4444
A unified framework of tumor segmentation and response assessment in patients with malignant gliomas using structural and APT-weighted MRI1Department of Radiology, Johns Hopkins University, Baltimore, MD, United States, 2Department of Computer Science, Johns Hopkins University, Baltimore, MD, United States, 3Department of Electrical and Computer Engineering, Johns Hopkins University, Baltimore, MD, United States, 4Department of Applied Mathematics and Statistics, Johns Hopkins University, Baltimore, MD, United States, 5Department of Biomedical Engineering, Johns Hopkins University, Baltimore, MD, United States
Synopsis
Keywords: CEST / APT / NOE, CEST & MT
Motivation: Amide protein transfer-weighted (APTw) MRI has been validated to accurately detect recurrent malignant gliomas across different studies. However, APTw image interpretation is time consuming and requires professional knowledge.
Goal(s): Our goal was to develop a reliable, automated imaging diagnostic tool to assess malignant glioma response to therapies are urgently needed.
Approach: We developed and verified a unified CNN-based deep-learning framework for both tumor segmentation and tumor progression assessment by adding APTw MRI data to structural MR images as model input.
Results: The use of APTw images can improve not only diagnostic accuracy but also segmentation performance to structural MRIs.
Impact: The proposed deep-learning method could be a highly efficient solution that could help clinical experts to make precise diagnoses for patients with post-treatment gliomas.
Introduction
Amide proton transfer-weighted (APTw) imaging is a chemical exchange saturation transfer (CEST)-based molecular MRI technique. Several research groups have confirmed that APTw hyperintensity is a reliable imaging marker of recurrent malignant glioma1-6. However, APTw image interpretation is time consuming and requires professional knowledge and automated reliable analysis would be important for its general accessibility in the clinic. Advances in artificial intelligence and computer vision have achieved powerful solutions for improving medical imaging techniques and automatic diagnosis7-10. Here, we developed and verified a unified CNN-based deep-learning framework for both tumor segmentation and tumor progression identification by adding APTw MRI data to structural MR images as model input. The goal was to evaluate the power of APTw images in the deep-learning algorithm for both tumor segmentation and classification of treatment effect and tumor recurrence in post treatment malignant gliomas.Methods
MRI protocolAll patients were scanned on a Philips 3T MRI system. The sequences performed for each patient included T1w, T2w, FLAIR, APTw, and gadolinium contrast-enhanced T1w (Gd-T1w). A 3D imaging acquisition scheme was used for volumetric APTw imaging. APTw images were calculated using the magnetization transfer ratio asymmetry at 3.5ppm offset from the water frequency. All MR images were resampled to a spacing of 0.5×0.5×2.0 mm. Normalization, bias correction and co-registration were applied.Patients
A total of 117 MRI scans from 81 patients post-treated malignant gliomas were re-assessed. All patients underwent MRI studies after the chemoradiotherapy completion. Each scan was annotated as “response" to treatment or “progressive disease", according to the RANO criteria11. All the imaging datasets have also been pixel-wise annotated manually following the same annotation protocol in BraTs Challenge12. Pixel-wise annotations comprise the Gd-enhancing tumor (ET), the non-enhancing tumor region (NER), and the peritumoral edematous/invaded tissue (Edema).
Unified Deep-learning Segmentation and Classification Framework
The proposed framework was built on the U-net backbone13 and trained using a using a dual branch (DB) paradigm with both pixel-level and scan-level supervision. The U-net backbone is designed to output the progression-aware segmentation map that further divide ET and NER into stable, improved or increasing regions. Then, the proposed classification branch is added to predict the probability of tumor recurrence based on the volumetric ratio of increasing ET and NER. Finally, a label merging process is applied to initial segmentation map to enable supervised learning using manually annotated ground truth for the segmentation branch. Fig. 1 presents the overview of the proposed tumor recurrence classification framework. To further assess the added value of APTw images, we separated our experiments into two main groups: without APTw (only structural MRIs as input) and with APTw (both structural and APTw MRIs). The whole imaging dataset was split into 70%, 10%, and 20% for training, validation, and testing datasets in a chronological order (the MRI acquisition date). The AUC of tumor recurrence classification and volumetric and distance metrics of tumor sub-region segmentation were evaluated for all scans in the testing datasets.
Results
For the response assessment, the proposed model without APTw images as input achieved an AUC of 0.92 (sensitivity, 0.88; specificity, 0.90). By adding the APTw images to the framework input, the classification performance improved to AUC 0.94 (sensitivity, 0.92; specificity, 0.99). For the brain tumor segmentation performance, an improvement was also observed by comparing the result with and without APTw images (Table 1). Interestingly, the Dice coefficient increased the most for the tumor core region from 0.68 to 0.71, suggesting that APTw imaging can help to distinguish tumor boundary. In this study, pairs of models using data with and without APTw MRI were compared to explore the added value of APTw MRI to structural MRIs.Table 1. Quantitative brain tumor sub-region segmentation results of models with and without APTw images. HD95: 95% Hausdorff distance, ASD: Average Surface Distance. The “Whole Tumor” describes the entire extent of the disease (ET, NER and Edema). The “Tumor Core” entails the ET and NER part of the tumor.
| | Whole Tumor (ET+NER+Edema) | Tumor Core (ET+NER) | Enhancing Tumor (ET) | ||||||
| | Dice | HD95 | ASD | Dice | HD95 | ASD | Dice | HD95 | ASD |
| w/ APTw | 0.87 | 6.03 | 1.40 | 0.71 | 9.72 | 3.50 | 0.65 | 7.28 | 1.93 |
| w/o APTw | 0.86 | 6.49 | 1.41 | 0.68 | 9.99 | 3.64 | 0.64 | 10.95 | 1.86 |
Conclusion
The proposed framework utilizing multi-parametric MRIs showed promising results in tumor progression detection and brain tumor segmentation. The AUC of our best-performing model were 0.94 for scan-level classifications with a specificity of 0.99. Based on this performance, the proposed method could be a highly efficient solution for clinical experts to make precise diagnoses for patients with post-treatment malignant gliomas and further prognosis analysis.Acknowledgements
This work was supported in part by grants from the National Institutes of Health (R01CA228188, R01CA0276221 and R37CA248077).
References
1.Park YW, et al. Differentiation of recurrent diffuse glioma from treatment-induced change using amide proton transfer imaging: incremental value to diffusion and perfusion parameters. Neuroradiology 2020.
2. Park JE, et al. Identification of Early Response to Anti-Angiogenic Therapy in Recurrent Glioblastoma: Amide Proton Transfer–weighted and Perfusion-weighted MRI compared with Diffusion-weighted MRI. Radiology 2020;295(2):397-406.
3. Regnery S, et al. Chemical exchange saturation transfer MRI serves as predictor of early progression in glioblastoma patients. Oncotarget 2018; (9):28772-28783.
4. Paech D, et al. Relaxation-compensated amide proton transfer (APT) MRI signal intensity is associated with survival and progression in high-grade glioma patients. Eur Radiol. 2019 Sep;29(9):4957-4967.
5. Jiang S, et al. Identifying recurrent malignant glioma after treatment using amide proton transfer-weighted MR imaging: A validation study with image-guided stereotactic biopsy. Clin Cancer Res. 2019;25:552-561.
6. Zhou J, et al. Review and consensus recommendations on clinical APT-weighted imaging approaches at 3T: Application to brain tumors. Magn Reson Med. 2022;88:546-74.
7. Eijgelaar RS, et al. Robust Deep Learning-based Segmentation of Glioblastoma on Routine Clinical MRI Scans Using Sparsified Training. Radiology Artificial intelligence 2020;2(5):e190103.
8. Cohen O, et al. Rapid and quantitative chemical exchange saturation transfer (CEST) imaging with magnetic resonance fingerprinting (MRF). Magn Reson Med. 2018;80(6):2449-2463.
9. Glang F, et al. DeepCEST 3T: Robust MRI parameter determination and uncertainty quantification with neural networks-application to CEST imaging of the human brain at 3T. Magn Reson Med. 2020;84(1):450-466.
10. Li M, et al. DC-AL GAN: Pseudoprogression and true tumor progression of glioblastoma multiform image classification based on DCGAN and AlexNet. Med Phys 2020;47(3):1139-1150.
11. Wen PY, et al. Updated response assessment criteria for high-grade gliomas: response assessment in neuro-oncology working group. J Clin Oncol. 2010;28:1963-1972.
12. Baid U, et al. The RSNA-ASNR-MICCAI BraTS 2021 Benchmark on Brain Tumor Segmentation and Radiogenomic Classification. arXiv:2107.02314, 2021.
13. Olaf R, et al. U-net: Convolutional networks for biomedical image segmentation. MICCAI 2015.
Figures
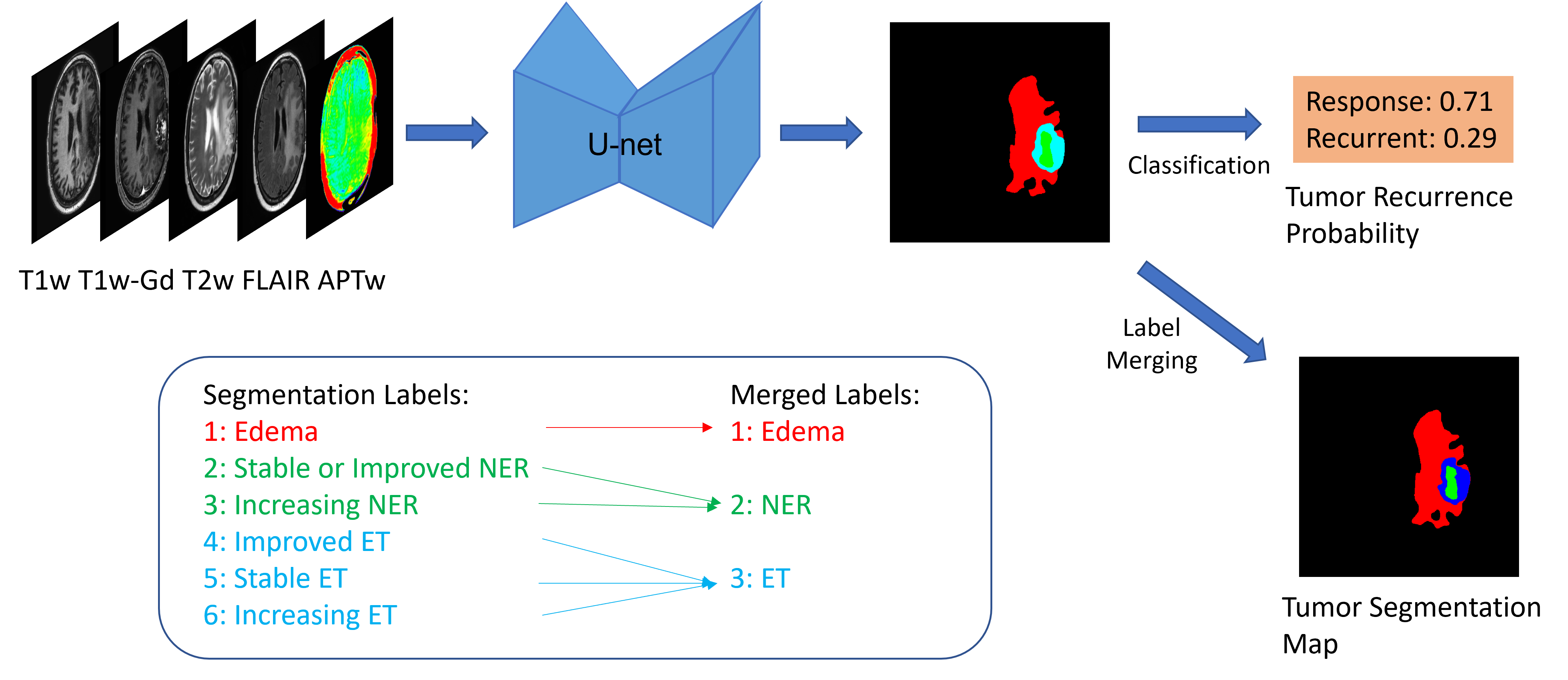
Figure 1. Overview of the proposed deep-learning pipeline, which consists of a U-net segmentation backbone that takes multi-modal data as input, a classification branch for tumor recurrence and segmentation branch for tumor segmentation. A label merging process is applied to initial segmentation map to enable supervised learning using manually annotated ground truth for the segmentation branch.
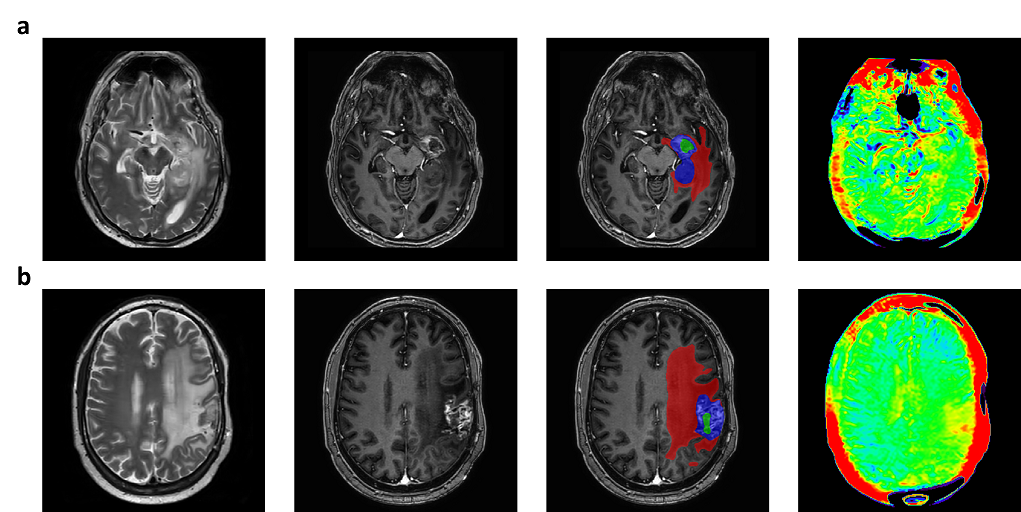
Figure 2. Columns from left to right: T2w, Gd-T1w, Gd-T1w overlaid with predicted segmentation map, and APTw images. (a) (b) correspond to patient annotated as “Response” and “Recurrent” respectively.