4464
Challenges for in-vivo hepatic GlycoNOE on human subjects at 7T1Magnetic Resonance Methodology, Institute of Diagnostic and Interventional Neuroradiology, University of Bern, Bern, Switzerland, Bern, Switzerland, 2Translational Imaging Center, Sitem-insel, Bern, Switzerland, Bern, Switzerland, 3Insel Hospital, University Hospital Bern, Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism UDEM, Bern, Switzerland, Bern, Switzerland
Synopsis
Keywords: CEST / APT / NOE, Spectroscopy, 13C-MRS, metabolism, validation, 7T, human
Motivation: The GlycoNOE technique promises advantages compared to GlycoCEST and spectroscopic methods for fast non-invasive determination of hepatic glycogen content on standard MRI systems.
Goal(s): Establish a robust glycoNOE technique at 7T for hepatic glycogen quantification in humans.
Approach: A single-voxel MRS technique was combined with CEST modules and tested in vitro and in human subjects together with standard 13C-MRS.
Results: The method gave excellent results in vitro, but in vivo the failure rate was substantial and shows that further refinements of the method are needed to provide robust measurements of hepatic glycogen in human subjects, especially in pathological conditions.
Impact: The GlycoNOE technique promises advantages compared to GlycoCEST and spectroscopic methods for determining hepatic glycogen content in vivo. Lack of robustness as implemented for a combined CEST-spectroscopy technique hinders its use in humans.
Introduction
Quantitative exploration of hepatic glycogen metabolism is highly relevant for the evaluation of glucose homeostasis in health and disease1–3. Current methods for glycogen quantification, including 1H- and 13C-MRS6–8, are limited by low SNR and need for specialized hardware (13C-MRS), additionally cost and incomplete detection of full glycogen stores (13C-MRS with labelled glucose), and uncertain signal specificity and quantification uncertainties (1H-MRS).GlycoCEST9,10 indirectly monitors glycogen by exploiting magnetization exchange between glycogen hydroxyl and water protons but has shown limited success in-vivo11 due to the fast hydroxyl proton exchange (need for high irradiation levels) and signal overlap with other sources.
GlycoNOE11, based on the nuclear Overhauser effect (NOE), has been proposed as a better alternative. It measures the exchange of magnetization between water and aliphatic glycogen protons. However, in the liver it also faces technical challenges like signal overlap with the direct saturation peak, sensitivity to frequency shifts from breathing and involuntary motion, as well as considerable energy deposition. Although GlycoNOE has been applied successfully in-vitro and in mouse liver, its robustness and reproducibility in human liver remains unproven.
The objectives of our project were: 1) to replicate the reported in-vitro results for a human scanner and 2) to probe the method's reliability for hepatic human application using a CEST-MRS technique that promises the benefit from direct frequency correction.
Methods
Data acquired at 7T (Terra, Siemens) with a triple-tuned 13C/2H/1H surface coil (Rapid Biomedical) in-vivo and a 64-channel extremity coil in-vitro.In-vitro: compartmental phantom with 25mm spheres, filled with 50, 150 and 300mM (glucose units) bovine (Type IX G0885) or rabbit (Type III G8876,) liver glycogen, dissolved in PBS at pH 7.4.
In-vivo: 16 healthy subjects, with 4 examinations for parameter optimization and 12 subjects investigated with optimized settings. Subjects fasted overnight in case of glucose loading or two hours after the last meal. 4 GlycoNOE investigations, interleaved with 13C-MRS scans to directly measure natural-abundance glycogen for 150 minutes.
GlycoNOE: CEST saturation (using 70 Gaussian pulses) placed before a semi-LASER spectroscopy sequence12: VOI of 15x15x15mm3, TE 40ms, acquisitions with voluntary respiratory synchronization in-vivo (TR 3500–4500ms), 2 or 3 averages per offset, 1200ms total saturation time, B1 = 1.04µT; 65 measurements with saturation offset from -4 to 4ppm (interleaved acquisitions for downfield and upfield saturation, plus 1 scan at -100ppm); acquisition time 8:40 min.
13C-MRS: pulse-and-acquire sequence with 2ms hyperbolic-secant-pulse, TR 600ms, 512 acquisitions, acquisition time 5:08 minutes.
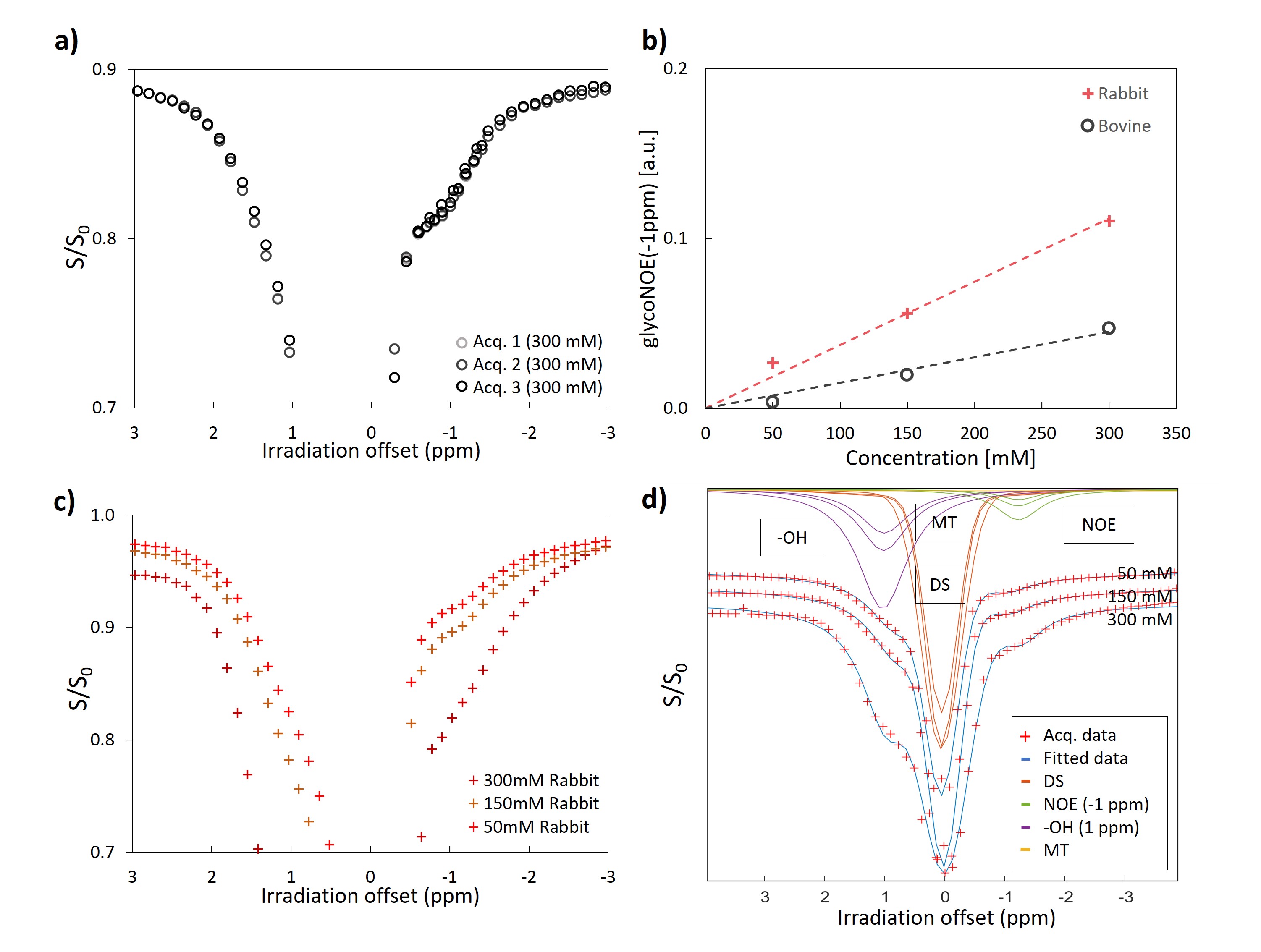
Data processed with jMRUI/AMARES13 to obtain Z-spectra as intensity of fitted water signal scaled by intensity at -100ppm. 4-pool fitting in Matlab (see Fig-1).
Results and Discussion
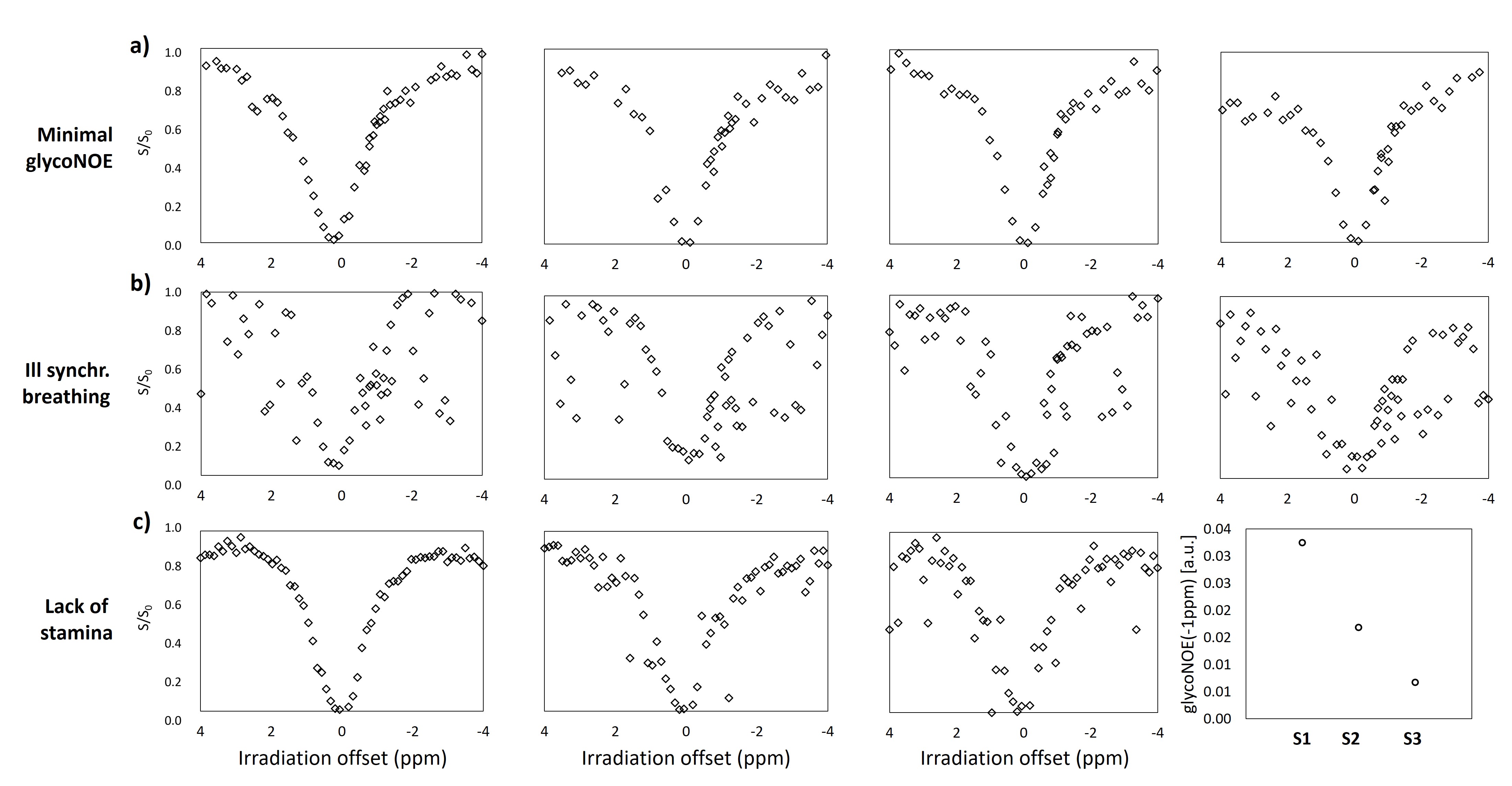
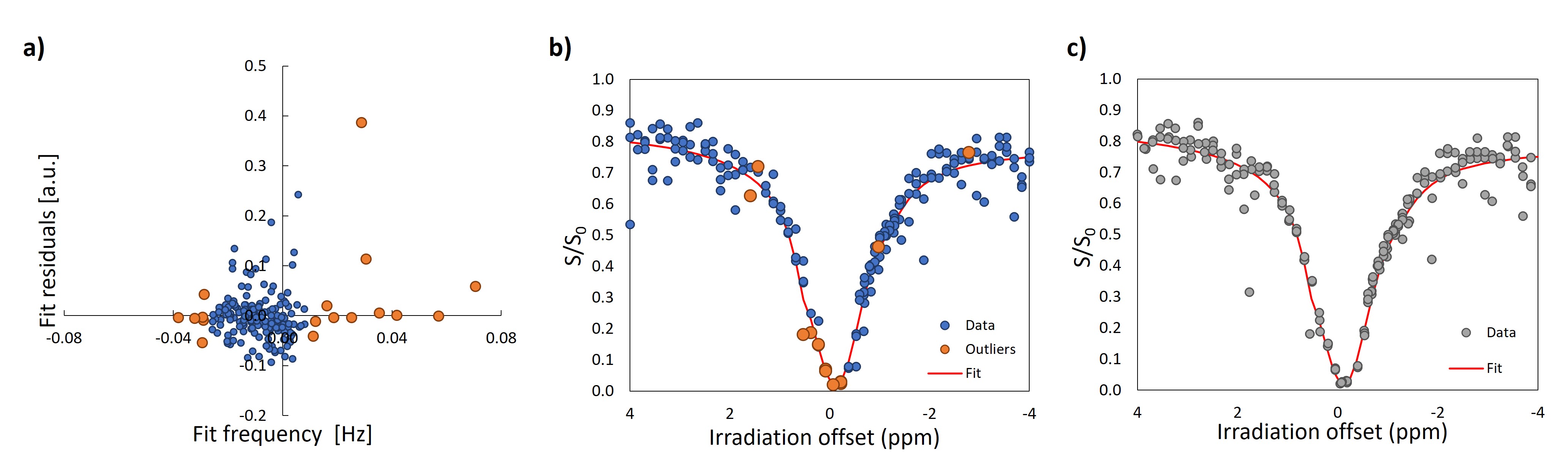
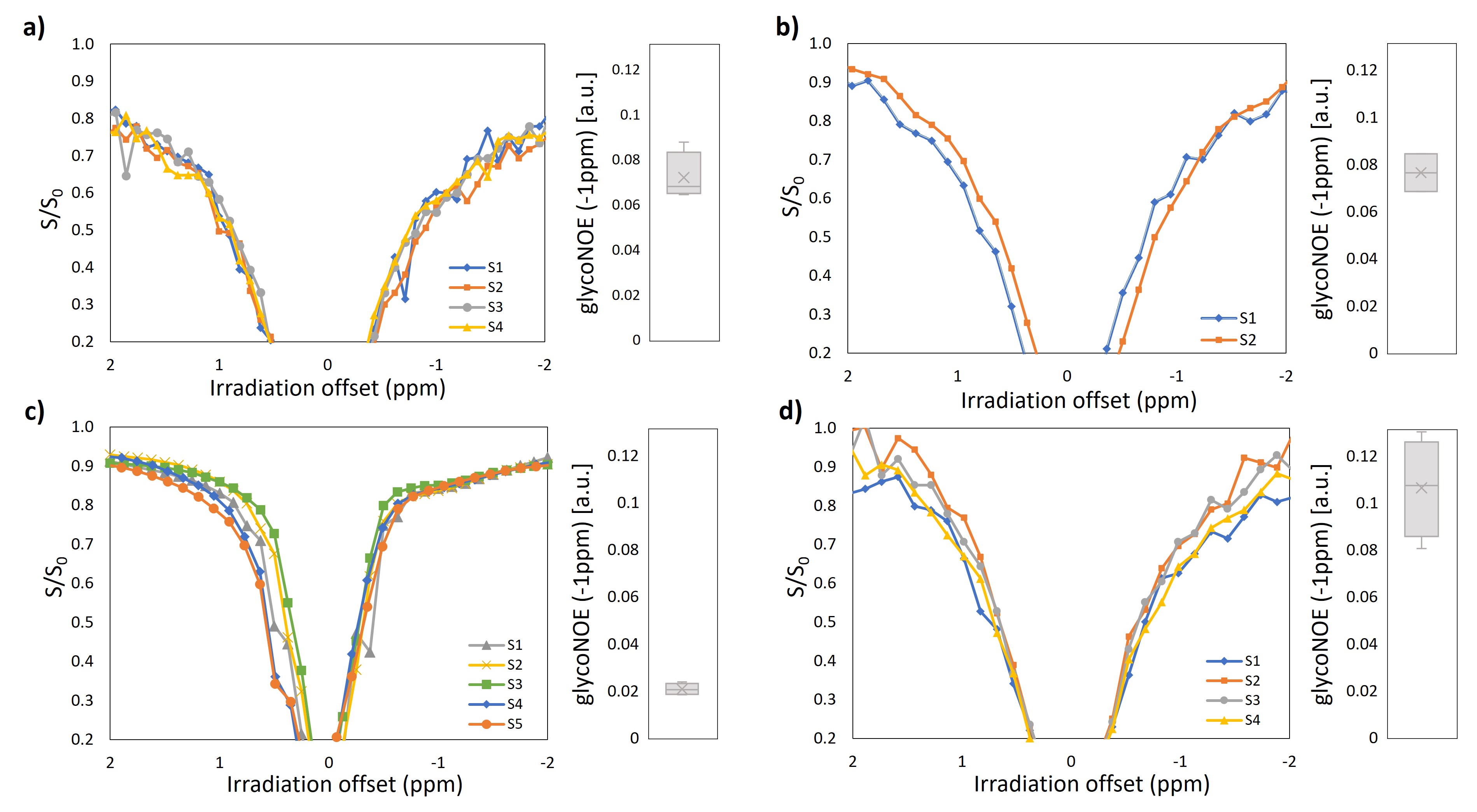
Fig-1 shows the in-vitro suitability of GlycoNOE at 7T for quantitative mapping of glycogen content. Repeatability is excellent (Fig-1a) and pool sizes scale linearly with concentration (Fig-1b). A 4-pool-fit readily distinguishes 3 components (Fig-1d), where at 7T NOE causes a 0.8ppm broad component at -1ppm, OH-CEST appears as 0.9ppm wide peak at +1ppm, both overlapping with the direct saturation peak, but without appreciable MT effect. As expected for a larger particle size with slower tumbling, the GlycoNOE pool is larger for rabbit ( ∼52 nm particle size) than for bovine glycogen (∼7 nm)11.Fig-2 and Fig-4 demonstrate the variability of outcomes for hepatic human GlycoNOE scans. Fig-2 contains examples of three common pitfalls. 1) lack of substantial NOE signal and occasional outlier signals possibly related to irregular breathing (Fig-2a); 2) no regular synchronized breathing with relaxed expiration position (Fig-2b); 3) intensity drift over time (Fig-2c). The use of knowledge of the water resonance frequency for each scan does not improve the outcome sufficiently (Fig-3). Fig-4 shows in-vivo results from 4 apparently (technically) successful acquisitions (success rate of 25% only), where stable results could be acquired in 2 to 5 repeated scans.
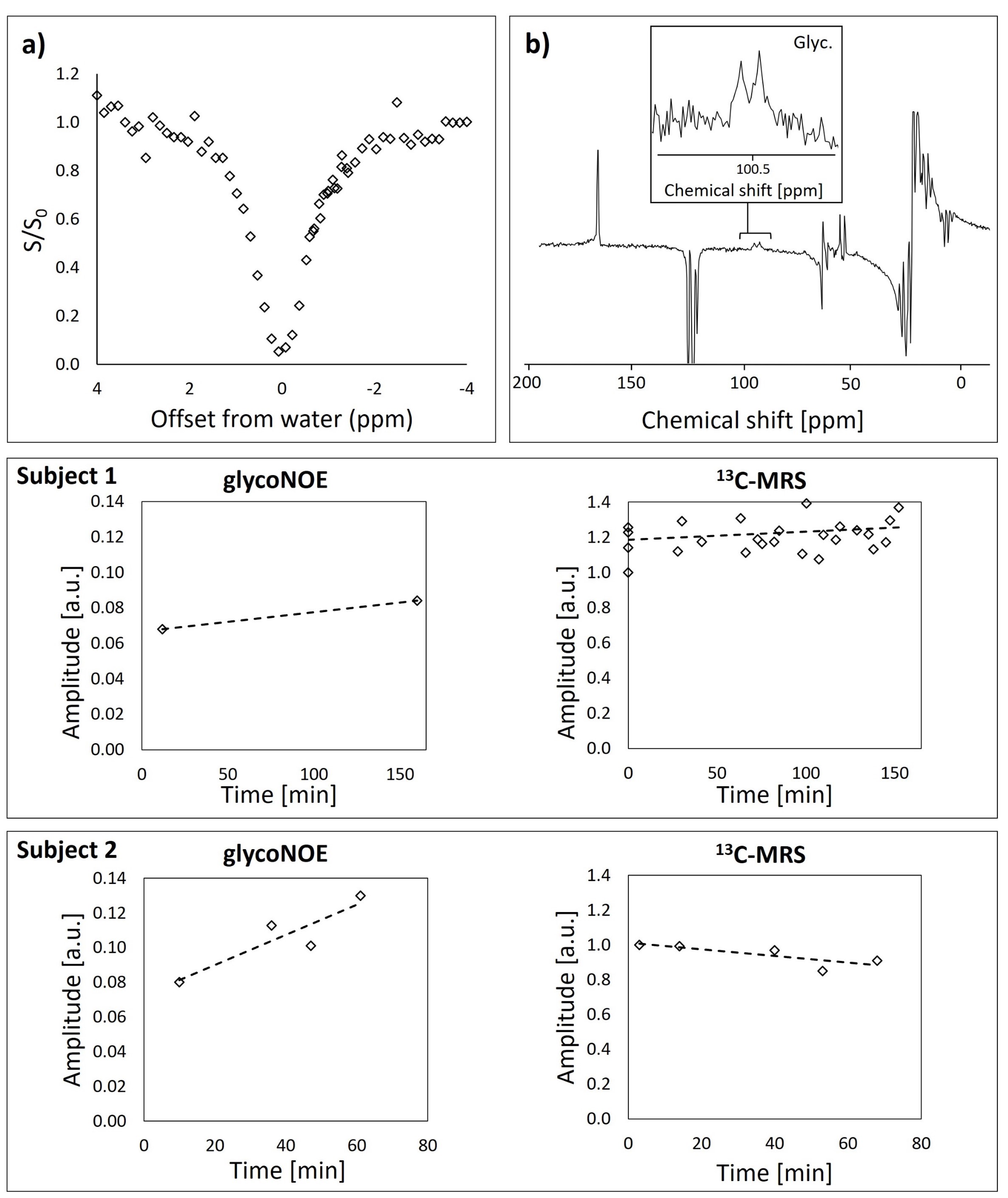
In Fig-5, glycogen levels determined by in-vivo glycoNOE are compared to those determined by 13C-MRS. If in subject-1 the increase in glycoNOE signal is in accordance with the course of the 13C-MRS glycogen signal, this is inconsistent in subject-2 despite the apparent technical success in both cases.
Conclusions
GlycoNOE is a valid tool for estimation of glycogen content in stationary situations but lacks robustness for investigation of hepatic glycogen in humans even in the optimized high-SNR situation of single voxel MRS with synchronized breathing, where the known resonance frequency of water during signal detection does unfortunately not characterize the saturation period sufficiently. Alternative outlier detection/correction using iterative fitting, the use of more restricted prior knowledge or most promisingly conversion to single-shot Z-spectrum acquisition16-19 may improve the robustness of the method.Acknowledgements
This project is supported by the Swiss National Science Foundation (PCEGP3_186978) and Diabetes Center Bern.References
[1] Petersen MC, Vatner DF, Shulman GI. Regulation of hepatic glucose metabolism in health and disease. Nat Rev Endocrinol. 2017;13(10):572-587.
[2] Adeva-Andany MM, González-Lucán M, Donapetry-García C, et al. Glycogen metabolism in humans. BBA Clin. 2016;5:85-100.
[3] Magnusson I, Rothman DL, Katz LD, et al. Increased rate of gluconeogenesis in type II diabetes mellitus. A 13C nuclear magnetic resonance study. J Clin Invest. 1992;90(4):1323-1327.
[4] Patlak CS, Blasberg RG, Fenstermacher JD. Graphical evaluation of blood-to-brain transfer constants from multiple-time uptake data. J Cereb Blood Flow Metab. 1983;3(1):1-7.
[5] Iozzo P, Geisler F, Oikonen V, et al. Insulin stimulates liver glucose uptake in humans: an 18F-FDG PET Study. J Nucl Med. 2003;44(5):682-689.
[6] Valette J, Tiret B, Boumezbeur F. Experimental strategies for in-vivo13C NMR spectroscopy. Anal Biochem. 2017;529:216-228.
[7] Ouwerkerk R, Pettigrew RI, Gharib AM. Liver Metabolite Concentrations Measured with 1H MR Spectroscopy. Radiology. 2012;265(2):565-575.
[8] Weis J, Kullberg J, Ahlström H. Multiple breath-hold proton spectroscopy of human liver at 3T: Relaxation times and concentrations of glycogen, choline, and lipids. J Magn Reson Imaging. 2018;47(2):410-417.
[9] van Zijl PCM, Jones CK, Ren J, at al. MRI detection of glycogen in-vivo by using chemical exchange saturation transfer imaging (glycoCEST). Proc Natl Acad Sci U S A. 2007;104(11):4359-4364.
[10] Miller CO, Cao J, Chekmenev EY, et al. Noninvasive measurements of glycogen in perfused mouse livers using chemical exchange saturation transfer NMR and comparison to (13)C NMR spectroscopy. Anal Chem. 2015;87(11):5824-5830.
[11] Zhou Y, van Zijl PCM, Xu X, et al. Magnetic resonance imaging of glycogen using its magnetic coupling with water. Proceedings of the National Academy of Sciences. 2020;117(6):3144-3149.
[12] Hoefemann M, Döring A, Fichtner ND, Kreis R. Combining chemical exchange saturation transfer and 1H magnetic resonance spectroscopy for simultaneous determination of metabolite concentrations and effects of magnetization exchange. Magnetic Resonance in Medicine. 2021;85(4):1766-1782.
[13] Stefan D, Cesare FD, Andrasescu A, et al. Quantitation of magnetic resonance spectroscopy signals: the jMRUI software package. Meas Sci Technol. 2009;20(10):104035.
[14] Zang LH, Howseman AM, Shulman RG. Assignment of the 1H chemical shifts of glycogen. Carbohydr Res. 1991;220:1-9.
[15] Chen W, Avison MJ, Zhu XH, Shulman RG. NMR studies of 1H NOEs in glycogen. Biochemistry. 1993;32(43):11483-11487.
[16] Xu X, Lee JS, Jerschow A. Ultrafast Scanning of Exchangeable Sites by NMR Spectroscopy. Angewandte Chemie-International Edition 2013;52(32):8281-8284.
[17] Döpfert J, Witte C, Schröder L. Slice-selective gradient-encoded CEST spectroscopy for monitoring dynamic parameters and high-throughput sample characterization. Journal of Magnetic Resonance 2013;237:34-39.
[18] Wilson NE, D'Aquilla K, Debrosse C, et al. Localized, Gradient-Reversed Ultrafast Z-Spectroscopy In Vivo at 7T. Magn Reson Med 2016;76(4):1039-1046.
[19] Zhang Y, Zu T, Liu RB, Zhou JY. Acquisition sequences and reconstruction methods for fast chemical exchange saturation transfer imaging. NMR Biomed 2023;36(6).
Figures