4494
Rapid LAVA imaging with deep learning reconstruction: evaluation of image quality and diagnostic performance in patients with liver cancer1Department of Radiology, First Affiliated Hospital,School of Medicine,ZheJiang University, Hangzhou, China, 2MR Research, GE Healthcare, Beijing, China
Synopsis
Keywords: AI/ML Image Reconstruction, Cancer
Motivation: 3D gradient-echo based liver acceleration volume acquisition (LAVA) sequence is widely used for dynamic contrast imaging in liver. LAVA usually requires breath-holding for over 16 seconds, posing a challenge for individuals with difficulty in prolonged breath-holding.
Goal(s): To investigate whether deep learning reconstruction (DLR) allows for LAVA imaging with reduced scan time but without sacrificing image diagnostic quality.
Approach: SNR, CNR, and subjective analysis using 5-point Likert scales were compared to evaluate the image quality and diagnostic performance between DLR-LAVA and conventional LAVA.
Results: Compared to conventional LAVA, DLR-LAVA showed similar SNR, CNR, and qualitative image quality scores.
Impact: Deep learning reconstruction based rapid LAVA imaging is promising for reducing breath-hold time while maintaining similar image quality compared with conventional LAVA imaging.
Introduction
Liver cancer is the second leading cause of cancer-related deaths worldwide 1. Dynamic contrast-enhanced (DCE) MRI has been extensively applied in clinic for liver cancer diagnosis due to its diverse tissue contrast mechanisms and its capacity to assess imaging features 2. A commercially available 3D liver acceleration volume acquisition (LAVA) imaging 3 is routinely applied in clinic for contrast-enhanced abdominal examination.Dynamic LAVA imaging for liver is usually acquired in breath-hold manner, requiring over 16 seconds per phase. The relative long breath-hold time can be challenging for patients to cooperate, resulting in poor image diagnostic quality. To address this issue, a vendor-provided deep learning reconstruction (DLR; AIRTM Recon DL, GE Healthcare), developed by training a neural network for noise removal and other artifact elimination from original k-space data, allows for rapid image acquisition without sacrificing image quality 4. Previous studies predominantly evaluated the clinical value of DLR in 2D MR imaging of lumbar spine, prostate and other anatomical structures, since increased SNR, imaging sharpness as well as diminished imaging artifact allowed for rapid imaging acquisition, increased image resolution, robust diagnostic efficacy and so on5,6. However, few studies have been performed to explore the impact of DLR on 3D MR imaging.
In this study, we aimed to investigate if DLR for high image quality allowed for rapid 3D LAVA imaging in liver cancer diagnosis by comparing with the reference of conventional 3D LAVA images at portal phase.
Methods
20 patients (16 with liver cancer, 4 with ductal cancer) were enrolled in this study with institutional review board approval. The conventional portal phase 3D LAVA (Con-LAVA) breath-hold sequence was scanned on a 3 T platform (SIGNA Architect, GE Healthcare) with a 30ch adaptive image receive coil employed. The scan parameters were of: TR=3.9 ms; TE=1.7 ms; field-of-view=36×36 cm2; matrix=352×288; slice thickness=1.5 mm; NEX=1; Intensity Filter F; acceleration factor for parallel imaging=3. For rapid 3D LAVA sequence, the applied scan parameters were the same as for Con-LAVA, but with the acceleration factor of 4. The accelerated 3D LAVA images were separately reconstructed with DLR (Acc-DLR-LAVA) and without DLR (Acc-LAVA).Two readers with 5 years and 7 years experiences independently assessed the image quality. SNR of livers (SNRliver=SIliver /SDliver), SNR of tumors (SNRtumor=SItumor /SDtumor), CNR between tumors and liver normal tissues ($$$CNR=\frac{|SItumor-SIliver|}{\sqrt{SDtumor^{2}+SDliver^{2}}}$$$) were calculated for Con-LAVA, Acc-LAVA, and Acc-DLR-LAVA. The quality of images was evaluated based on a 5-point scale (5, excellent; 4, good; 3, acceptable, not affecting diagnosis; 2, poor, affecting diagnosis; and 1, nondiagnostic) 7.
The intraclass correlation coefficient (ICC) was used to evaluate the inter-observer agreement of the image quality scores (0.21–0.40, poor; 0.41–0.60, moderate; 0.61–0.80, good; 0.81–1.00, excellent). ANOVA with Bonferroni correction was used to compare SNR and CNR among three imaging sets. Wilcoxon signed-rank test was used to compare the image quality scores. P value < 0.05 was considered statistically significant. All statistical analyses were performed using SPSS (IBM, v20.0).
Results
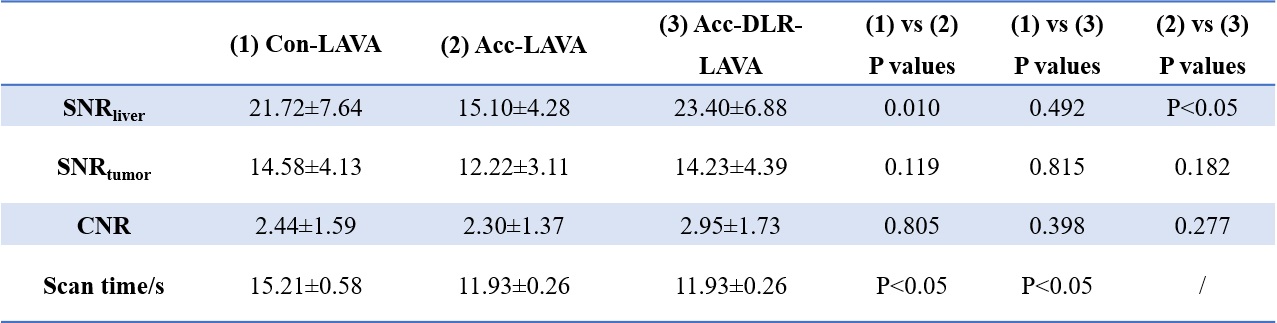
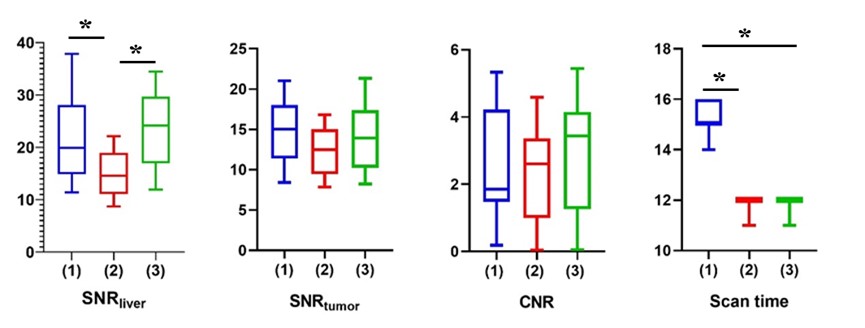
ICC values for all indices measured by two readers were greater than 0.80, indicating excellent inter-observer agreement. The mean levels of quantitative measures by two readers were thus used in subsequent analyses.For SNR and CNR, compared to Con-LAVA, Acc-DLR-LAVA showed no difference (P>0.05), and Acc-LAVA showed a noticeable decrease trend (P < 0.05 for SNRliver; Fig.1 and Tab.1).
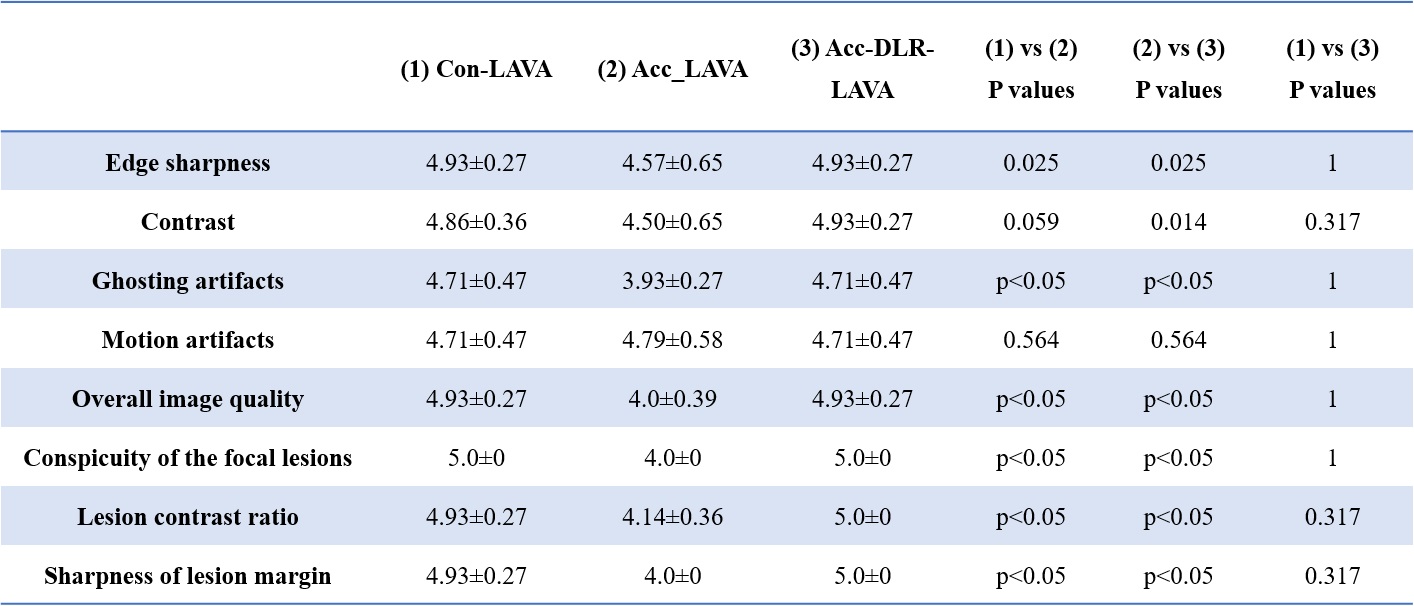
Acc-DLR-LAVA received comparable scores, rated for image quality, relative to Con-LAVA, indicating sufficient image quality. Significantly higher scores were revealed in Acc-DLR-LAVA and Con-LAVA if compared with Acc-LAVA (P < 0.05; Tab.2 and Fig.2).
The acquisition time for Acc-DLR-LAVA (11.93±0.26s) was significantly shorter than the Con-LAVA (11.93±0.26s vs 15.21±0.58s; P<0.05).
Discussion
In our study, accelerated LAVA imaging after DLR offered sufficient image quality and clear lesion margin compared to the conventional LAVA imaging, validated by comparable SNR, CNR, and qualitative image quality scores. With these, DLR LAVA sequence, however, required only an acquisition time of 11.93s, significantly shorter than conventional LAVA sequence, suggesting a substantial advantage for patients with difficulty holding breath for extended durations.Conclusion
Accelerated LAVA imaging after DLR has been demonstrated to shorten the acquisition time without compromising image quality, offering potential clinical benefits for patients who struggle with prolonged breath-hold and improving the overall comfort of patient examinations.Acknowledgements
No acknowledgement found.References
1. European Association for the Study of the Liver. EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2018, 69:182–236.
2. An C, Rakhmonova G, Choi JY, Kim MJ. Liver imaging reporting and data system (LI-RADS) version 2014: understanding andapplication of the diagnostic algorithm. Clin Mol Hepatol. 2016; 22:296–307.
3. Liu, T., Wang, Y., Xu, Z., et al. Application study of 3D LAVA-Flex on lumbar intervertebral disc degeneration. European Journal of Medical Research. 2021; 26(1): 1-8.
4. Lebel RM. Performance characterization of a novel deep learning-based MR image reconstruction pipeline. arxiv.org/abs/2008.06559.
5. Han, M., Bahroos, E., Hess, et al. Technology and Tool Development for BACPAC: Qualitative and Quantitative Analysis of Accelerated Lumbar Spine MRI with Deep-Learning Based MR Image Reconstruction at 3T. Pain Medicine. 2023; pnad035.
6. Ueda, T., Ohno, Y., Yamamoto, K., et al. Deep learning reconstruction of diffusion-weighted MRI improves image quality for prostatic imaging. Radiology. 2022; 303(2): 373-381.
7. Kim, D. H., Kim, B., Lee, H. S., et al. Deep Learning–Accelerated Liver Diffusion-Weighted Imaging: Intraindividual Comparison and Additional Phantom Study of Free-Breathing and Respiratory-Triggering Acquisitions. Investigative Radiology. 2023; 58(11): 782-790.
Figures