4460
Accelerating CEST-MRI for 3D renal imaging1Radiology, University of Texas Southwestern Medical Center, Dallas, TX, United States, 2Philips Healthcare, Gainesville, FL, United States, 3Advanced Imaging Research Center, University of Texas Southwestern Medical Center, Dallas, TX, United States, 4Philips Research, Hamburg, Germany
Synopsis
Keywords: CEST / APT / NOE, CEST & MT
Motivation: CEST-MRI is gaining recognition as a valuable tool for characterization of tumors and other ailments. However, its application in body imaging is still relatively limited. Specifically, applications to renal imaging are hampered by fat artifacts, motion, and limited coverage.
Goal(s): The goal of our work is to achieve reliable renal CEST MRI.
Approach: We are developing and compare acceleration of 3D GRE multi-point Dixon methods, to work in conjunction with timed breathing. The acquisition acceleration strategies include Compressed Sensing (CS) and CS with CASPR k-space sampling pattern.
Results: The developments allow expansion of the previous single-slice CEST MRI to a 3D whole-kidney coverage.
Impact: CEST-MRI for renal assessment will provide valuable information on kidney health and function, adding to existing multiparameteric MRI protocols, to serve as a molecular-level assessment of diseases, such as differentiation of renal cancers and acute renal failure.
INTRODUCTION
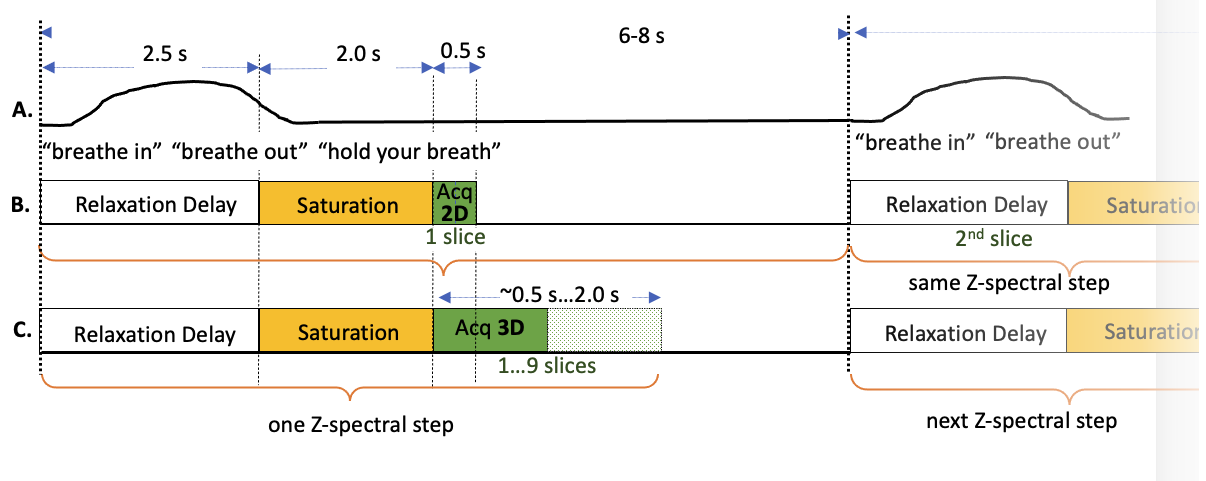
CEST MRI has gained recognition as a promising addition to the molecular and biomarkers imaging arsenal. CEST approaches that utilize the signatures from amide groups (Amide Proton Transfer-weighted, APT(1, 2), imaging), became a valuable tool in the assessment of brain malignancy(3-6). Still, a successful application of CEST as an imaging tool for renal imaging in general, and renal cancer in particular, has not yet been achieved. The translation of CEST techniques into a reliable assessment tool for renal ailments is hampered by the difficulties associated with general kidney imaging: contaminating fat signals, respiratory motion, limited coverage, and large B0 inhomogeneities. Here we are addressing two of these aspects: fast volumetric acquisition that also allows for a motion insensitive protocol. To this end, the acquisition employs timed breathing (Figure 1). Thus, the whole imaging volume, including saturation, needs to be collected within 6-8 sec, which was shown to be a comfortable breathing pattern. Previously, we have utilized a multi-slice 2D multi-point Dixon(7). Here, we extend the previous work to a 3D acquisition, combining it with Compressed SENSE (CS) acceleration. Different k-space sampling patterns, including Cartesian (CS) and CS+CASPR (Cartesian Acquisition with Spiral Profile Reordering(8)) are employed. The results are compared in terms of image quality and 3D coverage.METHODS
3T MRI (Ingenia, Philips Healthcare) equipped with dual transmit body coil for transmit and 28-channel abdominal array for receive was utilized for the study. Eleven volunteers without kidney ailments were recruited so far for this IRB-approved study. For image acquisition, a 3D TFE single shot multi-point Dixon acquisition sequences were implemented. For CEST saturation we used: 40x50 msec pulses, for a total saturation length of 2 sec, enabled by alternated parallel transmission, B1rms=1.17 μT, and 15 points in the Z-spectrum [±7 ppm] or [±10 ppm]. Here, two different variants of the 3D acquisition are discussed: (i) CS (n=10); (ii) CS+CASPR (n=1). . Other acquisition parameters were FOV=360x300, voxel size 3x3 mm2, slice thickness = 5mm, number of slices varied from 3 to 9. Single shot acquisition included 3 echo Dixon with TR/TE1/DTE = 3.4/1.04/0.6 msec. Acquisition length varied depending on the acquisition scheme, the TFE length was adjusted to be minimum number accommodating the whole 3D acquisition for a given scheme and acceleration. The CEST processing was done on the pixel-by-pixel basis using custom Matlab codes. The processing utilized water-only images, followed by motion correction using SNMI registration, B0 correction using minimum of Z-spectra and standard MTRasym calculation.RESULTS
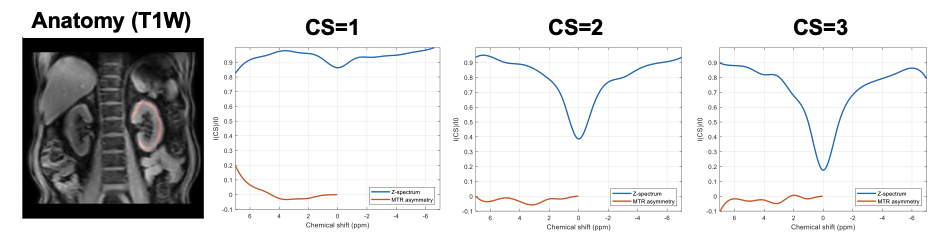
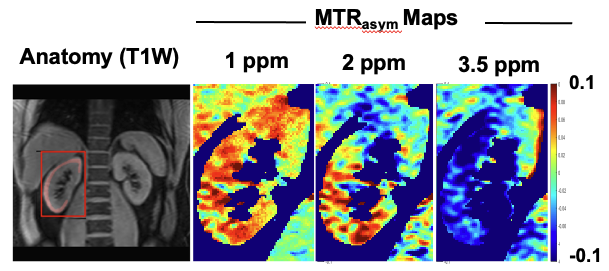
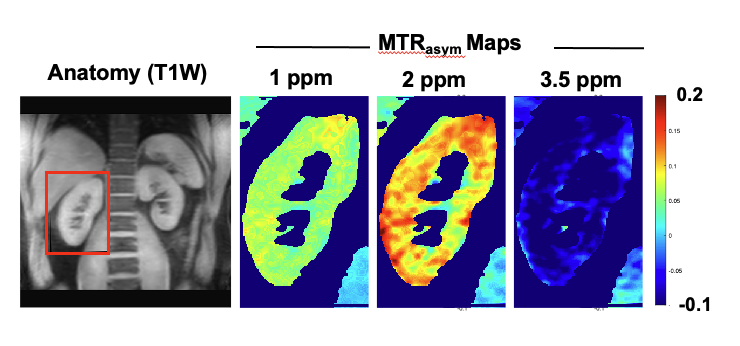
Using the timed breathing scheme shown in Figure 1, along with auditory coaching from the scanning technologist, allowed for comfortable breathing patterns that were well tolerated. Switching to 3D allows acquisition of up to 5 slices within 6 to 7 sec breathing pattern. However, single shot acquisition of non-accelerated 3D leads to prohibitively long acquisition time and loss of CEST saturation. This is illustrated in Figure 2. Here, CS=1, 2 and 3 led to single shot factors/TFE shot acquisition time of 525/1,783 msec, 240/815 msec, 120/408 msec. The CEST contrast loss occurs due to T1 influence and Z-magnetization recovery during acquisition. Using CS allowed for significant reduction of the acquisition train lengths such that the loss of CEST effect was not signitifcant. Importantly, CS did not result in the generation of significant artifacts, as can be appreciated in Figure 3. CS was also combined with CASPR pattern. The results are shown in Figure 4. The combination allowed acquisition of 9 slices in the single shot with shot length 224/759 msec.DISCUSSION
The results demonstrate that acceleration is needed for renal 3D volumetric CEST not only for motion, but for the maximum CEST possible. 3D CS CASPR readout resulted in the maximum number of slices, 9, covering 4.5 cm of kidney. The CEST effect was more consistent across the kidney. Thus, the whole kidney coverage within a single shot is feasible. While the 3D CASPR readout adds to a motion-insensitive acquisition of any of the single RF-offset frames of the Z-spectrum, there was still a need to correct through-frame motion artifacts by post-processing registration. Additional testing and modifications of the acquisition, such as combination with Turbo Spin Echo is underway. Moreover, advanced noise reduction using AI algorithms, as well as different CEST quantification, such as multi-peak Lorentzian fit, may further improve quality of CEST and are currently investigated.CONCLUSION
Acceleration is necessary to achieve 3D kidney CEST-MRI. CS using advanced motion-insensitive k-space trajectory (CASPR) allows for whole-kidney CEST imaging, that comfortably fits with the breathing pattern in normal volunteers. Evaluation of this technique in kidney cancer patients is forthcoming.Acknowledgements
The work is supported, in part, by the NIH grant R01CA252281.References
1. J. Zhou, B. Lal, D. A. Wilson, J. Laterra, P. C. van Zijl, Amide proton transfer (APT) contrast for imaging of brain tumors. Magn Reson Med 50, 1120-1126 (2003).
2. J. Zhou, J.-F. Payen, D. A. Wilson, R. J. Traystman, P. C. M. van Zijl, Using the amide proton signals of intracellular propteins and peptides to detect pH effects in MRI. Nat. Med. 9, 1085-1090 (2003).
3. J. Zhou et al., Differentiation between Glioma and Radiation Necrosis using Molecular Magnetic Resonance Imaging of Endogenous Proteins and Peptides. Nat. Med. 17, 130-134 (2011).
4. J. Zhou et al., Practical data acquisition method for human brain tumor amide proton transfer (APT) imaging. Magn Reson Med 60, 842-849 (2008).
5. O. Togao et al., Amide proton transfer imaging of adult diffuse gliomas: correlation with histopathological grades. Neuro Oncol 16, 441-448 (2014).
6. K. Sagiyama et al., In vivo chemical exchange saturation transfer imaging allows early detection of a therapeutic response in glioblastoma. Proc Natl Acad Sci U S A 111, 4542-4547 (2014).
7. E. Vinogradov et al. (2015) Endogenous Urea CEST (urCEST) for MRI monitoring of kidney function. in International Society for Magnetic Resonance in Medicine (Toronto).
8. J. S. Greer et al., Robust pCASL perfusion imaging using a 3D Cartesian acquisition with spiral profile reordering (CASPR). Magn Reson Med 82, 1713-1724 (2019).
Figures