4506
Joint group sparsity-based motion-compensated deep learning reconstruction for 3D whole-heart joint T1/T2 mapping1School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 2King’s Institute for Artificial Intelligence, London, United Kingdom, 3MR Research Collaborations, Siemens Healthcare Limited, Camberley, United Kingdom, 4School of Engineering, Pontificia Universidad Católica de Chile, Santiago, Chile, 5Millennium Institute for Intelligent Healthcare Engineering, Santiago, Chile
Synopsis
Keywords: AI/ML Image Reconstruction, Cardiovascular
Motivation: Myocardial T1 and T2 mapping is crucial in the assessment of cardiovascular disease. 3D whole-heart joint T1/T2 mapping approaches have been proposed, however they require long reconstruction times.
Goal(s): By leveraging deep learning (DL)-based techniques, we aim to significantly reduce the reconstruction times for 3D whole-heart joint T1/T2 mapping, while maintaining high-quality results.
Approach: Recently a joint group sparsity-based DL approach was proposed for image reconstruction of undersampled multi-contrast MRI data. Here, we propose to extend this approach for non-rigid motion-corrected reconstructions for multi-contrast 3D data for joint T1/T2 mapping.
Results: Our approach achieves good agreement with reference techniques, while outperforming single-contrast reconstructions.
Impact: Joint group sparsity-based deep learning non-rigid motion-corrected reconstruction for multi-dimensional joint 3D T1/T2 whole-heart mapping achieves good agreement with reference techniques and outperforms single-contrast reconstructions. The approach significantly reduces reconstruction times, making it feasible for clinical applications.
Introduction
Myocardial T1 and T2 mapping play an important role in the assessment of cardiovascular disease (CVD)1. Recently, a free-breathing high-resolution, motion-compensated 3D joint T1/T2 water/fat sequence has been proposed and validated in phantom and healthy subjects2. To obtain the 3D whole-heart T1 and T2 maps, a reconstruction of eight intermediate motion-compensated volumes is needed, which is very time consuming. Recently, a joint group sparsity-based network approach (JGSN)7 was proposed and applied for the reconstruction of multi-contrast single coil static imaging. JGSN was evaluated on two combinations of two contrasts; T1 and T2 weighted brain images, and proton density weighted image with and without fat-suppression of knee data. In this work we propose to extend this approach for the joint reconstruction of the eight intermediate contrasts for multi-coil joint 3D T1/T2 mapping. This enables a joint, regularised motion compensated reconstruction (MC-JGSN) from the free-breathing undersampled data, while increasing the speed and maintaining the quality of the reconstructions.Methods
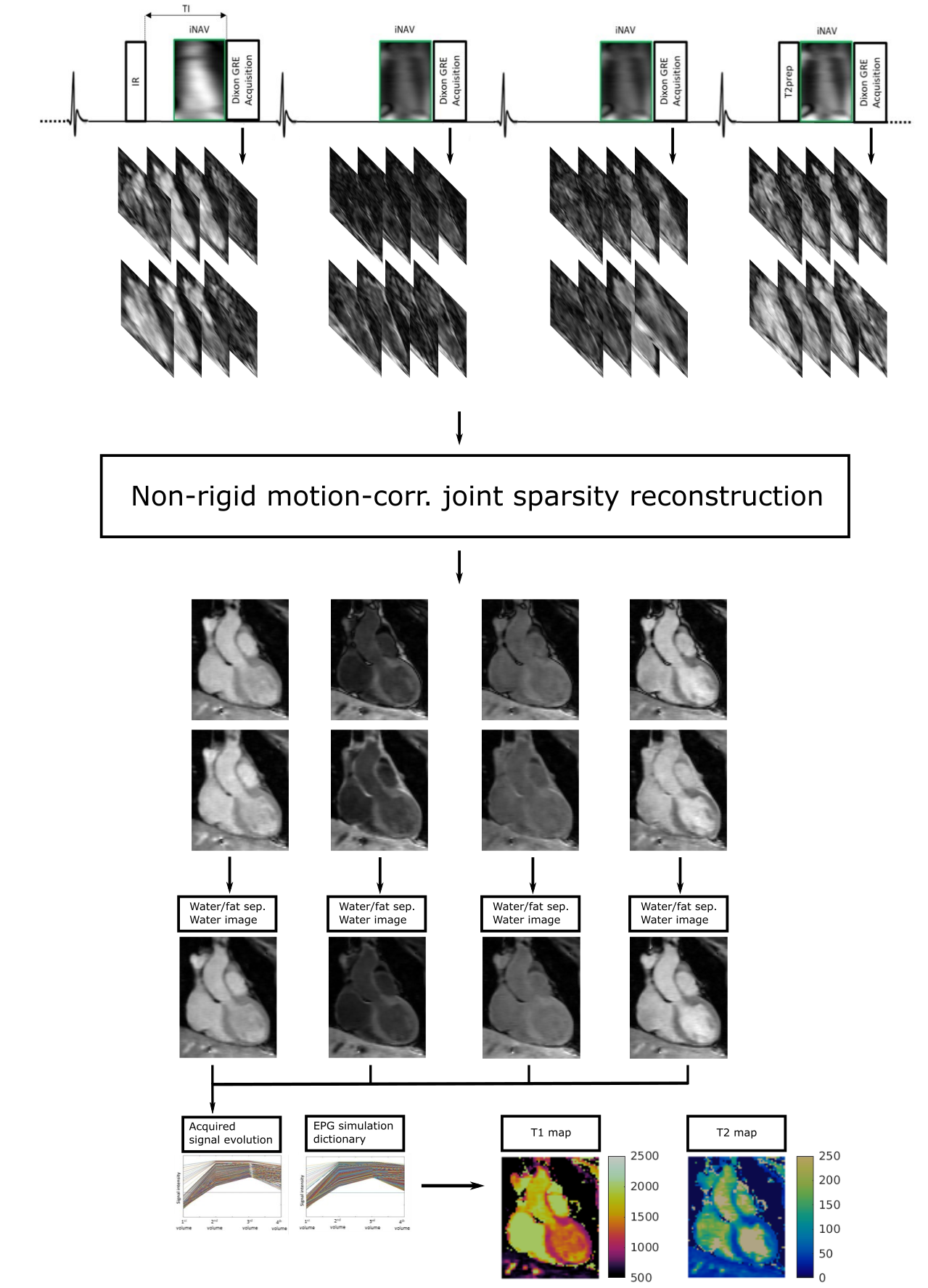
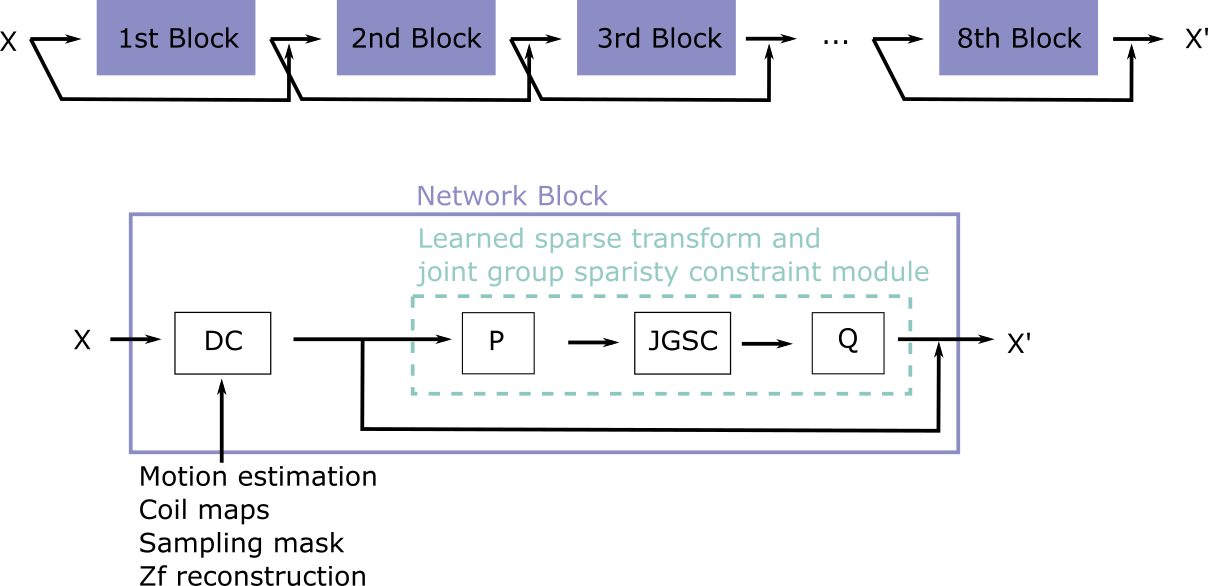
The proposed pipeline and MC-JGSN network are shown in Figure 1 and 2. The joint T1/T2 water/fat mapping research sequence2 uses a 4x undersampled variable density Cartesian trajectory3 and acquires four interleaved, ECG-triggered spoiled gradient-echo volumes with 2-point bipolar Dixon encoding. Prior to the first and fourth volume an inversion recovery and T2 preparation pulse is used, whereas no preparation is used prior to the second and third interleaves. Image navigators are employed to enable non-rigid respiratory motion correction. Maps are generated based on dictionary matching.MC-JGSN is extended from the proposed two-contrast application7 to the reconstruction of eight non-rigid motion-corrected volumes. Due to the high data requirements, the network was applied to 2D-slices of the 3D-volume. The network was trained using a weighted ADAM optimizer with a learning rate of 0.001. The network was trained for 50 epochs with a training/testing split of 52/6. Details on the learned sparse transform and joint group sparsity constraint module can be found in Guo et al.7.
After the reconstruction of the eight multi-contrast images, a water-fat separation algorithm is applied and a patient specific dictionary of pre-calculated T1/T2 combinations is matched against the measured water image signal evolution, resulting in the final T1/T2 maps.
Acquisitions were performed at 1.5T (MAGNETOM Aera, Siemens Healthineers AG, Erlangen, Germany) on 58 subjects (34 patients with suspected CVD and 24 healthy subjects). Main acquisition parameters were FA=8˚, TR = 6.67ms, TE1/TE2=2.38/4.76ms, 2mm3 isotropic resolution and a subject specific mid-diastolic trigger-delay and acquisition window of ~100ms, resulting in a total scan time of nine minutes. The data was pre-processed for each contrast by computing a high quality refence image with a high-dimensional patch-based higher order low-rank (HD-PROST) reconstruction5. A reference high-quality respiratory bin image, together with undersampled respiratory bin images for all contrasts reconstructed using zero-filling and respective motion fields, are inputted into the network. Non-rigid inter-bin respiratory motion fields are estimated using NiftyReg8. The motion correction is applied in each data consistency step.
Results
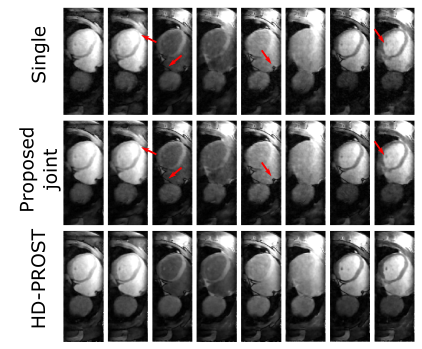
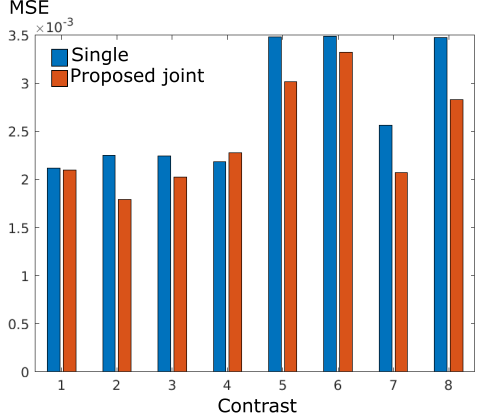
Reconstruction results for the proposed multi-contrast MC-JGSN reconstruction are shown in Fig. 3 for one example test-set subject for all eight contrasts in comparison to reference HD-PROST reconstruction and the reconstruction for each contrast individually. Comparable visual image quality is achieved between the proposed approach MC-JGSN and HD-PROST. The proposed MC-JGSN joint reconstruction outperformed the single-contrast reconstructions in terms of image sharpness. The most prominent differences are marked with red arrows. MSE error with respect to the reference images is compared for the single-contrast reconstructions and joint reconstructions (Fig. 4), showing an advantage of the joint reconstruction over the single reconstructions. The computed T1 and T2 maps are shown in Fig. 5 for the same subject, showing the improved sharpness and comparable T1 and T2 septum values, especially in the T2 map. The proposed MC-JGSN reconstruction took about 3s per slice for the joint reconstruction and 4.2s per slice for all eight contrasts for the single-contrast reconstruction. Please note that here we do not consider the overhead in loading the data. We report a time of over 2 hours for HD-PROST for the complete volume.Conclusion
We have proposed joint group sparsity-based deep learning approach for motion-compensated multi-contrast MRI reconstruction in the context of myocardial 3D T1/T2 mapping. The proposed approach shows comparable image quality to the reference HD-PROST reconstruction, while significantly reducing reconstruction time. We also found an enhanced quality of the joint reconstruction over the single reconstructions. Extension of the proposed approach to a 3D network and application in an end-to-end manner for both motion estimation and reconstruction will be investigated as future work.Acknowledgements
This work was supported by the following grants: (1) EPSRC P/V044087/1; (2) BHF programme grant RG/20/1/34802, (3) Wellcome/EPSRC Centre forMedical Engineering (WT 203148/Z/16/Z), (4) Millennium Institute for Intelligent Healthcare Engineering ICN2021_004, (5) FONDECYT 1210637 and1210638, (6) IMPACT, Center of Interventional Medicine for Precision and Advanced Cellular Therapy, ANID FB210024.References
1. Messroghli, D.R., Moon, J.C., Ferreira, V.M. et al. Clinical recommendations for cardiovascular magnetic resonance mapping of T1, T2, T2* and extracellular volume: A consensus statement by the Society for Cardiovascular Magnetic Resonance (SCMR) endorsed by the European Association for Cardiovascular Imaging (EACVI). J Cardiovasc Magn Reson 2017; 19, 75.
2. Milotta, G, Bustin, A, Jaubert, O, Neji, R, Prieto, C, Botnar, RM. 3D whole-heart isotropic-resolution motion-compensated joint T1/T2 mapping and water/fat imaging. Magn Reson Med. 2020; 84: 3009– 3026.
3. Prieto C, Doneva M, Usman M, et al. Highly efficient respiratory motion compensated free-breathing coronary MRA using golden-step Cartesian acquisition. J Magn Reson Imaging. 2015; 41: 738-746.
4. Qi, H, Hajhosseiny, R, Cruz, G, et al. End-to-end deep learning nonrigid motion-corrected reconstruction for highly accelerated free-breathing coronary MRA. Magn Reson Med. 2021; 86: 1983– 1996.
5. Bustin A, Ginami G, Cruz G, et al. Five-minute whole-heart coronary MRA with sub-millimeter isotropic resolution, 100% respiratory scan efficiency, and 3D-PROST reconstruction. Magn Reson Med. 2019; 81: 102-115.
6. Weigel, M. Extended phase graphs: Dephasing, RF pulses, and echoes - pure and simple. J. Magn. Reson. Imaging 2015; 41: 266-295.
7. Guo, D., Zeng, G., Fu, H., Wang, Z., Yang, Y., & Qu, X. (2023). A Joint Group Sparsity-based deep learning for multi-contrast MRI reconstruction. Journal of Magnetic Resonance, 346, 107354.
8. Modat M, Ridgway GR, Taylor ZA, Lehmann M, Barnes J, Hawkes DJ, et al. Fast free-form deformation using graphics processing units. Computer Methods and Programs in Biomedicine. 2010;98(3):278–284.
Figures