4554
Comparative Analysis of Cardiac T1 Mapping Reliability: Free-Breathing Versus Breath-Hold Techniques1University of Wisconsin - Madison, Madison, WI, United States
Synopsis
Keywords: Quantitative Imaging, Myocardium, T1 Mapping, Repeatability
Motivation: Quantitative myocardial T1 mapping is an invaluable tool for detection and characterization of myocardial fibrosis and infarction. Recent emergence of free-breathing non-ECG-gated techniques requires evaluation of their reliability in controlled experiments.
Goal(s): We evaluated repeatability of free-breathing non-ECG-gated Multitasking and breath-held MOLLI T1 mapping techniques and studied factors influencing them.
Approach: Test-retest study was performed in 15 healthy adult volunteers. Bland-Altman plots and Spearman rank correlation were used for statistical analysis.
Results: Our analysis reveals that while free-breathing technique has low bias, controlling data sampling patterns is needed to prevent high variability of test-retest measurements.
Impact: Reliability of myocardial T1 mapping with free-breathing techniques may benefit from designing controlled data sampling patterns utilizing either external or self-calibrated cardiac/respiratory triggers.
Introduction
Quantitative myocardial T1 mapping is an invaluable tool for detection and characterization of myocardial fibrosis and infarction. The standard approach is to acquire data within one breath-hold period using ECG-triggering and single-shot imaging to produce T1 maps without cardiac and respiratory blurring1, although at the expense of spatial resolution and limited applicability in subjects who cannot hold their breath long enough. The free-breathing cardiac T1 mapping without ECG gating has a potential to enable longer scan times to improve spatial coverage and/or resolution. One such promising technique is a Multitasking algorithm2 that targets relatively short free-breathing T1 mapping. It relies on interleaved acquisition of calibration lines to learn respiratory and cardiac data binning and temporal bases to guide low-rank data reconstruction. Evaluation of such methods is challenging given numerous intricate steps in data acquisition and processing3. In this work, we investigate and evaluate the method through a reductionist lens, in which performance of self-calibrated data binning and inherent data were controlled using external monitoring of cardiac and respiratory phases and extended acquisition times, thereby allowing independent evaluation of the sampling pattern and reconstruction characteristics of the Multitasking approach.Methods
Data Acquisition: 2D free-breathing, ECG-free, IR-prepped Golden-angle radial MRI technique with dual flip angle (FA) Multitasking acquisition scheme for B1+ corrected myocardial T1 mapping [1] was implemented for the study (FOV=360mm×360mm, Xres=528 , FAs=3o/10o, BW=125kHz, TR/TE=4.7/1.9ms, scan time 420 sec). 377 pairs of unique golden and fixed (calibration) angle projections were acquired during each IR pulse. MOLLI1 was chosen as the standard breath-hold method (FOV=360mm×324mm, BW=111kHz, TR/TE=3.0/1.2ms, acquisition matrix=160×120, flip angle=35o, TI=129ms). ECG and respiratory signals were recorded for Multitasking acquisition using 4-lead ECG and respiratory bellows, respectively. MOLLI scans were performed at end-expiration and end-diastole.Subject Population: 15 healthy adult subjects were enrolled in the study (in accordance with the IRB). Each subject was imaged at a 3T system (Premier, GE Healthcare, Waukesha, WI) with both sequences. The scans were repeated after the subject was removed from the scanner and repositioned.
Data Processing and Analysis: Mean T1 values were estimated in the myocardium ROIs. Given the availability of multiple phases in Multitasking and independence of their sampling patterns, the analysis was performed using measurements from systolic and diastolic periods. Multitasking data from three subjects were excluded from the repeatability analysis due to the failure of reconstruction to yield clinically useful images. Bland-Altman plots were used for assessment of repeatability of individual techniques.
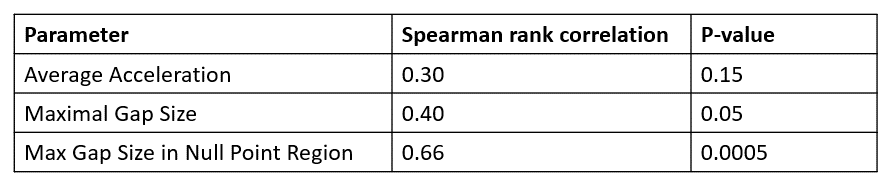
Our hypothesis is that the parameters of the sampling pattern resulting from free breathing may be the major determinants of the image quality and, hence, repeatability. We tested the associations of the test/retest differences with the following parameters for each four-tuple (2 FAs for test/retest) of sampling patterns: (1) overall acceleration; (2) maximum gap (number of consecutively unsampled inversion times); (3) maximum gap in sampling the initial IR curve (i.e., within the vicinity of null-point, first 20% of total inversion times) that is most critical for the performance of T1 mapping. The measures were compared using non-parametric Spearman rank correlations.
Results
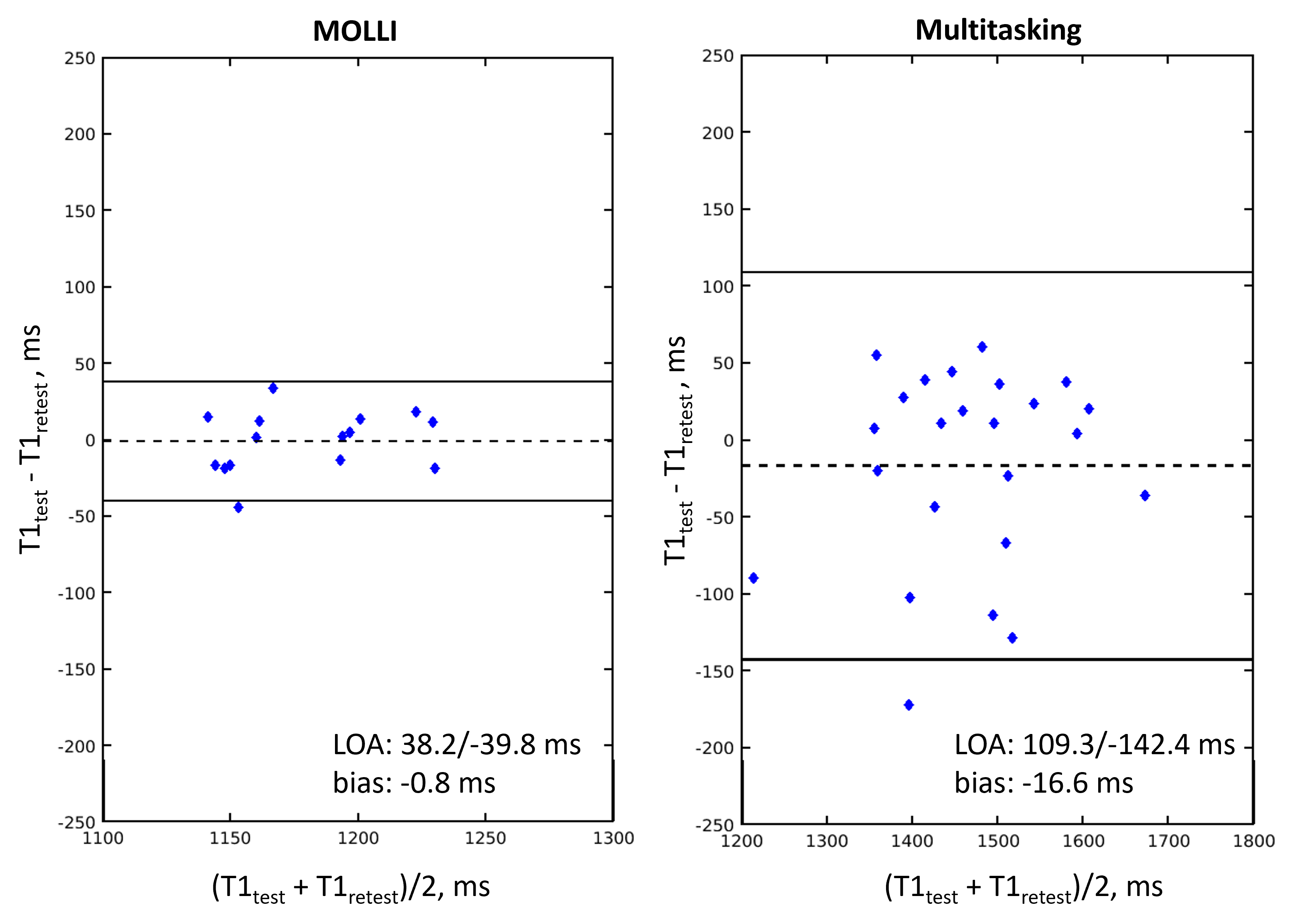
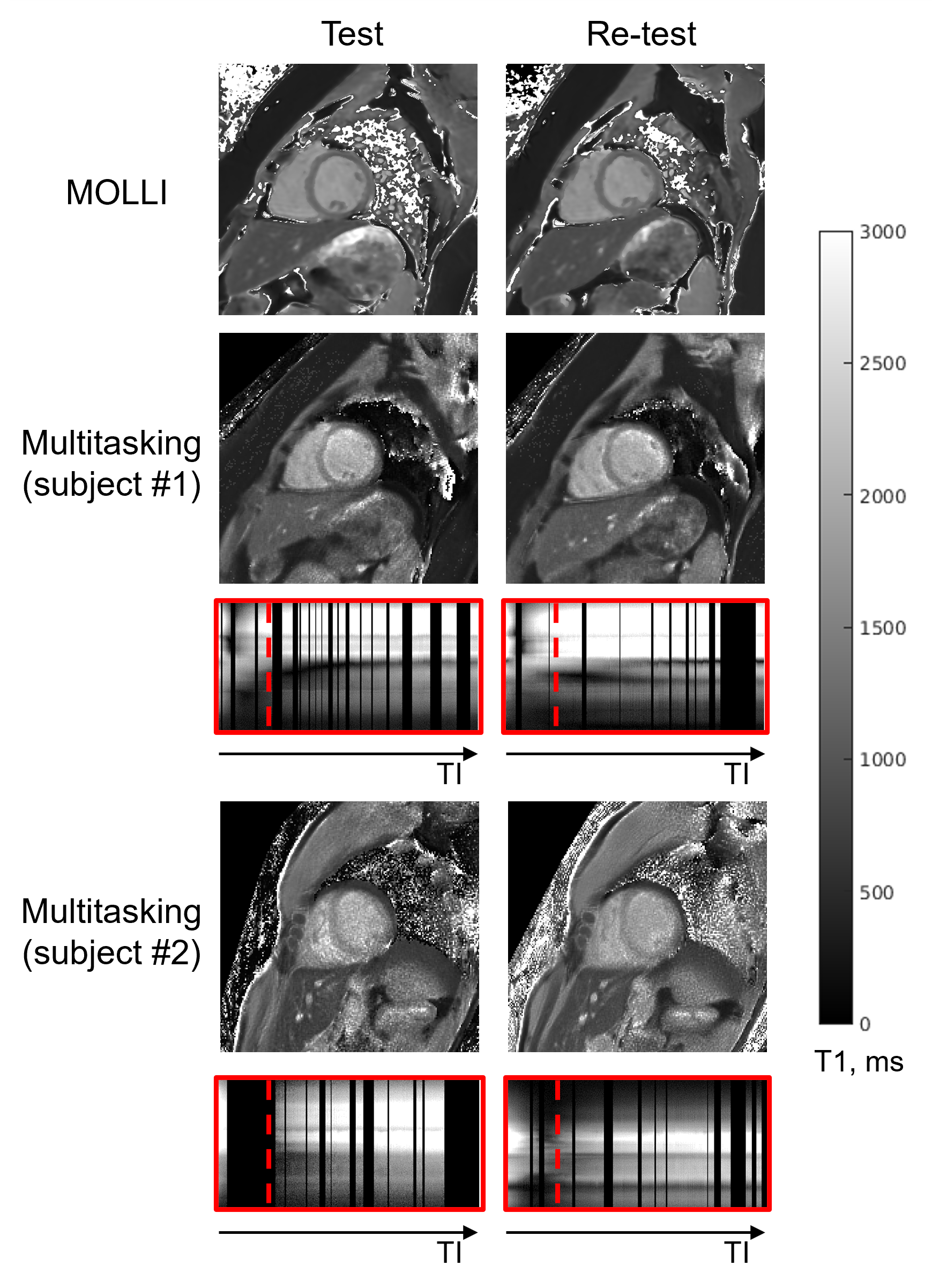
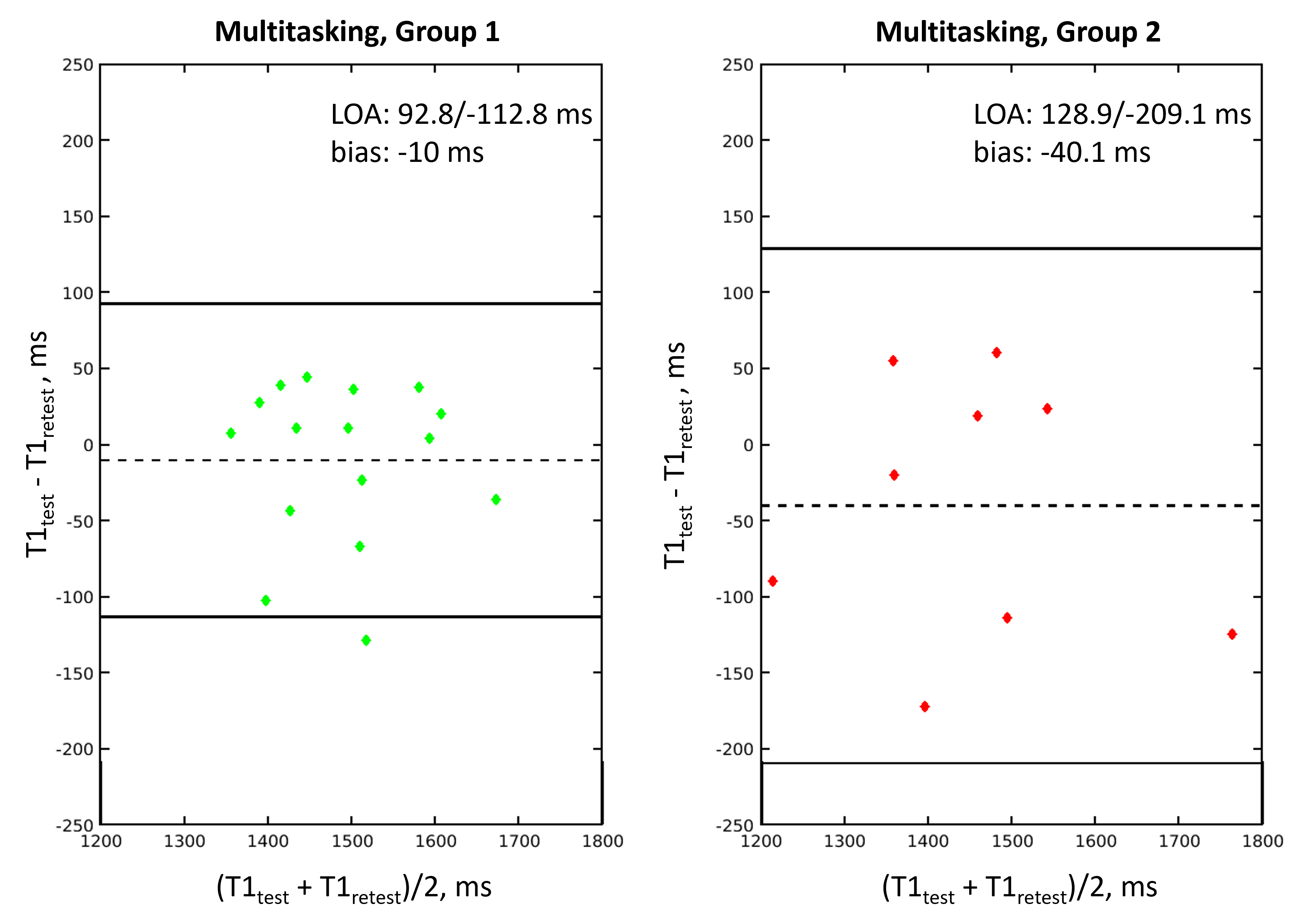
Figure 1 illustrates the repeatability of the techniques. MOLLI resulted in lower bias and higher repeatability (3.2x) compared to the free-breathing technique. Figure 2 shows representative T1 maps from MOLLI and Multitasking. Note the reduced consistency of T1 mapping with the latter in case of suboptimal sampling patterns due to free breathing (Subject 2). Table 1 confirms that the gaps of unsampled data in the null-point area are the best determinants of the performance of the free-breathing technique, supporting the hypothesis that poor sampling of the initial IR curve is the most likely source of insufficient stability and repeatability of Multitasking T1 mapping. To further evaluate the idea, we performed Bland-Altman analysis separately for the cases stratified into two groups according to this parameter (Fig. 3): Group 1 has maximal critical gap size not exceeding 10, the rest are Group 2.Discussion and Conclusions
Both free-breathing and breath-hold techniques are characterized by sufficiently low bias based on the averaged test-retest results. However, the limits of agreements indicate high variability of the free breathing technique potentially jeopardizing its utility to characterize myocardial T1 changes. Our analysis revealed that the most probable reason for such instability is the possibility of high irregularity of the sampling pattern of the inversion curve inherent to the free-breathing paradigm that does not guarantee consistent sampling with controlled gaps of missing data. These results suggest that controlling data sampling patterns utilizing either external or self-calibrated cardiac/respiratory triggers may be more viable options for consistent myocardial T1 mapping.Acknowledgements
The authors thank GE Healthcare for the research support.
References
1. Messroghli DR, Radjenovic A, Kozerke S, Higgins DM, Sivananthan MU, and Ridgway JP. Modified Look-Locker inversion recovery (MOLLI) for high resolution T1 mapping of the heart. MRM 2004; 52:141
2. Serry FM, Ma S, Mao X, Han F, Xie Y, Han H, Li D, Christodoulou AG. Dual flip-angle IR-FLASH with spin history mapping for B1+ corrected T1 mapping: Application to T1 cardiovascular magnetic resonance Multitasking. MRM 2021; 86:3182.
3. Mao X, Lee HL, Hu Z, Cao T, Han F, Ma S, Serry FM, Fan Z, Xie Y, Li D, Christodoulou AG, Simultaneous Multi-Slice Cardiac MR Multitasking for Motion-Resolved, Non-ECG, Free-Breathing T1–T2 Mapping, Frontiers in Cardiovascular Medicine, 9(2022)
Figures