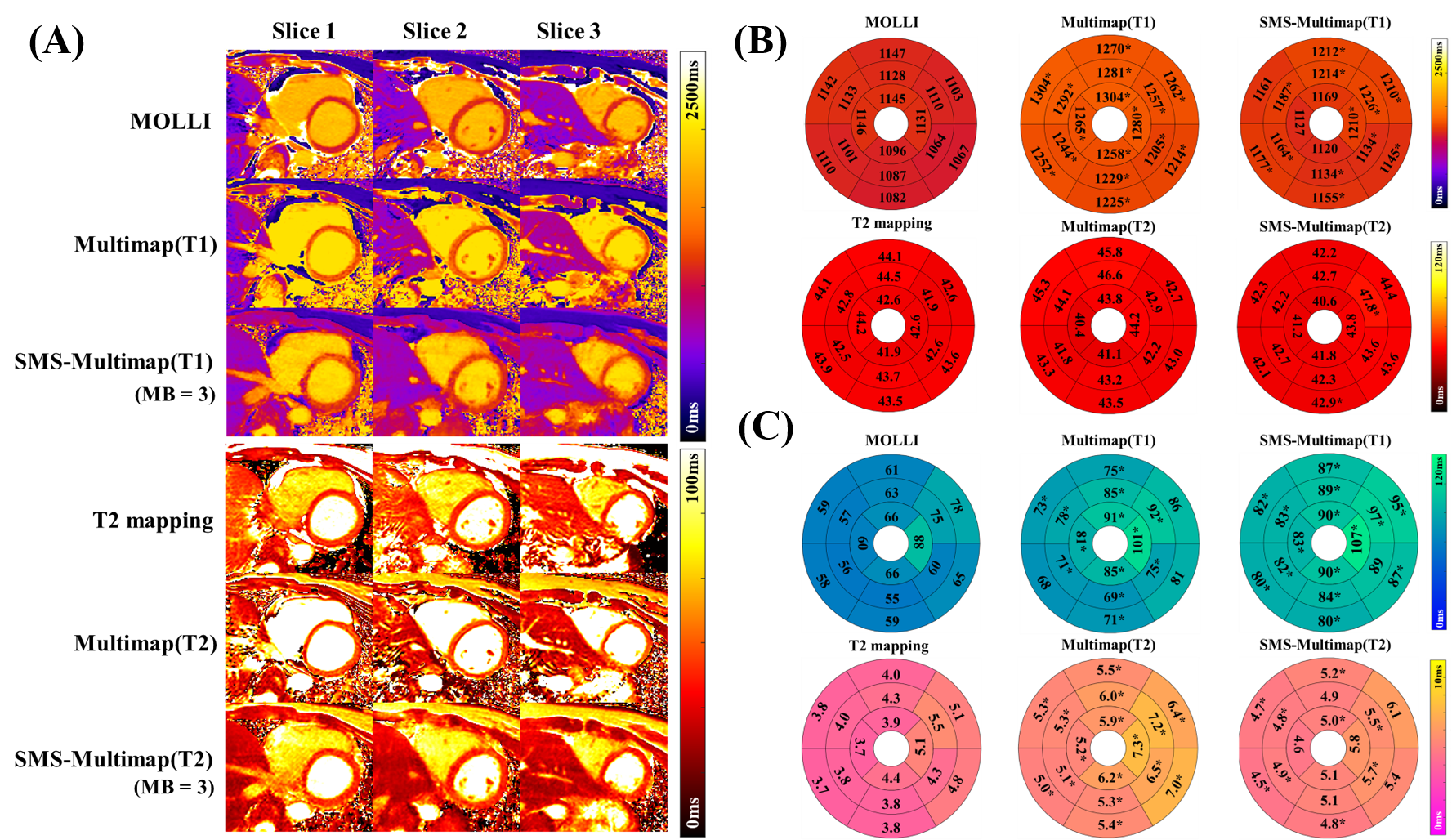
Fig. 4 shows the comparisons between MOLLI/T2 mapping, Multimapping4, and SMS-Multimapping (MB=3) in terms of visual qualities (A), regional T1/T2 means (B), and regional T1/T2 standard deviations (C) over 10 subjects. SMS-Multimapping showed an overall similar quality relative to Multimapping. Both Mutlimapping and SMS-Mutlimapping showed higher regional T1s relative to MOLLI and similar regional T2s relative to T2 mapping. SMS-Multimapping had an overall lower T1 precision relative to MOLLI and Multimapping, and a lower T2 precision relative to T2 mapping.
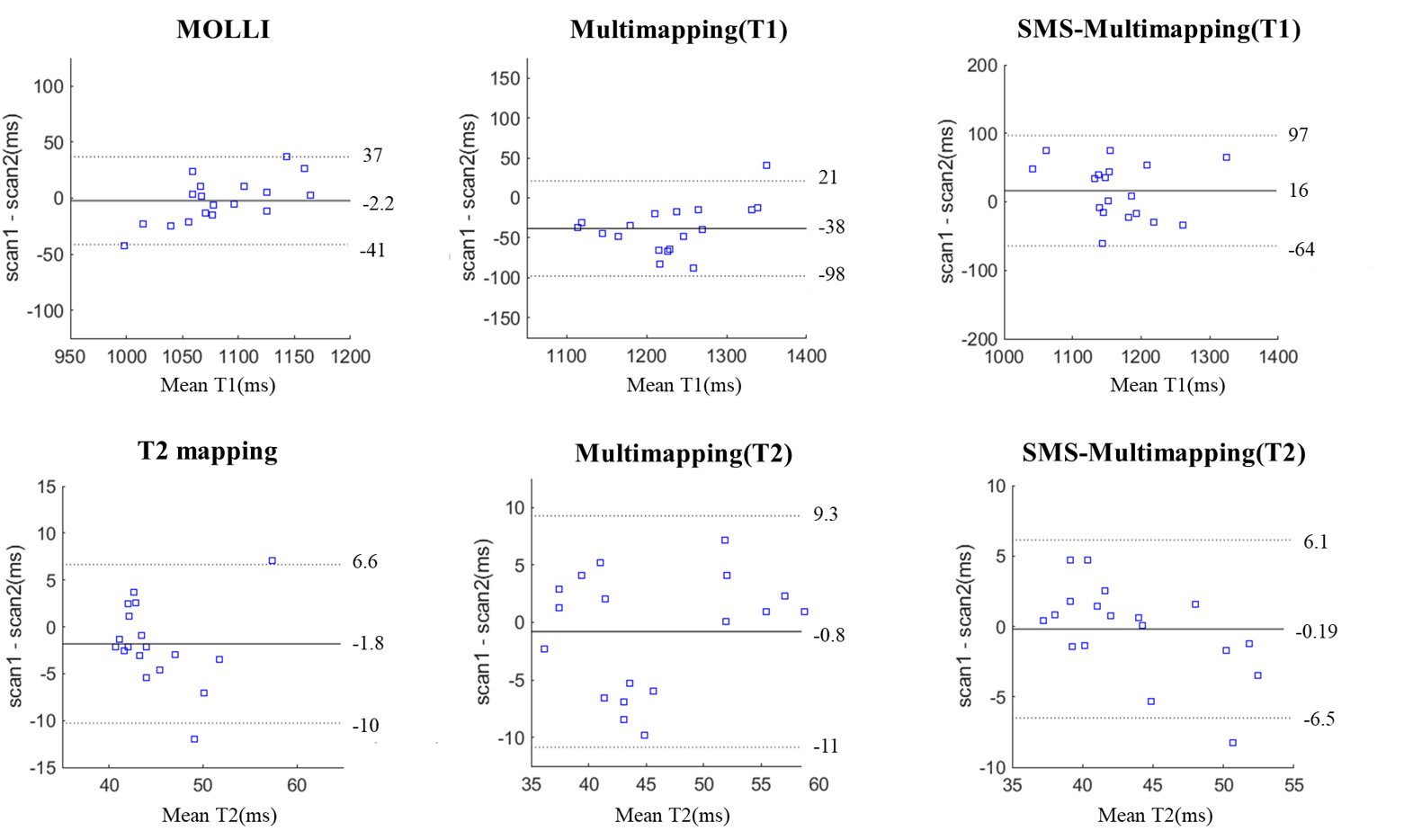
Fig. 5 shows preliminary evaluations of the regional T1/T2 scan-rescan reproducibility in 3 subjects. The regional T2 of SMS-Multimapping appeared very reproducible, while the regional T1 of SMS-Multimapping appeared less reproducible than the other methods.
Discussion and Conclusions
SMS-Multimapping is able to fulfill simultaneous 3-slice T1 and T2 mapping in 10 heartbeats, which is a reasonable time for a single breath-hold. The proposed LLRS reconstruction well mitigated the noise and artifacts caused by the acceleration. The regional T1 and T2 measured by SMS-Multimapping showed good accuracy, albeit the precision and reproducibility appeared slightly lower than MOLLI/T2 mapping, potentially due to the inherent lower SNR of the FLASH readout and the large acceleration rate. The 6-fold reduction of scan time could greatly improve patient comfort and make parametric mapping more feasible for severely ill patients in clinical practice.Acknowledgements
No Acknowledgements found.References
1. Taylor AJ, Salerno M, Dharmakumar R, Jerosch-Herold M. T1 Mapping: Basic Techniques and Clinical Applications. JACC Cardiovasc Imaging. 2016;9(1):67-81. doi:10.1016/j.jcmg.2015.11.005
2. Kellman P, Aletras AH, Mancini C, McVeigh ER, Arai AE. T2-Prepared SSFP Improves Diagnostic Confidence in Edema Imaging in Acute Myocardial Infarction Compared to Turbo Spin Echo. Magn Reson Med. 2007;57(5):891-897. doi:10.1002/mrm.21215
3. Kellman P, Wilson JR, Xue H, Ugander M, Arai AE. Extracellular volume fraction mapping in the myocardium, part 1: evaluation of an automated method. J Cardiovasc Magn Reson. 2012;14(1):63. doi:10.1186/1532-429X-14-63
4. Henningsson M. Cartesian dictionary-based native T1 and T2 mapping of the myocardium. Magn Reson Med. 2022;87(5):2347-2362. doi:10.1002/mrm.29143
5. Barth M, Breuer F, Koopmans PJ, Norris DG, Poser BA. Simultaneous multislice (SMS) imaging techniques. Magn Reson Med. 2016;75(1):63-81. doi:10.1002/mrm.25897
6. Weingärtner S, Moeller S, Schmitter S, et al. Simultaneous multislice imaging for native myocardial T1 mapping: Improved spatial coverage in a single breath-hold. Magn Reson Med. 2017;78(2):462-471. doi:10.1002/mrm.26770
7. Ye H, Cauley SF, Gagoski B, et al. Simultaneous multislice magnetic resonance fingerprinting (SMS-MRF) with direct-spiral slice-GRAPPA (ds-SG) reconstruction. Magn Reson Med. 2017;77(5):1966-1974. doi:10.1002/mrm.26271
8. Hilbert T, Schulz J, Marques JP, et al. Fast model-based T2 mapping using SAR-reduced simultaneous multislice excitation. Magn Reson Med. 2019;82(6):2090-2103. doi:10.1002/mrm.27890
9. Gaspar AS, Silva NA, Price AN, Ferreira AM, Nunes RG. Open-source myocardial T1 mapping with simultaneous multi-slice acceleration: Combining an auto-calibrated blipped-bSSFP readout with VERSE-MB pulses. Magn Reson Med. April 2023. doi:10.1002/mrm.29661
10. Zhang T, Pauly JM, Levesque IR. Accelerating parameter mapping with a locally low rank constraint: Locally Low Rank Parameter Mapping. Magn Reson Med. 2015;73(2):655-661. doi:10.1002/mrm.25161
11. Mao X, Lee HL, Hu Z, et al. Simultaneous Multi-Slice Cardiac MR Multitasking for Motion-Resolved, Non-ECG, Free-Breathing T1–T2 Mapping. Front Cardiovasc Med. 2022;9:833257. doi:10.3389/fcvm.2022.833257
12. Hamilton JI, Jiang Y, Ma D, et al. Simultaneous multislice cardiac magnetic resonance fingerprinting using low rank reconstruction. NMR Biomed. 2019;32(2):e4041. doi:10.1002/nbm.4041
13. Wang X, Rosenzweig S, Scholand N, Holme HCM, Uecker M. Model-based reconstruction for simultaneous multi-slice mapping using single-shot inversion-recovery radial FLASH. Magnetic Resonance in Medicine. 2021;85(3):1258-1271. doi:10.1002/mrm.28497
14. Yang F, Zhang J, Li G, Zhu J, Tang X, Hu C. Regularized SUPER-CAIPIRINHA: Accelerating 3D variable flip-angle T1 mapping with accurate and efficient reconstruction. Magn Reson Med. 2023;90(4):1380-1395. doi:10.1002/mrm.29714
15. Boyd S. ADMM. FNT in Machine Learning. 2010;3(1):1-122. doi:10.1561/2200000016
Figures