4561
Quantitative multi-dimensional assessment of cardiovascular system (qMACS)1Department of Radiology, University of Southern California, Los Angeles, CA, United States, 2University of Southern California, Los Angeles, CA, United States, 3Department of Radiological Sciences, University of California, Los Angeles, CA, United States, 4Biomedical Imaging Research Institute, Cedars-Sinai Medical Center, Los Angeles, CA, United States
Synopsis
Keywords: Quantitative Imaging, Quantitative Imaging, free‐breathing, ECG-free, multi-contrast
Motivation: A recently developed MACS technique provides exquisite delineation of the structure and motion of the whole heart and aorta. However, it lacks T1, T2 information and is limited in assessing complex vascular and myocardial pathologies.
Goal(s): To develop a quantitative MACS (qMACS) technique by incorporating T1 and T2 mapping into original MACS imaging pipeline.
Approach: The qMACS sequence builds on a multi-tasking imaging framework and stack-of-stars acquisition. Respiratory-resolved T1,T2 maps were generated using dictionary-matching approach.
Results: Free‐breathing and ECG-free 3D quantitative imaging of cardiovascular system in 10 minutes is feasible by proposed qMACS. qMACS measured slightly higher myocardial T1/T2 values than reference methods.
Impact: qMACS is a time-efficient and patient-friendly technique for both quantitative and qualitative imaging of the whole cardioaortic system and may be used as a gatekeeper approach to the diagnosis of a variety of cardiovascular diseases.
Introduction
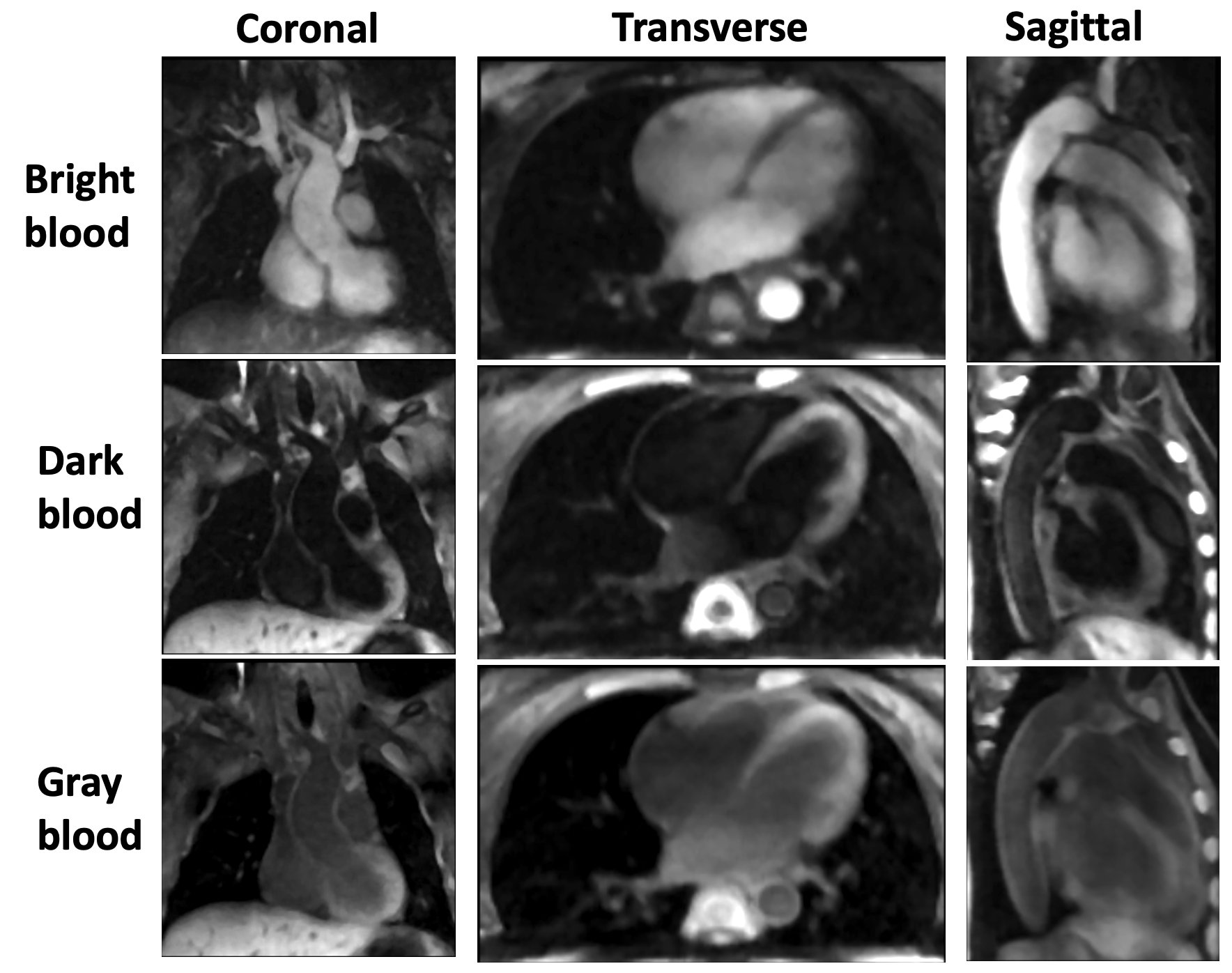
Imaging assessment of the cardiac and aortic structure and function is a key component for diagnosis, risk stratification, and procedural planning in patients with cardiovascular diseases. Our previous work presents an MR Multitasking1 based 3D multi-dimensional assessment of cardiovascular system (MACS) technique to provide multi-contrast, cardiac phase-resolved imaging of the whole heart and thoracic aorta in a single scan without the need for ECG triggering or respiratory navigation2,3. However, MACS cannot provide T1 and T2 information and is thus limited in assessing complex vascular and myocardial pathologies. In this work a quantitative MACS (qMACS) technique was developed to produce T1, T2 maps and co-registered images of bright blood (BB), dark blood (DB), gray blood (GB) images and in single 10-minute free-breathing and ECG-free scan.Methods
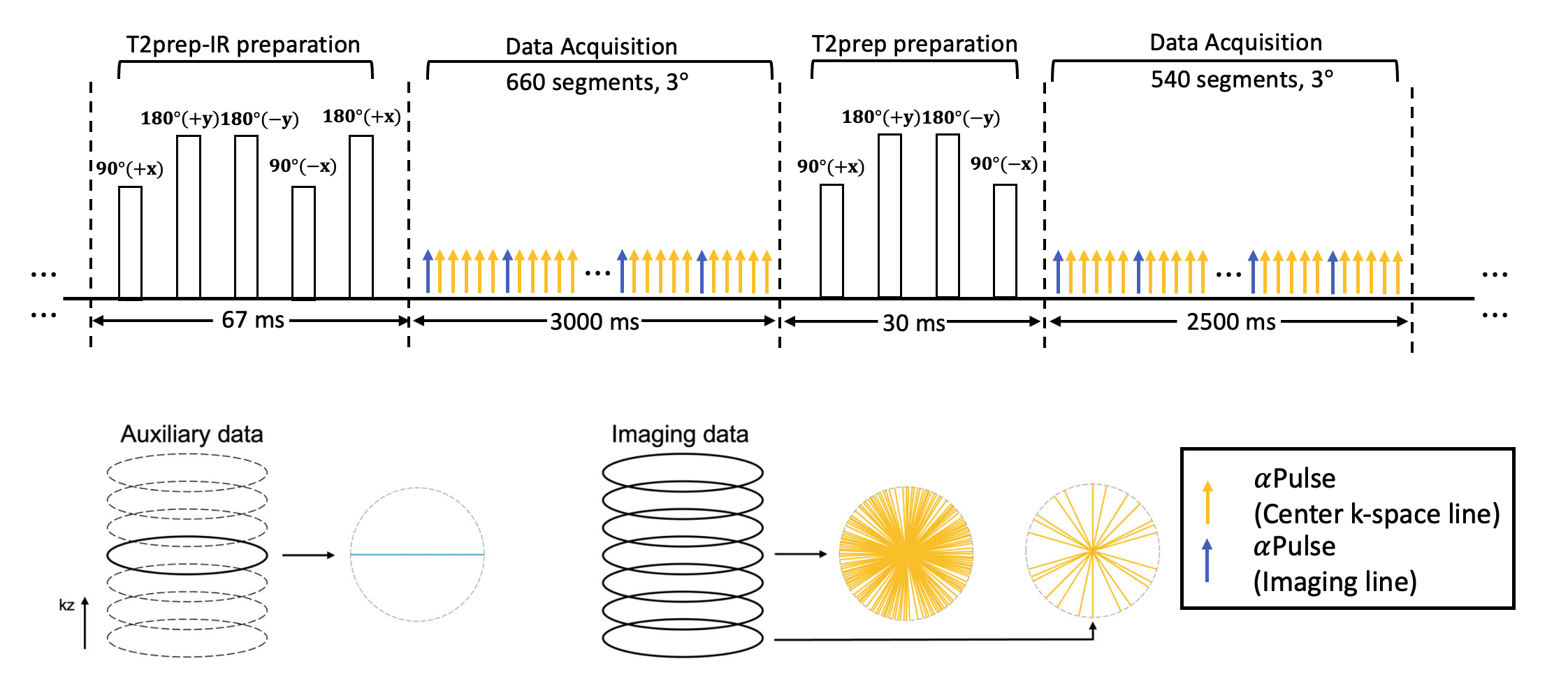
Sequence design and reconstruction: The proposed technique was implemented based on continuous FLASH readouts with tiny-golden-angle (Ψ=32.039°) stack-of-stars k-space sampling. T2-prepared inversion recovery (T2IR) preparation and T2 preparations are combined to generate T1/T2-weighted signals during magnetization evolution. Following each preparation module, RF pulse flip angles are 3° and segments are 660 for T2IR and 540 for T2-prep. Subspace auxiliary data are interleaved with imaging data every six segments and are collected at the 0° radial spoke of the center partition (Fig 1). qMACS adopts a low-rank tensor image model for 6D imaging, with three spatial dimensions for volumetric imaging, one cardiac motion dimension for cine imaging, one respiratory motion dimension for free-breathing imaging, one T2IR/T2 time dimension for multi-contrast assessment.Data Collection: The phantom study was performed on a standard Calimetrix phantom (Calimetrix, Madison, WI). Five human volunteers (31.6±6 yrs) were imaged on a 3T scanner (Siemens) with a standard 18-channel body coil and a 32-channel spinal coil. qMACS parameters were: FOV = 224 × 224 × 162.4 mm3, TR/TE=4.5ms/2.1ms, water excitation, recovery period=3s, T2 preparation duration = 67/30ms, spatial resolution = 1.4x1.4x2.8 mm3, total scan time = 9:54min. Reference 2D T1 maps with MOLLI (1.4x1.4x8.0 mm3) and 2D T2 maps with T2-prep FLASH (1.4x1.4x8.0 mm3) were acquired in 3 slices during end-expiration breath-holds.
Parameter mapping: All T1/T2 maps were fit together using a dictionary matching approach to the signal evolution based on Bloch simulations, on a voxel-by-voxel basis. The dictionary was simulated with instantaneous RF pulses and included the dummy repetitions used to reach steady state. In addition, the dictionary included an estimate of correction term B0 and B1 inhomogeneity.
Results
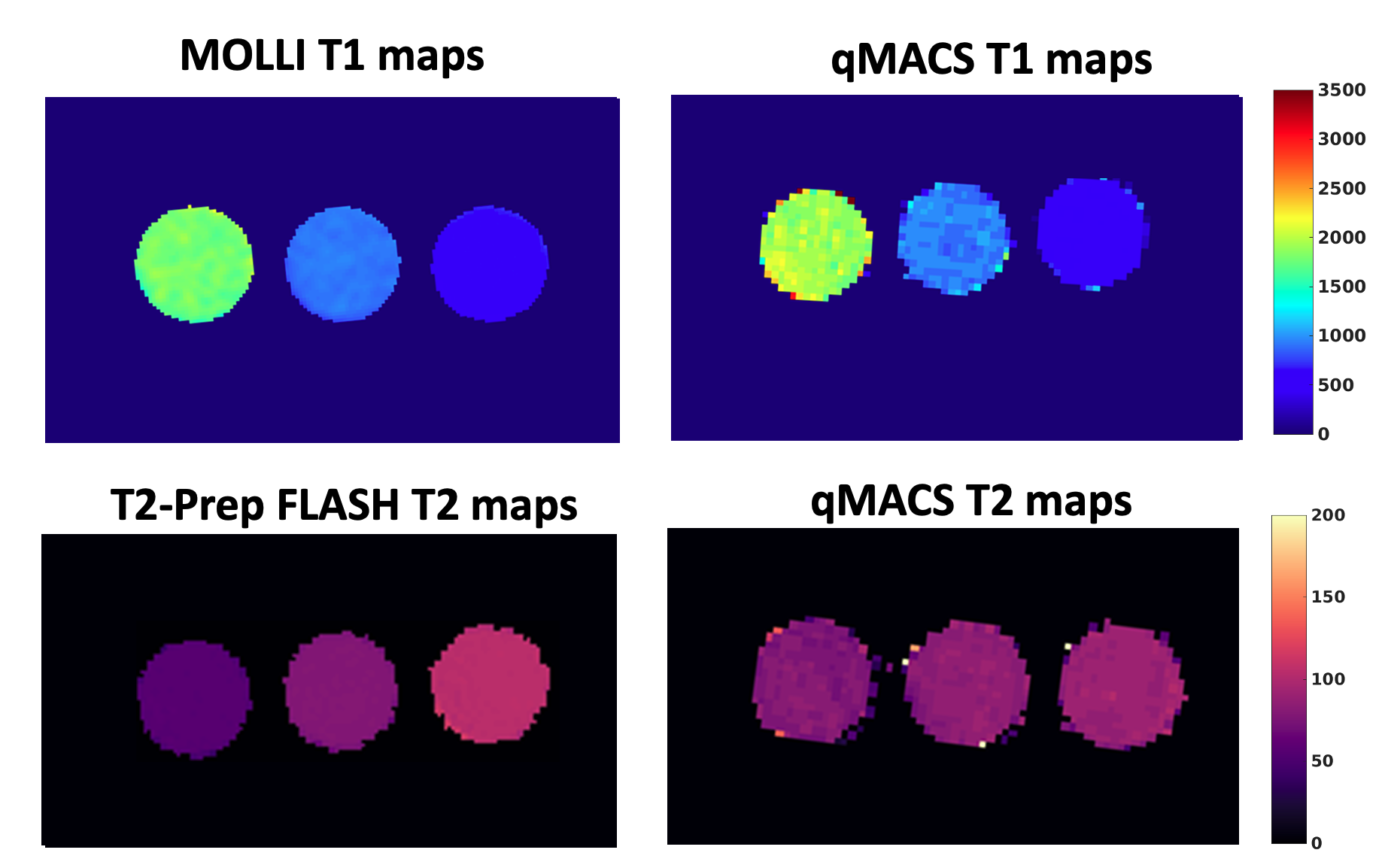
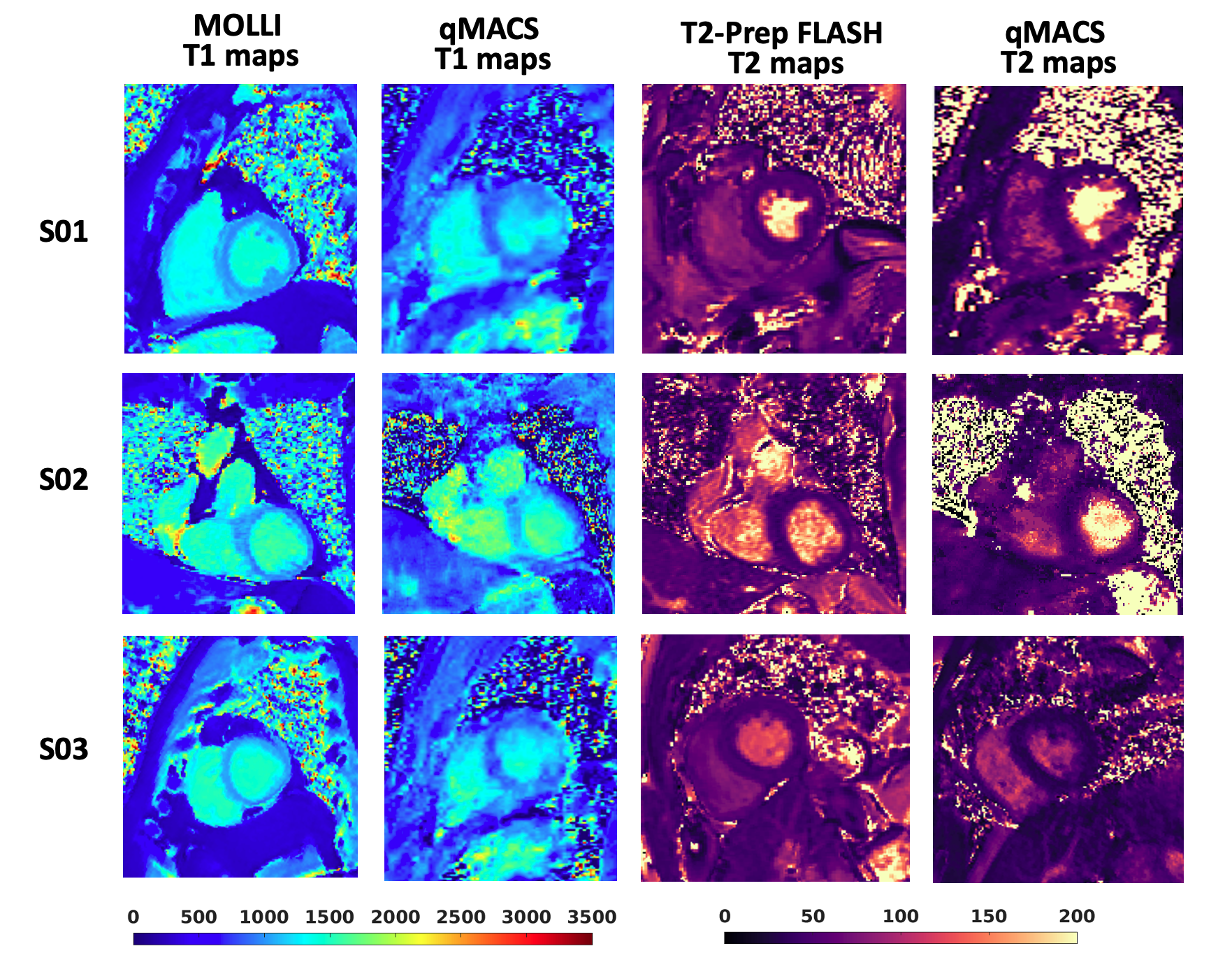
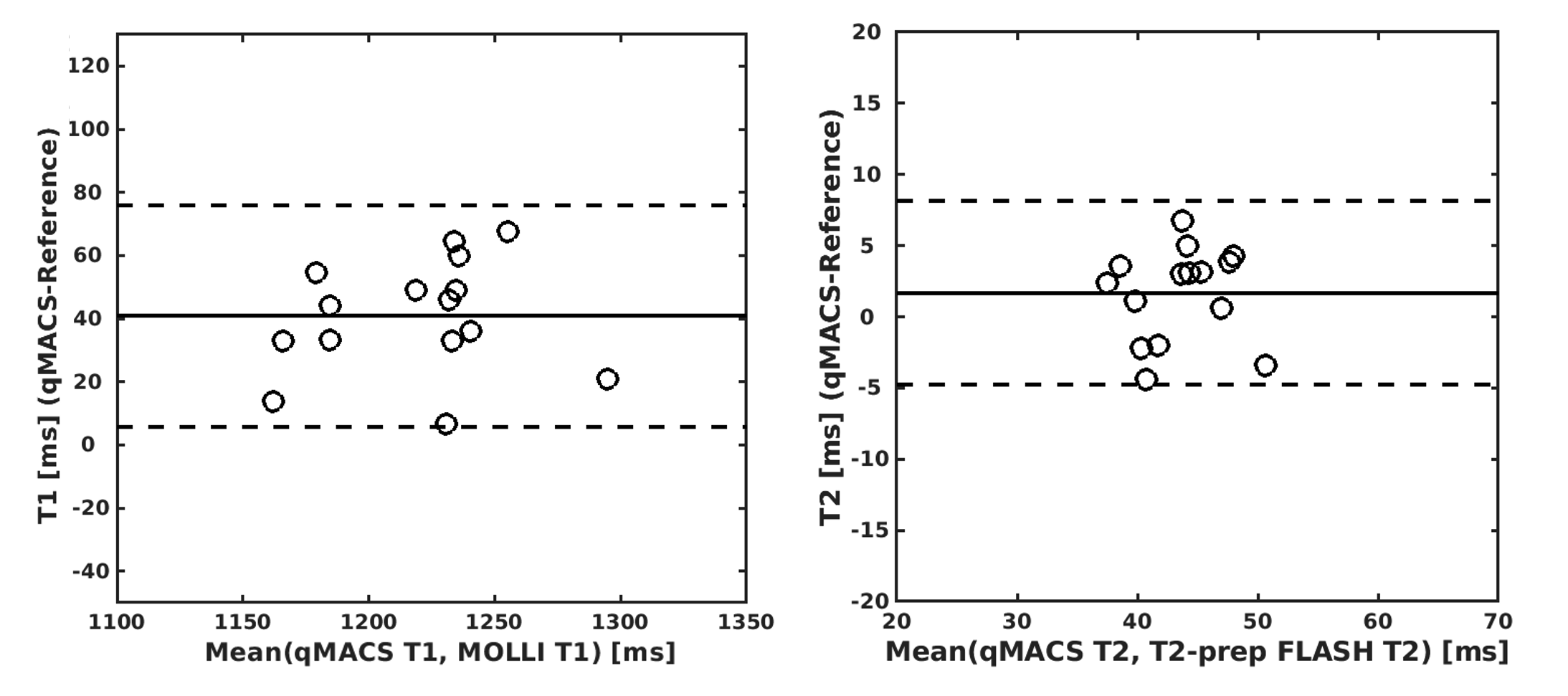
Representative cases with multi-contrast (BB, DB, GB) are shown in figure 2. Figure 3 displays the T1/T2 maps of the Calimetrix phantom generated by qMACS and reference sequences, respectively. The mean difference between the two methods was 5.6% for T1 and 4.7% for T2. T1/T2 mapping results from 3 healthy subjects are shown in Fig. 4. Figs. 5 depicts the summary statistics for segment-wise T1/T2 values. qMACS yielded higher myocardial T1 values (1284±163.7ms) than MOLLI (1198± 36.5ms), and higher myocardial T2 values (44.3±6.7ms) than the T2-prep FLASH method (42.2±5.3ms), which is still within the normal range reported by some studies4,5.Discussion
qMACS is a single-scan, free-breathing MRI technique allowing multi-contrast qualitative and quantitative imaging of the cardiovascular system. A traditional cardiac exam including structural and cardiac function imaging requires breath-holds and a total exam duration of approximately 30 minutes. The qMACS technique has notably condensed the overall exam time to a mere 10 minutes, all while allowing for free breathing and obviating the need for ECG synchronization. Additionally, the proposed approach ensures that all images and maps are co-registered, which could streamline the post-processing steps. This technique, owing to its flexible image contrast and quantitative nature, would potentially be valuable for early detection and severity assessment of cardiovascular diseases. Future initiatives aim to further refine this method by improving the sharpness of map images, verify repeatability and robustness, enhancing spatial resolution to mitigate partial volume effects.Conclusion
This work demonstrates the feasibility of the free‐breathing and ECG-free multi-contrast qualitative and quantitative imaging of the cardiovascular system in 10 minutes. Larger patient cohorts including diverse cardiovascular diseases are warranted for further refinement and validation.Acknowledgements
No acknowledgement found.References
1. Christodoulou, A. G., Shaw, J. L., Nguyen, C., Yang, Q., Xie, Y., Wang, N., & Li, D. (2018). Magnetic resonance multitasking for motionresolved quantitative cardiovascular imaging. Nature BME, 2(4), 215-226.
2. Hu, Z., Christodoulou, A.G., Wang, N., Shaw, J.L., Song, S.S., Maya, M.M., Ishimori, M.L., Forbess, L.J., Xiao, J., Bi, X. and Han, F., 2020. Magnetic resonance multitasking for multidimensional assessment of cardiovascular system: Development and feasibility study on the thoracic aorta. Magnetic resonance in medicine, 84(5), pp.2376-2388.
3. Hu, Z., Xiao, J., Mao, X., Xie, Y., Kwan, A.C., Song, S.S., Fong, M.W., Wilcox, A.G., Li, D., Christodoulou, A.G. and Fan, Z., 2023. MR Multitasking‐based multi‐dimensional assessment of cardiovascular system (MT‐MACS) with extended spatial coverage and water‐fat separation. Magnetic Resonance in Medicine, 89(4), pp.1496-1505.
4. Snel, G. J. H., Van Den Boomen, M., Hernandez, L. M., Nguyen, C. T., Sosnovik, D. E., Velthuis, B. K., ... & Prakken, N. H. J. (2020). Cardiovascular magnetic resonance native T2 and T2* quantitative values for cardiomyopathies and heart transplantations: a systematic review and meta-analysis. J Cardiovasc Magn Reson, 22, 1-34.
5. An, D. A., Chen, B. H., Shi, R. Y., Bu, J., Ge, H., Hu, J., ... & Wu, L. M. (2018). Diagnostic performance of intravoxel incoherent motion di usion-weighted imaging in the assessment of the dynamic status of myocardial perfusion. J Magn Reson Imaging, 48(6), 1602-1609.
Figures