4531
Whole body imaging at 3T with multi-coil array and compressed sensing for metastasis screening with cryo-fluorescence tomography validation.1Radiology, New York University School of Medicine, New York, NY, United States, 2Pathology, New York University School of Medicine, New York, NY, United States
Synopsis
Keywords: Biology, Models, Methods, Whole Body, compressed sensing; metastasis; fluorescence tomography
Motivation: Cancer metastasis involves multiple organs and traditional bioluminescent imaging lacks spatial resolution to locate metastatic foci. New MRI imaging protocols need to be developed to image metastasis distribution over the whole mouse body.
Goal(s):
- Acquire high resolution 3D volumes in an acceptable time frame.
- Validate findings using cryo-fluorescence tomography (CFT).
Approach:
- An 8-channel array coil was used to acquire whole body isotropic volumes with compressed sensing.
- Post imaging CFT datasets were acquired for validation.
Results:
- High contrast volumes of mouse body were acquired at 200x200x200 μm in 16 minutes.
- Liver metastatic foci observed.
- Correspondence of mouse anatomy with MRI and CFT achieved.
Impact: Whole body imaging with 8-channel array coil permits longitudinal visualization of major organs in normal and diseased states. Compressed sensing optimizes workflow for high throughput screening, and Cryo-Fluorescence tomography can then be used as gold standard for validation of MRI.
Introduction
Metastasis is a complex process in which cancerous cells can invade one or more organs [1], [2]. Recent advances in high throughput induction of cancer metastasis models using ultrasound guided intra-cardiac injections has shown to be efficient at metastasizing to organs such as the heart, liver, lungs, kidneys, spleen and pancreas [3]. To assess the extent to which the metastatic burden evolves over time the cells are normally labeled with bioluminescent reporters [2] and the progression of the metastasis followed using bioluminescent imaging. This type of imaging does not give the precise location of the metastatic foci. MRI can play a key role in assessing non invasively and longitudinally the metastatic burden across organs. For efficient imaging of such a high cohort of mice an efficient imaging protocol has been developed taking advantage of modern preclinical MRI methods such as parallel imaging and compressed sensing (CS) [4] in conjunction with array body coils to assess the whole mouse body. Cryo-fluorescence tomography data will be used as a gold standard validation tool.Methods
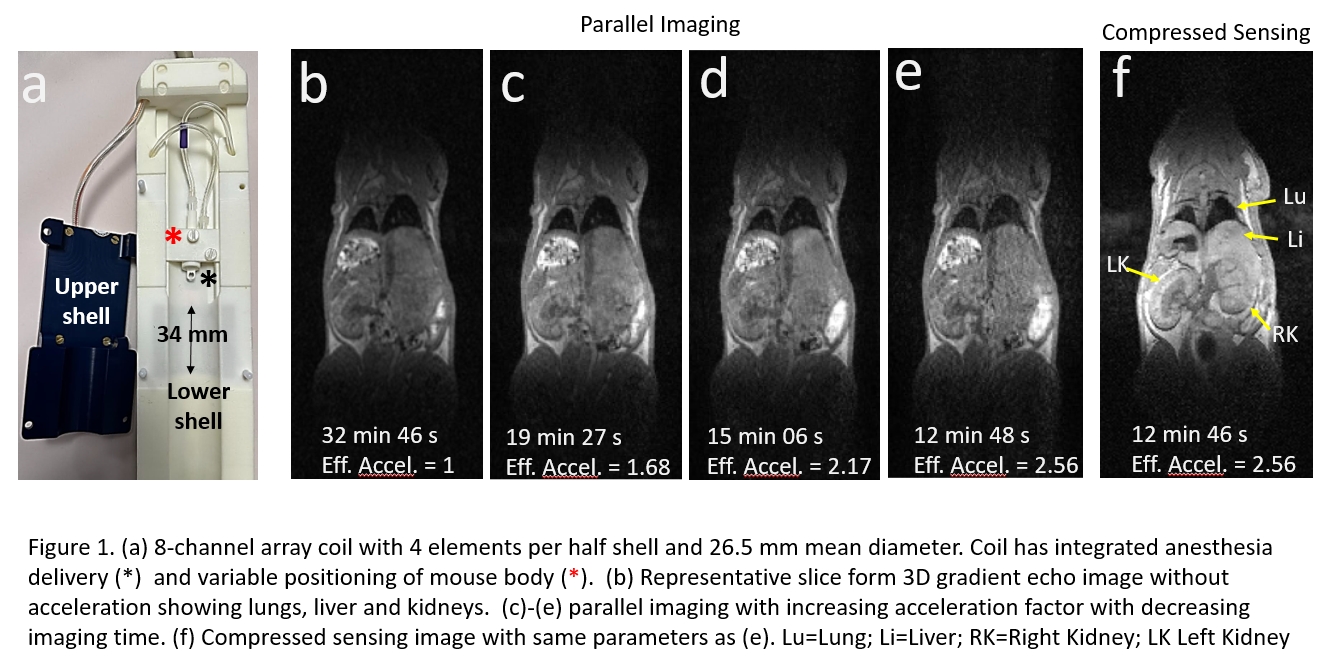
Mouse models: Induction of metastatic lesions was accomplished using high frequency ultrasound image guidance injections (IC) [2] of human melanoma cancer cells into the left ventricle of NSG immune-deficient mice.MRI imaging protocol: All experiments were performed on a 3-Tesla Bruker Biospec 7030 scanner interfaced to an Avance-3HD console running under Paravision 360 v3.3. An 8-channel array coil (Fig1a) was used to acquire in vivo 3D images of the mouse body. The array consists of an upper and a lower shell each half consists of 4 overlapping elements with a 34 mm in length formed in a circular pattern with a diameter which ranges from 24 to 29 mm. Gradient echo images where acquired with FA=15o, TR= 10ms, TE=2.2ms, BW=100kHz, NAv=12, 300μm isotropic resolution.
Cryo-Fluorescence tomography (CFT): Mouse bright field images where acquired from a Xerra CFT (Emit Imaging). A Whole frozen mouse was embedded in OCT and a blade shaves off 45 μm of material and a bright field image of the block face is acquired 45 μm isotropic resolution.
Results
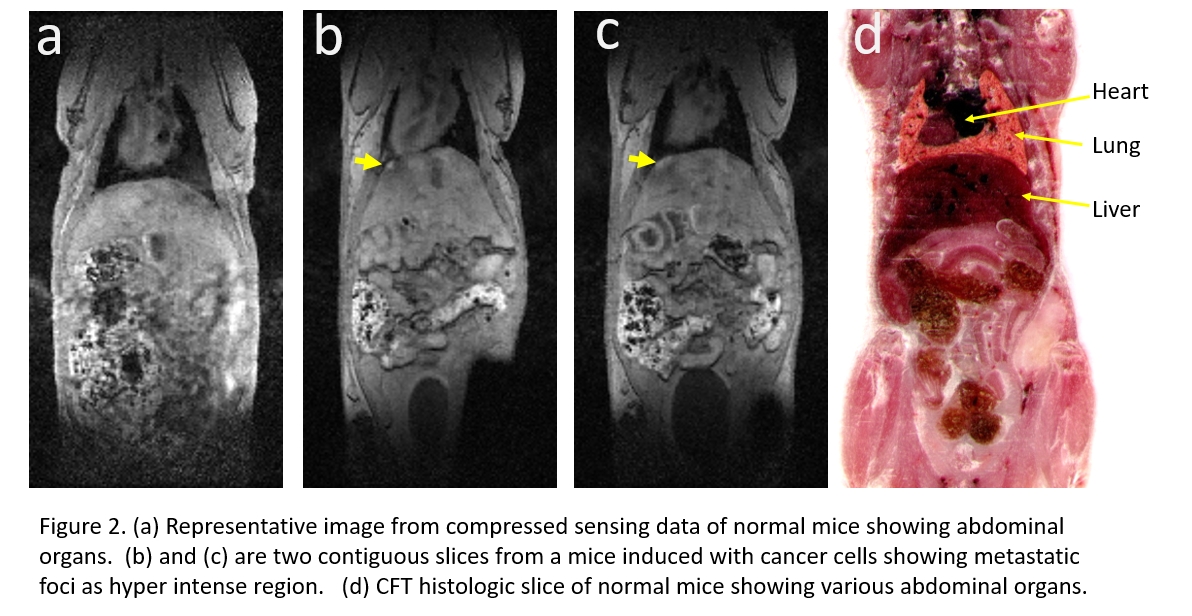
As shown in figure 1, the array coil has adequate coverage to image the major abdominal organs from the heart to well below the kidneys but with low contrast between the organs except for the lungs (Fig1b). By increasing the acceleration times in the parallel imaging protocol the acquisition time was reduced from 32 to 12 minutes (Fig1 c-e) but with further loss in image quality. To compare to parallel imaging 3D data was also acquired using compressed sensing by keeping all acquisition parameters with under sampling set at 39 % and the center ratio parameter set to 10%. At equal imaging times of less than 13 minutes at 300 μm resolution the CS image (Fig 1f) has superior image quality than the parallel receive imaging with acceleration factor of x2.56. Importantly the abdominal organs acquired at 12 minutes using the CS are clearly defined compared to the a non accelerated (Fig 1b) data acquired at 32 minutes.The parameters for the compressed sensing algorithm where further optimized to acquire 200 um isotropic resolution images in under 16 minutes (Fig 2a). Figure 2b and 2c are two contiguous slices showing a metastatic foci developed in the liver of a mice induced with cancer cells eight days post induction. The image sensitivity is high enough to capture metastatic events at time points earlier than expected.
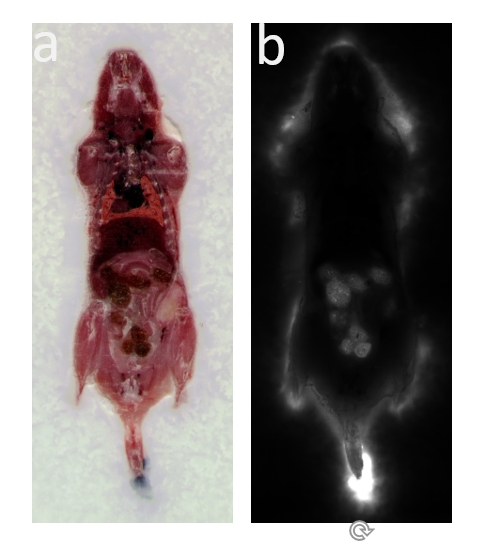
The CFT image (Fig 2d) shows an accurate whole mouse histological registration of the anatomical structures to the MRI images. Figure 3 shows a fluorescent image where the region near the liver and lungs have emit no auto fluorescence signal signal at these wavelengths.
Discussion and conclusion
Preclinical MRI imaging is routinely done at field strengths of 7T or greater. This work shows that the loss of sensitivity at 3T can be compensated by combining phased array coils with parallel image acceleration and compressed sensing. From the results CS seems to be the more sensitive method to image the abdomen at 200 μm isotropic resolution in 16 minutes. In the future the variable positioning of the mouse will be used to acquire several overlapping volumes and the stitch them together in post processing to acquired the whole mouse body. Future work will also involve injecting cells which also express fluorescent reporters so that the metastatic foci imaged with MRI can be validated with the CFT. From figure 3 metastatic cells which will be tagged with GFP reporter will easily be detected in the major organs of the mouse.Acknowledgements
This work was performed at the Preclinical imaging core; a shared resource partially supported by the NYUCI Center Support Grant, “NIH/NCI5P30CA016087”, the NIBIB Biomedical Technology Resource Center (NIH P41 EB017183) and by NIH grant UL1 TR00038 from the National Center for Advancing Translational Sciences (NCATS). NIH PPG 1P01HL131481References
[1] Morsi A, Gaziel-Sovran A, Cruz-Munoz W, Kerbel RS, Golfinos JG, **Hernando E, **Zaim Wadghiri Y (2013). Development and Characterization of a Clinically Relevant Mouse Model of Melanoma Brain Metastasis . Pigment Cell & Melanoma Res.26(5):743-5. PMID: 23647875.
[2] Shadaloey, A. A. S., Karz, A., Moubarak, R. S., Agrawal, P., Levinson, G., Kleffman, K., Aristizabal, O., Osman, I., Wadghiri, Y. Z., Hernando, E. A Robust Discovery Platform for the Identification of Novel Mediators of Melanoma Metastasis. J. Vis. Exp. (181), e63186 (2022).
[3] Kleffman K, Levinson G, Rose IVL, et al, Melanoma-Secreted Amyloid Beta Suppresses Neuroinflammation and Promotes Brain Metastasis. Cancer Discov. 2022 May 2;12(5):1314-1335.. PMID: 35262173; PMCID: PMC9069488.
[4] Feng L, Benkert T, Block KT, Sodickson DK, Otazo R, Chandarana H. Compressed sensing for body MRI. J Magn Reson Imaging. 2017 Apr;45(4):966-987. Epub 2016 Dec 16. PMID: 27981664; PMCID: PMC5352490.
Figures