4420
Alterations in the Pain-Related Functional Matrix among RCVS Patients during Resting-State fMRI.1Department of Radiology, Taipei Veterans General Hospital, Taipei, Taiwan, 2National Yang-Ming Chiao Tung University, Department of Biomedical Imaging and Radiological Sciences, Taipei, Taiwan, 3Department of Medical Imaging and Radiological Technology, Yuanpei University of Medical Technology, Hsinchu, Taiwan, 4School of Medicine, College of Medicine, National Yang-Ming Chiao Tung University, Taipei, Taiwan
Synopsis
Keywords: Functional Connectivity, Brain Connectivity
Motivation: Reversible cerebral vasoconstriction syndrome (RCVS) is a severe headache condition marked by recurrent explosive headaches. We investigate changes in the functional connectivity of brain regions associated with pain matrix in both RCVS patients and healthy controls.
Goal(s): Our hypothesis the functional connectivity mechanisms underlying pain processing differ between two groups.
Approach: We utilizing rs-fMRI imaging with graph theory analysis.
Results: The findings contribute to a more profound comprehension of the activation processes occurring within brain regions responsible for pain perception RCVS patients.We ascertain whether the mechanisms of pain processing in RCVS patients deviate from those observed in healthy controls.
Impact: We utilizing rs-fMRI imaging with graph theory to investigate functional connectivity mechanisms of pain matrix. The findings contribute comprehension of the activation processes occurring within brain regions responsible for pain perception RCVS patients deviate from those observed in healthy controls.
Purpose
Reversible cerebral vasoconstriction syndrome (RCVS) is a severe headache condition characterized by recurrent explosive headaches, often referred to as thunderclap headaches, and reversible segmental vasoconstriction seen in angiography. The underlying pathophysiology of RCVS remains unclear. This study aims to investigate changes in the functional connectivity of pain-related brain regions in RCVS patients and their impact on subjective health. Recent advances in neuroimaging, specifically graph theory applied to resting-state fMRI data, allow us to assess the brain's functional connectivity as a highly efficient large-scale network of nodes (brain regions) and pairwise edges. This network exhibits a clustered structure, often termed a "small-world" network. Evidence from cohort studies suggests that lower small-worldness values are linked to poorer performance in neuropsychological tasks. This study explores the mechanisms of pain processing through functional connectivity, using rs-fMRI and graph theory. Our hypothesis is that functional connectivity mechanisms in pain processing differ between RCVS patients and healthy controls.Methods
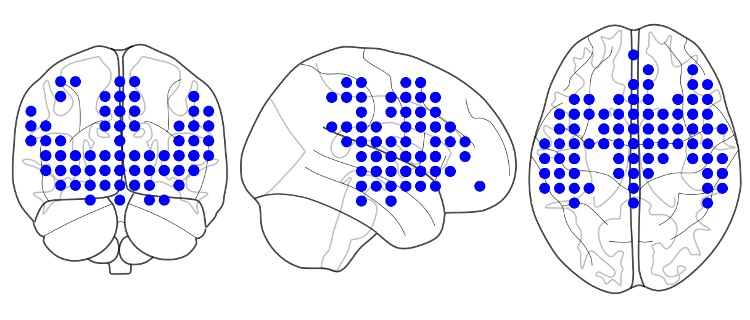
We studied 91 participants, including RCVS patients (23 male, 24 female, average age 45.94 ± 9.71) and healthy controls (22 male, 22 female, average age 40.00 ± 8.27), based on clinical evaluations. We used a 3.0T MRI scanner (General Electric Discovery MR750) with an 8-channel head coil for data collection. Resting-state fMRI (rs-fMRI) data were acquired with a gradient EPI sequence (TR = 2500 ms, TE = 30 ms, flip angle = 90°, FOV = 240 mm × 240 mm, matrix = 64 × 64, 45 slices, slice thickness = 3.5 mm). 3D T1-weighted image was acquired for co-registration and normalization (axial acquisition, TR = 7.8 ms, TE = 3.0 ms, TI = 450 ms, flip angle = 13°, FOV = 256 mm × 256 mm, matrix = 256 × 256, 180 slices, slice thickness = 1.0 mm). Data were preprocessed using the Data Processing Assistant for rs-fMRI toolbox. In the 200 volumes, the initial 5 volumes were excluded for subject adaptation and magnetization stabilization. Slice-timing correction and realignment addressed timing differences and head movement. Co-registration to structural images and spatial normalization to the MNI template were performed, and voxels were resampled to 2 mm isotropic. Images were smoothed with a 6 mm FWHM isotropic Gaussian kernel, and a linear trend and bandpass filter were applied for noise reduction. Six motion parameters, white matter signal, and CSF signal were extracted as covariates.To investigate resting-state brain activity differences, we conducted seed-based correlation analysis (SCA) using 159 predefined seed regions related to pain processing. We employed the graph theory analysis tool BRAPH to assess global and local network characteristics, including average degree, characteristic path length, mean clustering coefficient, global and local efficiency, strength, node efficiency, and node centrality. Statistical analysis was conducted using SPSS 17, with significance set at p < 0.05Results
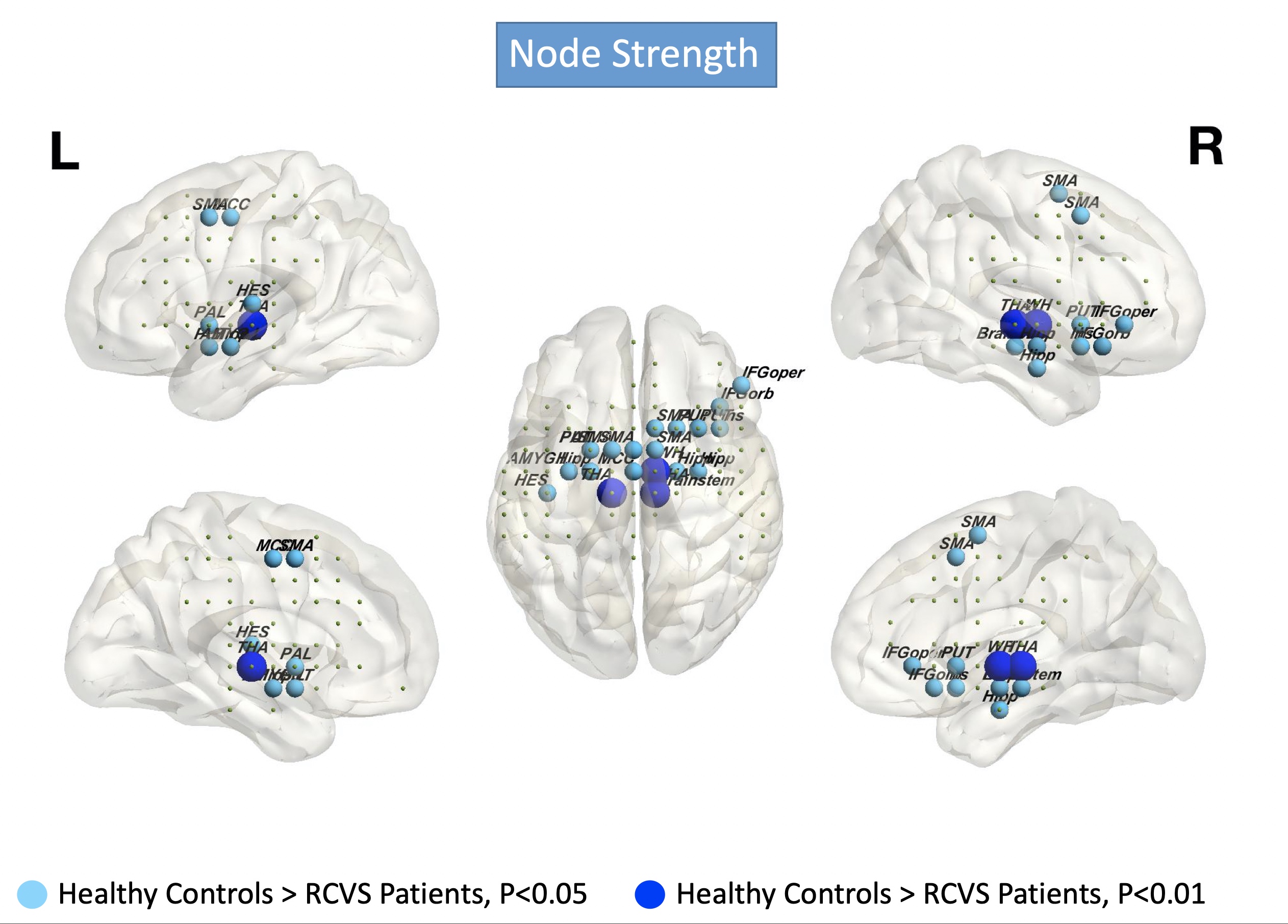
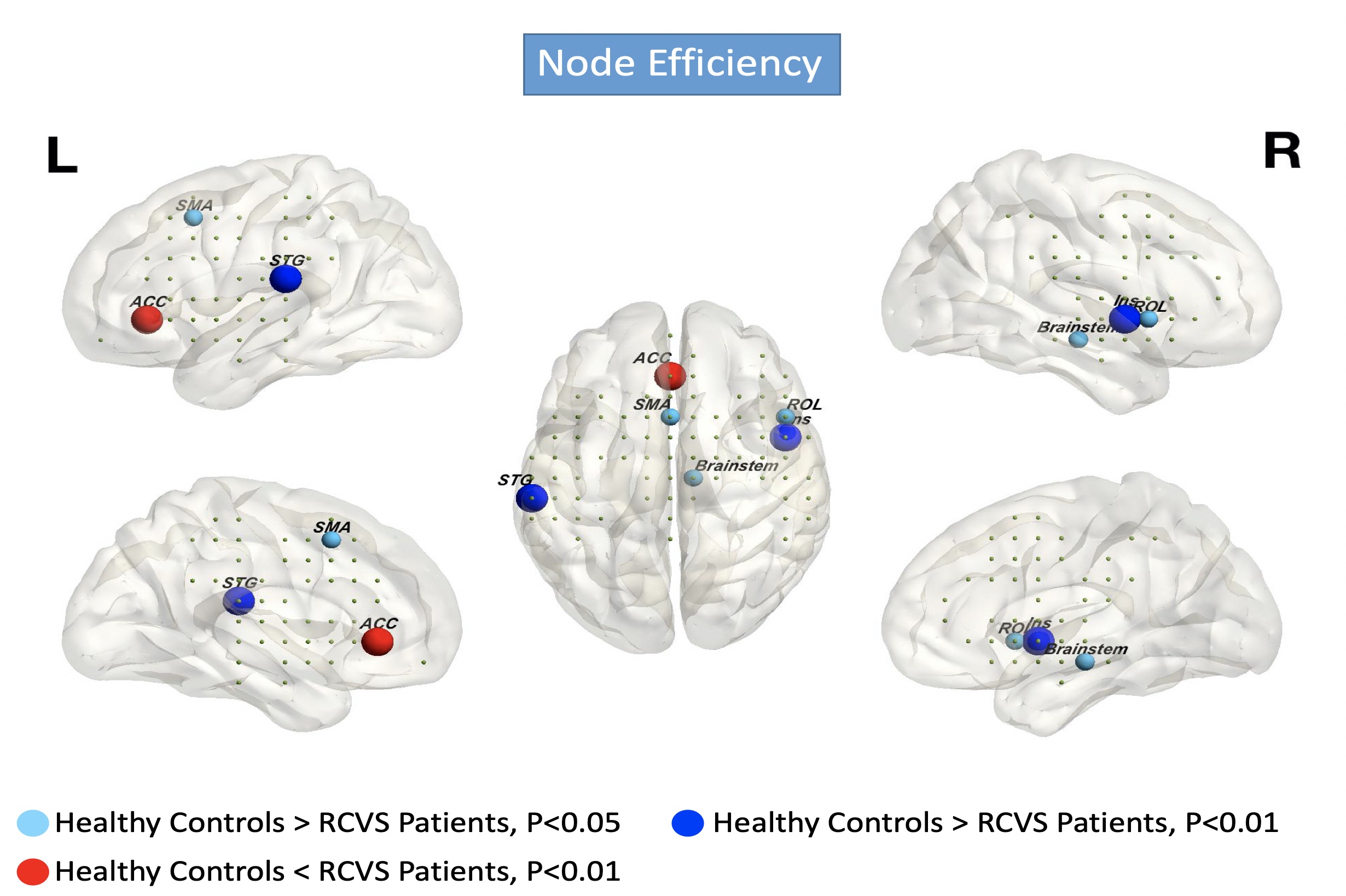
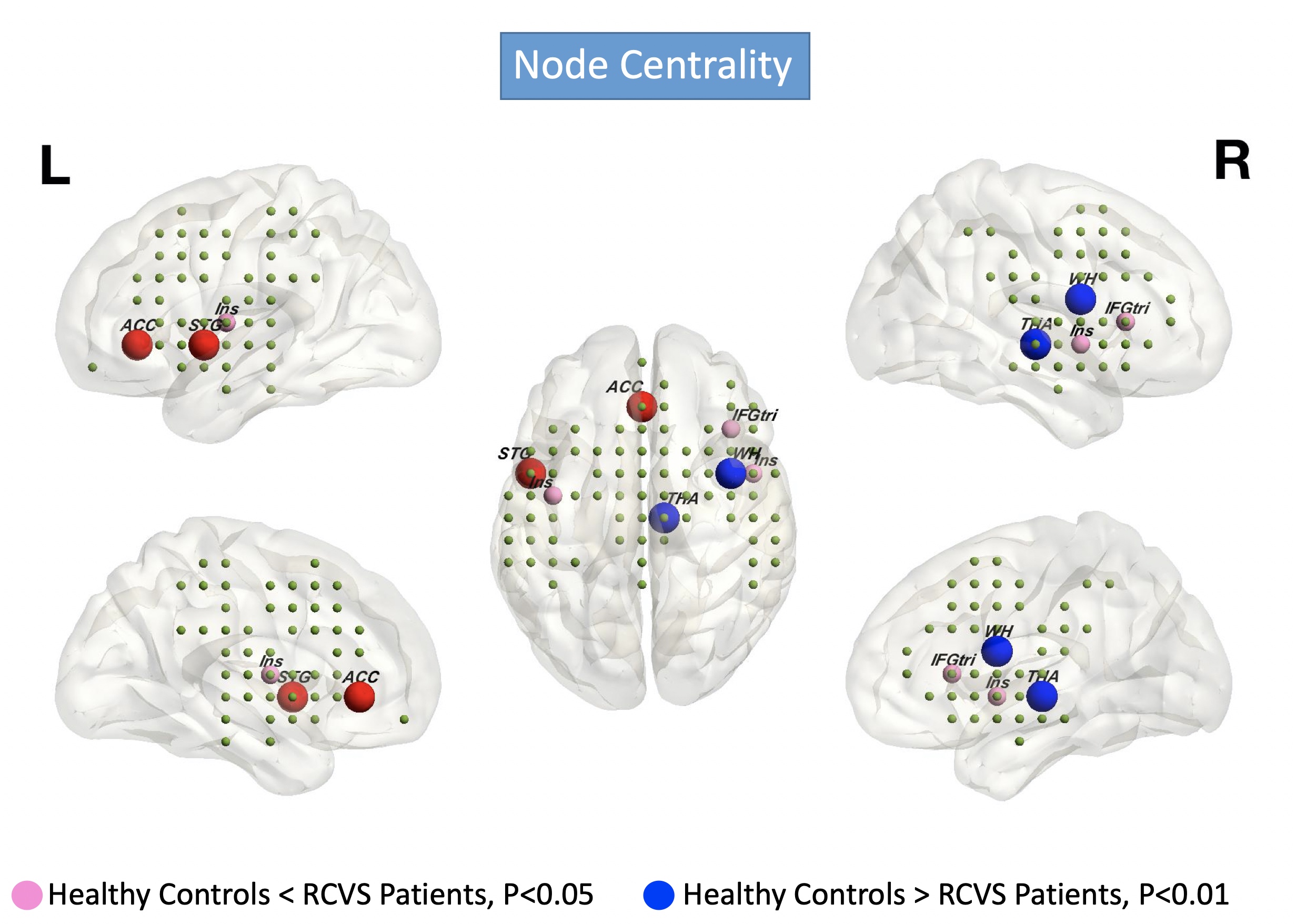
In the global network's topology, there was no significant difference in the pain matrix network between RCVS patients and HC. However, in the local network's topology (as depicted in Figure 2), it is evident that there are variations in the strength of brain node connections. These variances are observed in areas such as the frontal temporal lobe (including Frontal Inferior operculum, Amygdala, Heschl's area, Hippocampus, Inferior Frontal Gyrus Orbital, Insula, Middle Cingulate Cortex), the parietal lobe (specifically Supplementary Motor Areas), and central neuronal regions (Brain stem, Pallidum, Putamen, Thalamus). Notably, all HC exhibited stronger connections compared to RCVS patients. When considering node efficiency (as shown in Figure 3), RCVS patients displayed greater efficiency in processing pain in the Anterior Cingulate Cortex compared to HC. Conversely, HC showed higher efficiency in other areas, including the Brainstem, Insula, Rolandic Operculum, Supplementary Motor Areas, and Temporal superior Gyrus. In terms of node centrality (as presented in Figure 4), RCVS patients exhibited higher centrality of pain nodes in the Anterior Cingulate Cortex, Temporal superior Gyrus, Frontal Inferior Triangular, and Insula, as opposed to HC, where Thalamus and white matter showed higher centrality.Discussion and Conclusion:Discussion and Conclusion
The primary discovery in this study is the absence of significant differences in the connectivity of pain processing regions across all brain regions between RCVS patients and healthy subjects. Notably, we also unveil a novel insight into the reconfiguration of nodes within various brain networks in RCVS patients. Our objective in this research is to gain a deeper understanding of the activation mechanisms within pain-related brain regions in RCVS patients. We aim to determine whether the pain processing mechanisms in RCVS patients differ from HC.Acknowledgements
No acknowledgement found.References
1. Ducros A. Reversible cerebral vasoconstriction syndrome. The Lancet Neurology 2012;11:906-917.
2. Peyron R, Laurent B, Garcia-Larrea L. Functional imaging of brain responses to pain. A review and meta-analysis (2000). Neurophysiologie Clinique/Clinical Neurophysiology 2000;30:263-288.
3. Apkarian AV, Bushnell MC, Treede R-D, Zubieta J-K. Human brain mechanisms of pain perception and regulation in health and disease. European journal of pain 2005;9:463-484.
4. Davis KD. The neural circuitry of pain as explored with functional MRI. Neurological research 2000;22:313-317.
5. Medaglia JD. Graph theoretic analysis of resting state functional MR imaging. Neuroimaging Clinics 2017;27:593-607.
6. Wang J, Zuo X, He Y. Graph-based network analysis of resting-state functional MRI. Frontiers in systems neuroscience 2010;4:1419.
7. Yan C-G, Wang X-D, Zuo X-N, Zang Y-F. DPABI: data processing & analysis for (resting-state) brain imaging. Neuroinformatics 2016;14:339-351.
8. Flodin P, Martinsen S, Altawil R, et al. Intrinsic brain connectivity in chronic pain: a resting-state fMRI study in patients with rheumatoid arthritis. Frontiers in human neuroscience 2016;10:107.
Figures