4527
Post-Surgical Cavity Segmentation on MRI for Glioma Patients with Deep Learning and Transfer Learning Approach1Centre for Biomedical Engineering, Indian Institute of Technology, Delhi, New Delhi, India, 2Department of Radiology, Fortis Memorial Research Institute, Gurugram, India, 3Department of Electrical Engineering, Indian Institute of Technology, Delhi, New Delhi, India, 4Yardi School of Artificial Intelligence, Indian Institute of Technology, New Delhi, India, 5Department of Biomedical Engineering, All India Institute of Medical Sciences, New Delhi, India
Synopsis
Keywords: Diagnosis/Prediction, Tumor, Post cavity segmentation
Motivation: Currently, manual/semiautomatic methods are being used for post-surgical cavity segmentation in glioma patients, which is crucial for precise treatment planning and monitoring.
Goal(s): To evaluate the potential of deep learning models for automatic post-surgical cavity segmentation.
Approach: Deep learning models were trained on pre-surgery and post-surgery (within 72hours) MRI data and tested on post-surgery data. The concept of data augmentation and transfer learning were also used.
Results: Initially trained on the pre-surgery BraTS’2021 challenge dataset, the models underwent further refinement with local hospital's post-surgical data, resulting in 36% improvement in post-surgical cavity segmentation (U-Net3, DSC = 0.64).
Impact: This study demonstrates the potential of deep-learning in automatic segmentation of post-surgical cavity on MRI images. Proposed automatic segmentation models can assist in fast and objective treatment planning. Further optimizations for improved accuracy and validation on large dataset is required.
INTRODUCTION
The significance of segmenting the post-surgical cavity for glioma patients lies in its crucial role in treatment planning and monitoring1,2. Accurate segmentation allows healthcare professionals to assess the extent of tumor removal and plan follow-up treatments, such as radiation therapy. It also provides a means of monitoring disease progression and evaluating treatment effectiveness. The use of tumor lesion mask generated on pre-surgery images for radiation planning and monitoring is challenging due to brain deformation after surgery, particularly in large size tumors. Segmenting post-surgical cavities, particularly within few days of surgery, in glioma patients poses several challenges3. These include intensity heterogeneity, variations in cavity shape, size, and location, as well as the presence of surrounding edema and residual tumor tissue2,3 The contouring process is one of the laborious and time-consuming aspects of radiotherapy planning2. Additionally, image quality and variability in imaging techniques can complicate accurate segmentation1. Overcoming these difficulties is essential for precise treatment planning and monitoring in glioma patients1,2,4. The primary goal of this study is to develop a deep learning(DL) approach for performing segmentation of post-surgical cavity, leading to more accurate and reliable results in treatment planning and monitoring.MATERIALS & METHODS
MRI data were collected from the BraTS'21 Challenge5, encompassing pre-operative scans from 1251 patients, and from a local hospital, comprising post-operative scans from 41 patients with glioma. The post-operative scan includes T1-weighted, dual proton density-weighted(PD-W), T2-weighted, FLAIR, post-contrast T1-W, susceptibility-weighted imaging(SWI) and T1 Inversion-Recovery(T1IR). Ground truth(GT) masks for post-surgical cavities were generated with the help of k-means clustering algorithm using SWI sequences. These were validated and refined by an experienced radiologist. These masks were applied to FLAIR images and subsequent training/testing was carried out on FLAIR images. The data from the BraTS'21 challenge had already undergone preprocessing. In the local hospital dataset, preprocessing was carried out using the SPM12 toolbox. The BraTS'21 dataset was divided into training and validation sets in an 80:20 ratio, while the local hospital dataset underwent a similar split into training and testing sets. All images were resized to 240x240 dimensions and normalized. Both U-Net6 and MultiResU-Net7(MR U-Net) were trained. For transfer learning, the DL models were initially trained on the BraTS'21 training set (FLAIR images using whole tumor as GT) and subsequently fine-tuned on the local hospital dataset(DSLHTr). The entire process is illustrated in Figure 1, and the training parameters are detailed in Table 1. During the testing phase, all models were evaluated on the local hospital test dataset (DSLHTe), with the Dice Similarity Coefficient(DSC) serving as the performance metric.RESULTS
U-Net1 and MR U-Net1 models were trained on the DSLHTr dataset and assessed on the DSLHTe dataset, achieving DSC scores of 0.47 and 0.48, respectively. U-Net2 and MR U-Net2 models, initially trained on the BraTS'21 dataset and tested on DSLHTe, obtained DSC scores of 0.37 and 0.39. Subsequently, these U-Net2 and MR U-Net2 models were fine-tuned using the DSLHTr dataset resulting in U-Net3 and MR U-Net3 and re-evaluated on DSLHTe, resulting in improved DSC scores of 0.64 and 0.61, as shown in Table-2. Refer to Figure 2 for qualitative assessment.DISCUSSION
The study aims to demonstrate the potential of DL models in segmenting post-surgical cavities. The dataset used in this study consists of post-operative data collected within 72 hours of surgery. The choice to employ both U-Net and Multi Res U-Net models was based on their well-established reputation for accurately and effectively delineating structures, lesions, and regions of interest in medical images. Comparing the performance of the DL models on our local dataset versus the BraTS dataset, we observed that the models trained on the local data outperformed those trained on the BraTS dataset for post-surgery data of local hospital. The same is evident from the Figure 2 that the network trained on the BraTS data highlights the entire area encompassing both the post-surgical cavity and edema. This outcome is expected, as the BraTS dataset contains only pre-operative MR scans. To address this limitation, we adopted a transfer learning approach, where models initially trained on the BraTS data were further fine-tuned using our local hospital's post-surgical data. This strategy resulted in a remarkable 36% enhancement in the Dice Score for post-surgical cavity segmentation. Further optimization need to be carried out for improving accuracy and validation on large data from multi-center.CONCLUSION
Accurate post-surgical cavity segmentation is vital for glioma patient treatment planning and monitoring. The current study's success in utilizing transfer learning to improve segmentation holds promise for enhancing precision and reliability within the field, addressing the challenges posed by cavity variations and complex brain anatomy.Acknowledgements
Authors, Virendra Kumar Yadav and Ankit Kandpal share equal authorship. The authors acknowledges dedication and collaboration of MedImg lab(IIT-D) members, whose hard work has been invaluable to the study.References
1. Nalepa, J. et al. Deep learning automates bidimensional and volumetric tumor burden measurement from MRI in pre- and post-operative glioblastoma patients. Comput. Biol. Med. 154, 1–49 (2023).
2. Ermiş, E. et al. Fully automated brain resection cavity delineation for radiation target volume definition in glioblastoma patients using deep learning. Radiat. Oncol. 15, 1–10 (2020).
3. Holtzman Gazit, M., Faran, R., Stepovoy, K., Peles, O. & Shamir, R. R. Post-operative glioblastoma multiforme segmentation with uncertainty estimation. Front. Hum. Neurosci. 16, 1–9 (2022).
4. Helland, R. H. et al. Segmentation of glioblastomas in early post-operative multi-modal MRI with deep neural networks. Sci. Reports 2023 131 13, 1–13 (2023).
5. Baid, U. et al. The RSNA-ASNR-MICCAI BraTS 2021 Benchmark on Brain Tumor Segmentation and Radiogenomic Classification. (2021).
6. Ronneberger, O., Fischer, P. & Brox, T. U-net: Convolutional networks for biomedical image segmentation. Lect. Notes Comput. Sci. (including Subser. Lect. Notes Artif. Intell. Lect. Notes Bioinformatics) 9351, 234–241 (2015).
7. Ibtehaz, N. & Rahman, M. S. MultiResUNet : Rethinking the U-Net Architecture for Multimodal Biomedical Image Segmentation. (2019).
Figures
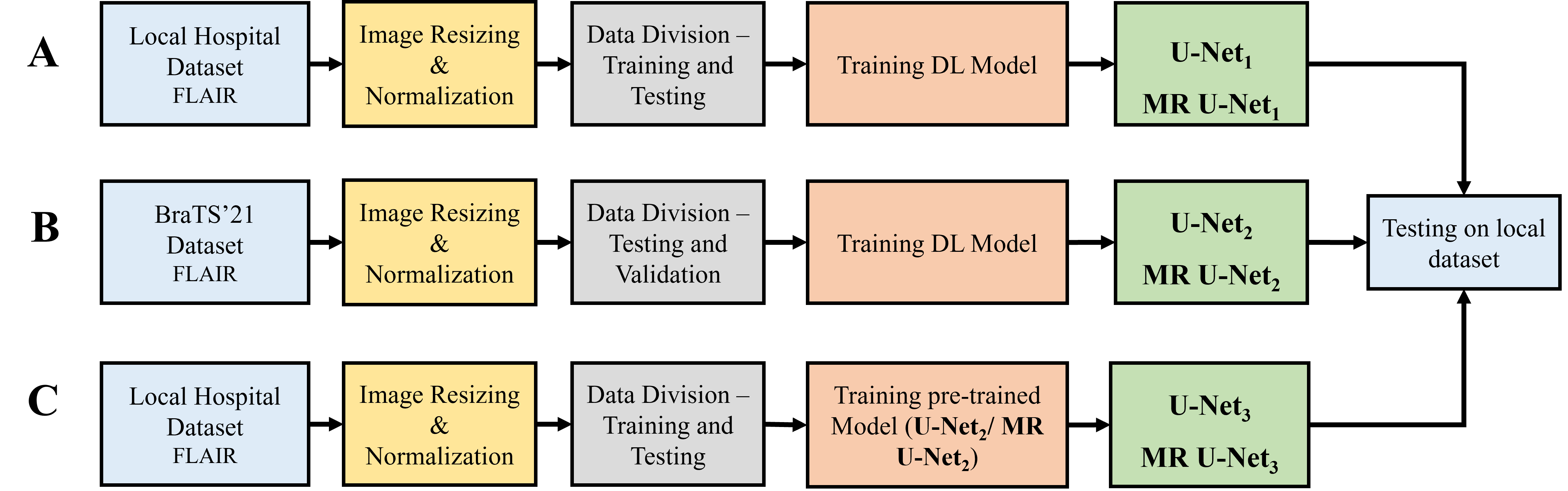
Figure 1. A workflow that demonstrates the stages in creating an automated model for post-surgical cavity segmentation and then assessing its performance using the Dice Similarity Coefficient (DSC) on a distinct test dataset. (A) Pipeline for developing U-Net1 /MR U-Net1; (B) Pipeline for developing U-Net2 /MR U-Net2; (C) Pipeline for developing U-Net3 /MR U-Net3 (transfer learning) (Abbreviations: - MR U-Net: MultiRes U-Net).
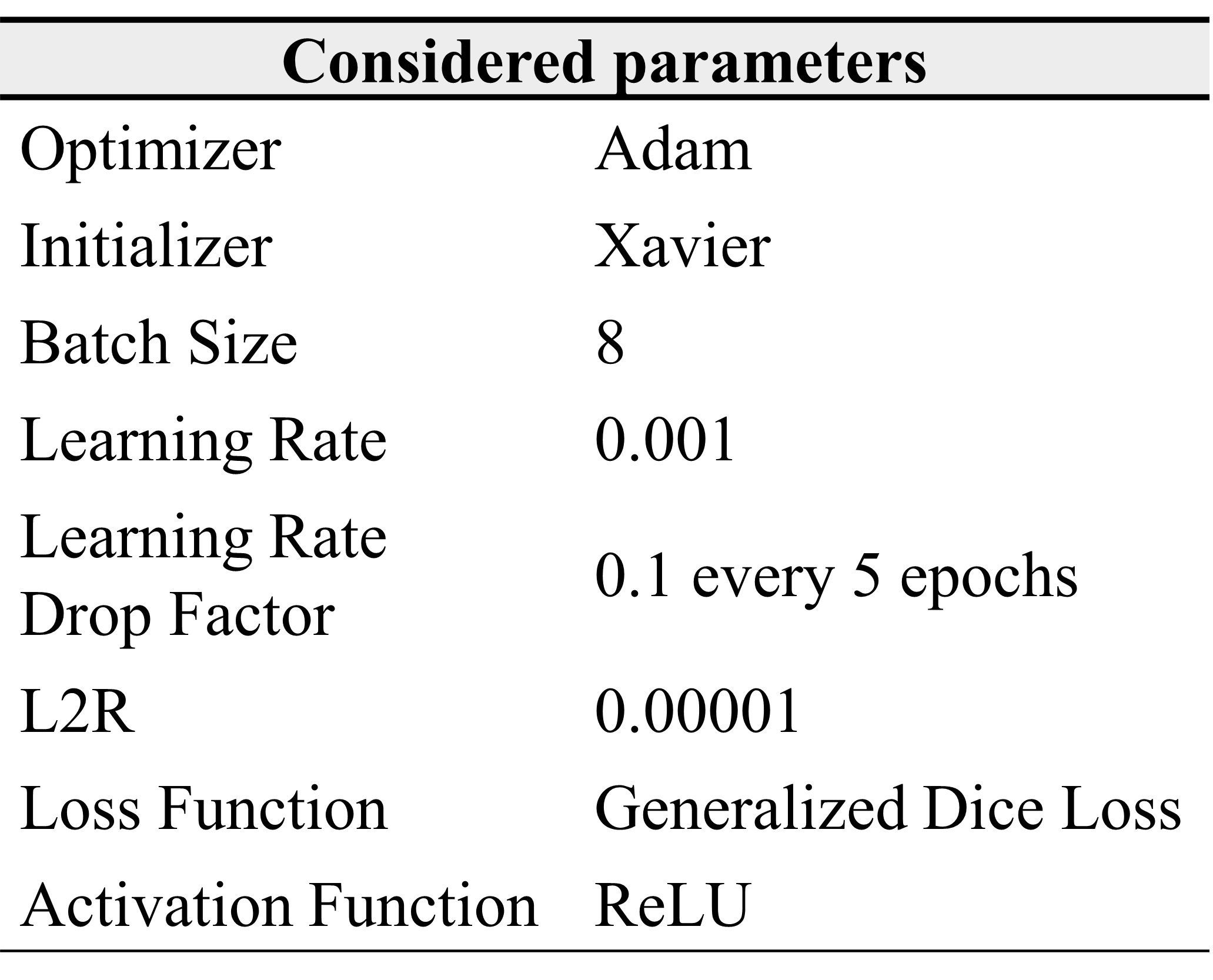
Table 1. Presents the optimized network parameters for the developed deep learning models.
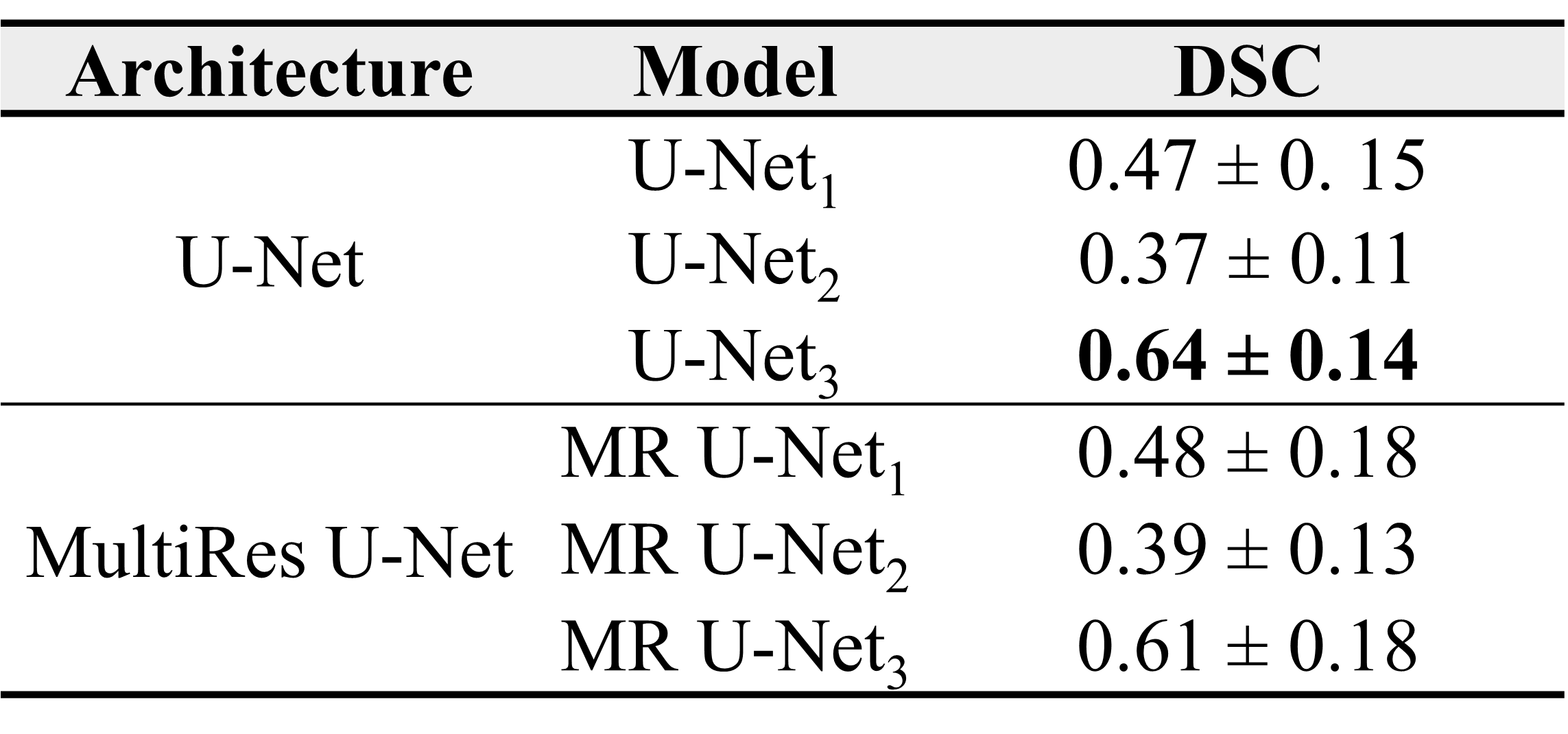
Table 2. Presents the Dice Similarity Coefficient (DSC) of the developed models on local hospital test dataset under different training conditions: utilizing only local hospital training data (U-Net1 /MR U-Net1), utilizing only BraTS’21 dataset (U-Net2 /MR U-Net2), further training U-Net2 / MR U-Net2 on local hospital training data, hence resulting in U-Net3 /MR U-Net3 (Abbreviations: - MR U-Net: MultiRes U-Net).
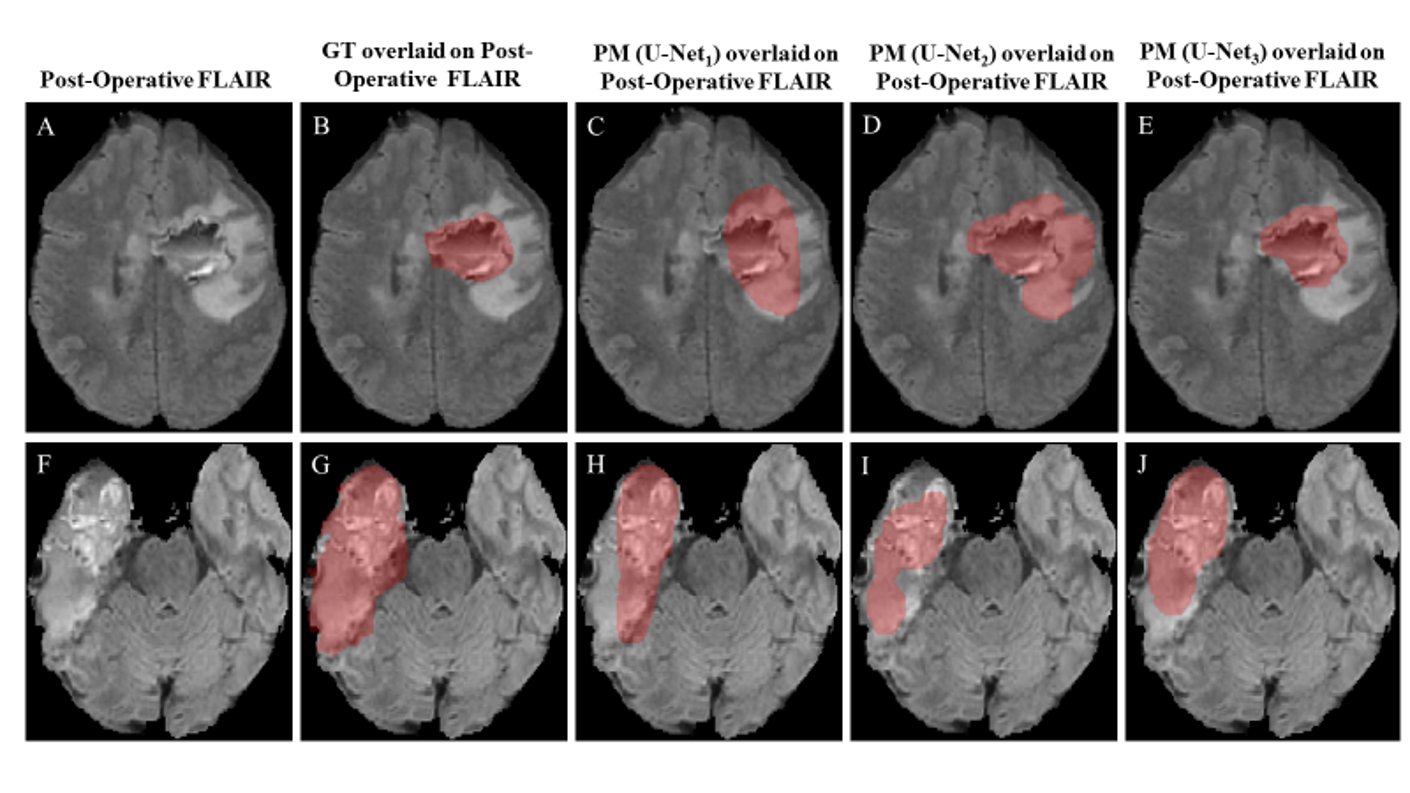
Figure 2. Provides a visual comparison between the results obtained by the developed deep learning models and the ground truth (GT). Subfigures (A-J) present the post-operative FLAIR image, post-operative FLAIR image with overlaid GT (B, G), FLAIR image with U-Net1 predicted tumor mask overlay (C, H), post-operative FLAIR image with U-Net2 predicted tumor mask overlay(D, I) and post-operative FLAIR image with U-Net3 predicted tumor mask overlay(E, J), all pertaining to glioma patients (Abbreviations:- FLAIR: fluid-attenuated-inversion-recovery; PM: predicted masks).