4492
ML models for 4D cine imaging1Centre for Translational Cardiovascular Imaging, UCL, London, United Kingdom
Synopsis
Keywords: AI/ML Image Reconstruction, Machine Learning/Artificial Intelligence
Motivation: The motivation behind this study is to severely shorten scan times for children undergoing cardiac examination.
Goal(s): The goal is to be able to create a 4D dataset from a short, free breathing real-time 2D stack of images.
Approach: We apply three machine learning models to the 2D stack. The first reconstructs the undersampled image data, the second corrects respiratory artefacts caused by free-breathing and the third model super resolves the images.
Results: The image quality is vastly improved after applying the machine learning models. The ventricular volumes are also in good agreement with the reference volumes.
Impact: Severely reduced scan times for comprehensive cardiac examination in CHD without the use of breath-holds. Machine Learning methods may be able to also be used for other imaging sequences, also resulting in faster image acquisition.
Introduction
Comprehensive cardiac examination in CHD normally includes a 2D short-axis stack of cine images (for assessment of ventricular function), as well as acquisition of 3D whole-heart (for anatomical assessment). Unfortunately, these sequences are time consuming, taking ~15 mins, and often require multiple breath holds. True 4D cine imaging is possible, but both acquisition and reconstruction are complex and take longer than is clinically tractable. In this study we investigated the possibility of reconstructing 4D cine images from a stack of sagittal radial real-time 2D cines that are rapidly acquired during free-breathing (total scan time ~ 40 seconds). We used ML to correct for interslice respiratory motion and poor through plane resolution and the aim of this study was to assess the accuracy of the resultant framework.Methods
Three consecutive machine learning networks were used to create 4D cine images (Figure 1) from real-time 2D cine data, as described below:1. Reconstruction of the 2D real-time images
A multi-coil complex 3D U-net was trained as previously described to perform de-aliasing of the real-time 2D images after standard NUFFT reconstruction of the undersampled radial. The ground truth training data was 2D breath-hold bSSFP cine data and the input was synthetically radially under-sampled cine data1.
2. Respiratory correction
A 3D U-Net was trained to correct for the non-rigid misalignment between consecutive slices caused by free-breathing during the 2D cine acquisition. The ground truth training data was Isotropic 3D whole heart data (389 volumes) with 1.5x1.5x1.5mm voxel size. The simulated input was created by first down-sampling the whole heart data in the sagittal dimension to match the real-time cine data slice thickness. Respiratory motion was then simulated for each down-sampled slice by performing a randomly parameterized non-rigid deformation. The network had two output channels for the x and y deformation fields, which were then applied to the input data to correct for respiratory motion and match the ground truth 3D data.
3. Super-resolution reconstruction
A 3D U-Net was also used to perform super resolution (SR) along the slice direction. The ground truth training data was the high resolution whole heart data and the input was the through plane down-sampled data (with no added respiratory motion).
Prospective Study:
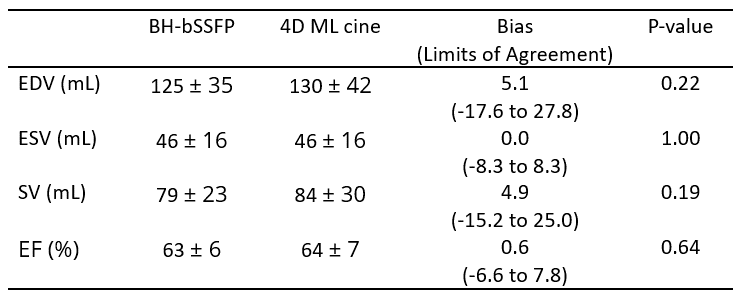
Prospective data was collected in 10 children with congenital heart disease (two patients with single ventricles). Reference standard breath-hold bSSFP SAX (~192x240 matrix, ~1.6x1.6mm resolution, ~9mm slice thickness, 40 reconstructed cardiac phases.) and real-time 2D cine data were acquired in 20 consecutive slices in the sagittal plane during free-breathing using a tiny-golden angle radial bSSFP sequence (256x256 matrix, 1.4x1.4mm resolution, 8mm slice thickness, 13 radial spokes, ~23x acceleration, 40.2ms temporal resolution, 32 reconstructed cardiac phases). The real-time data was processed using the methods above, to create 4D cine data. Quantification of systemic ventricular volumes was calculated for both techniques, through manual segmentation by a CMR specialist (VM). End-diastolic volume (EDV), end-systolic volume (ESV), Stroke volume (SV), and ejection fraction (EF) were calculated 1.
Results
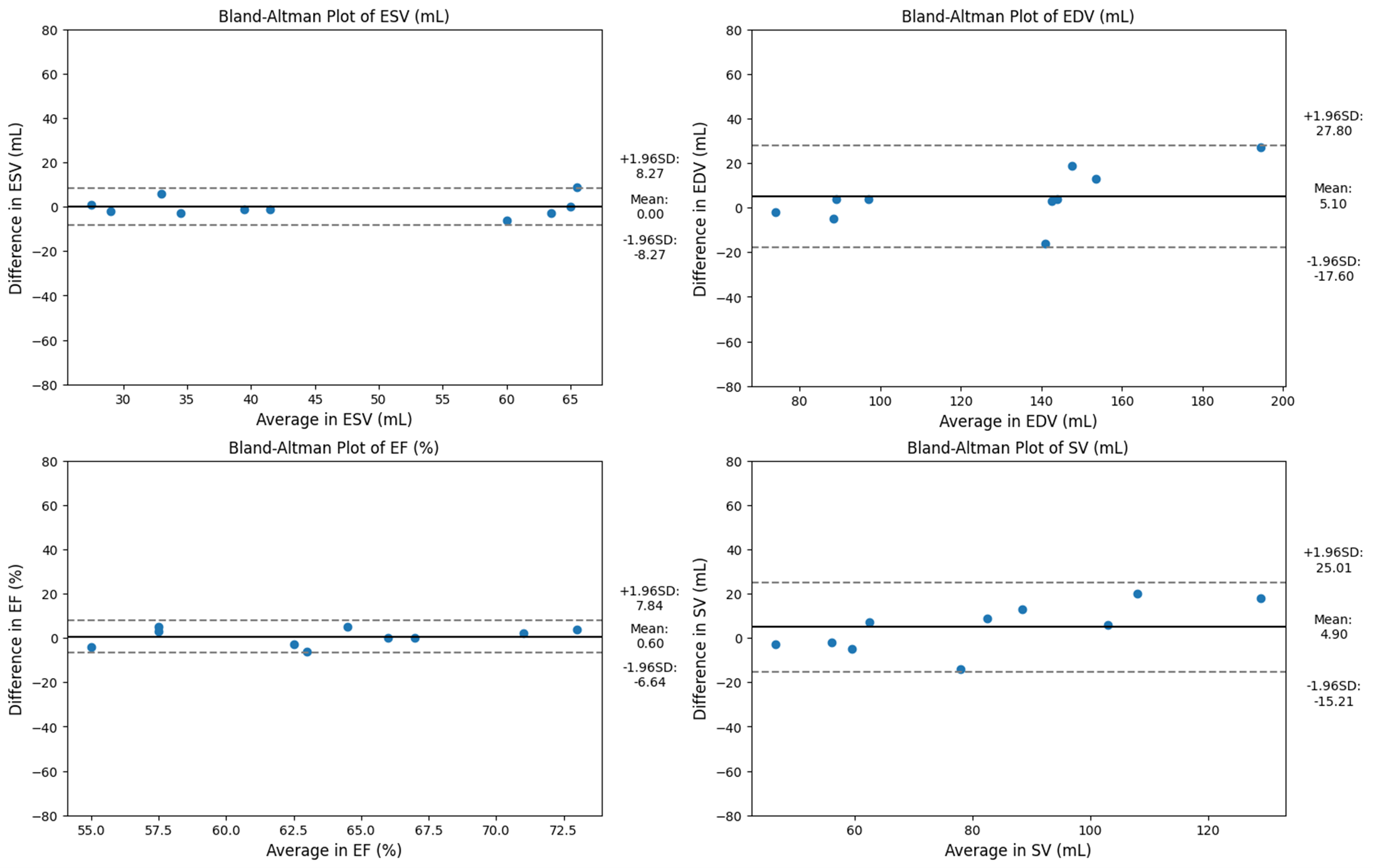
ML reconstruction was feasible in all cases and took ~1 minute. Figure 2 shows visual improvements in image quality after additional ML post-processing models are applied to the data. The respiratory correction model ensures continuity in the tissue across the slices of the image, while the SR model successfully improves the image resolution. Table 1 shows ventricular volumes from BH-bSSFP reference and the 4D ML cine data in good agreement with each other. Figure 3 shows Bland-Altman plots of the difference in ventricular volumes between the reference and the 4D ML cine with no significant bias.Discussion
Acquiring 4D cine data is highly desirable in evaluation of congenital heart disease as it allows assessment of function and anatomy. Current 4D techniques take several minutes to acquire, often require contrast, and have computationally intensive reconstructions. We have demonstrated that it is possible to use a combination of ML based interslice motion correction and super-resolution to create 4D cine data from multi-slice 2D+time real-time data. The benefit of this approach is that 2D SSFP has inherently high contrast, the stack can be acquired in less than a minute and the ML reconstruction are rapid. Ventricular volumes were in good agreement with the reference BH-bSSFP data. Thus, we believe 4D ML cine can replace 3D whole-heart scans and 2D short-axis cine images, vastly shortening scan times and eliminating the need for breath-holds.Conclusion
4D ML cine may be clinically useful as it has the potential to massively speed up scan times during comprehensive cardiac examination in CHD with the added benefit of not requiring breath-holds during scanning.Acknowledgements
No acknowledgement found.References
1. , , , , . Real-time cardiovascular MR with spatio-temporal artifact suppression using deep learning–proof of concept in congenital heart disease. Magn Reson Med. 2019; 81: 1143–1156. https://doi.org/10.1002/mrm.27480
Figures
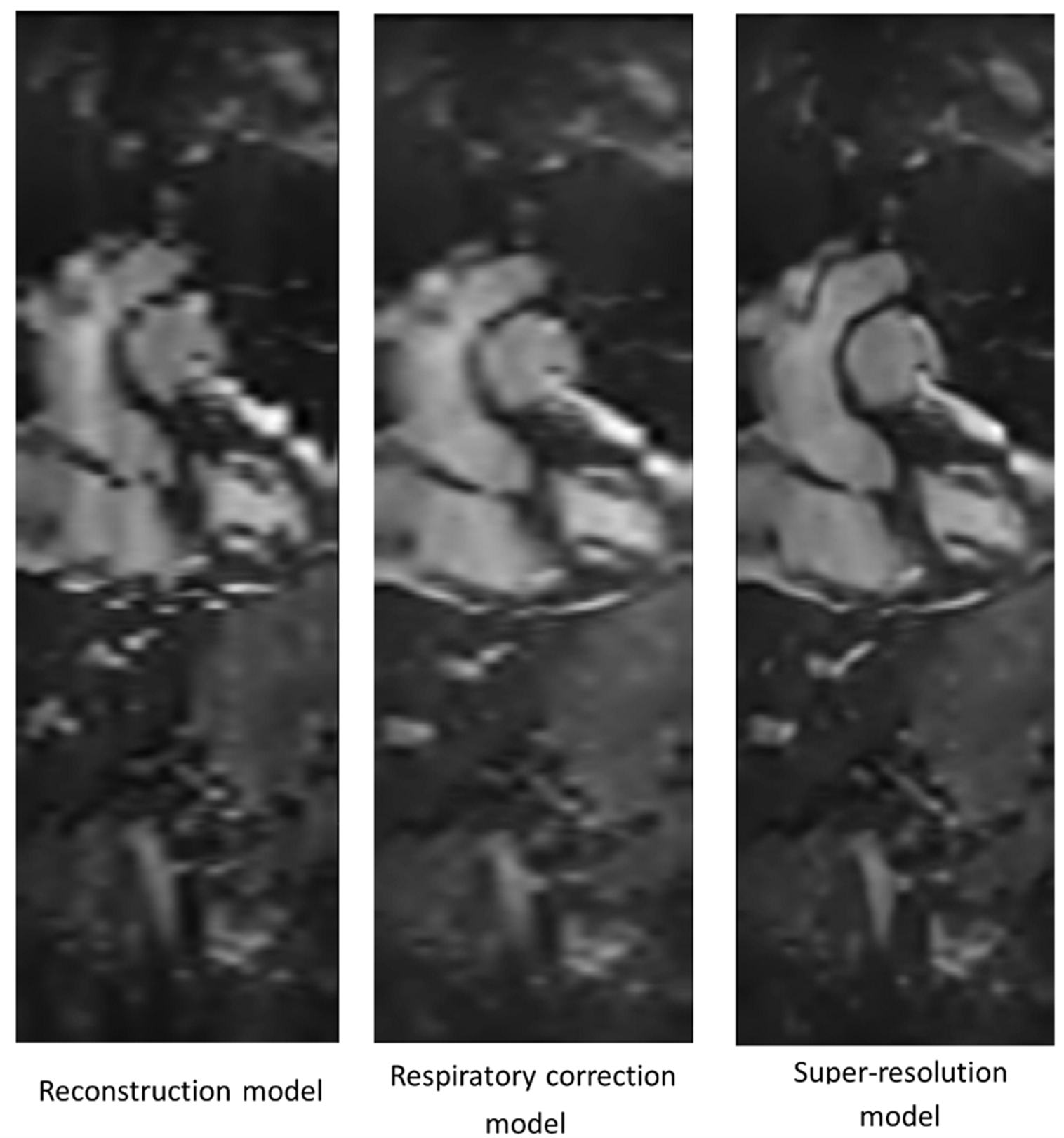
Figure 1: Images showing the cumulative application of ML models to the raw 2D cine data for an example timepoint