4419
Regional impairments in cerebrovascular reactivity in Fontan patients: fMRI CO2 challenge1Department of Biomedical Engineering, University of Southern California, Los Angeles, CA, United States, 2Cardiology, Children's Hospital Los Angeles, Los Angeles, CA, United States, 3Ming Hsieh Department of Electrical and Computer Engineering, University of Southern California Viterbi School of Engineering, Los Angeles, CA, United States, 4Institute of Imaging Science, Vanderbilt University, Nashville, TN, United States, 5Pediatric Neurosurgery, Children's Hospital Los Angeles, Los Angeles, CA, United States, 6Pediatrics CHLA, Keck School of Medicine of USC, Los Angeles, CA, United States
Synopsis
Keywords: fMRI Analysis, fMRI (resting state), Fontan, cerebrovascular reserve, CVR, BOLD
Motivation: Despite their high risk for cerebral injuries and neurocognitive deficits, cerebrovascular health in single ventricle heart disease (SVHD) patients is understudied.
Goal(s): Quantifying cerebrovascular reserve (CVR) in SVHD patients will determine the susceptibility of these patients to acute interruptions in oxygen delivery or increased metabolic demand.
Approach: In this study, we used blood oxygenation level-dependent BOLD-MRI under CO2 challenge to measure CVR in patients who underwent Fontan palliation and in control subjects.
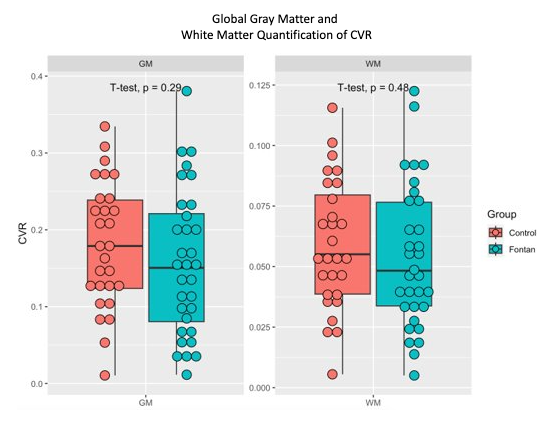
Results: Regional, but not global differences, were shown in CVR between Fontan versus healthy controls.
Impact: An important prognostic indicator of cerebrovascular integrity is the ability of blood vessels to dilate or constrict in response to a stimulus, measured by CVR. Therefore, quantifying CVR in SVHD patients will determine their susceptibility to increased metabolic demands.
Introduction
Single ventricular heart disease (SVHD) can occur due to congenital ventricular underdevelopment, anatomical valve absence, or lack/loss of contractility. SVHD patients require three corrective surgeries to optimize oxygenated blood delivery to the brain1,2. The final stage, Fontan palliation, causes all systemic blood blow to pass through the lungs without ventricular assistance, yielding increased risk for cerebral injury3,4. A key indicator of cerebrovascular health is cerebrovascular reactivity (CVR): the ability of blood vessels to dilate/constrict in response to stimulus5. Impairment of CVR increases the risk posed by fluctuations in oxygen delivery or increased metabolic demand. Current literature is scarce with regard to CVR response in SVHD patients. In this work, we used blood oxygenation level-dependent BOLD-MRI under CO2 challenge to measure CVR in patients who underwent Fontan repair and in controls.Methods
Participants: 32 Fontan patients (FP, age=20.5±2.3 y; Hb=15.8±2.1; Hct=47.7±4.7; F=11) and 28 control subjects (CTL, age=22.2±4.2 y; Hb=14.3±1.5; Hct=43.3±4.1; F=12).Neuroimaging data: MRI data were acquired on a 3T Philips Achieva (32-channel head coil) at Children’s Hospital Los Angeles. 3D T1-w: TR/TE=8.3/3.8 ms with isotropic voxel size of (VS) of 1 mm3. fMRI (700 s): TR/TE=1500/30 ms, VS=1.9×1.9×2.5 mm3, SENSE=5. End-tidal CO2 levels and CO2 stimuli were monitored/regulated via automated gas mixer (RespirAct, Thornhill Research, Toronto). A 4-cycle sinusoidal CO2 paradigm with peak-to-peak amplitude of five torr and period of one minute was utilized. The CO2 sinusoid was biased +5 torr from resting ETCO2, such that CO2 fluctuations ranged from 0-10 torr greater than resting ETCO2. CO2 data were temporally interpolated/resampled to match the BOLD acquisition scheme.
CVR modeling: T1-w cortical surface delineation, registration, and parcellation to the BCI-DNI anatomical atlas was performed using BrainSuite (http://brainsuite.org/). Preprocessing of BOLD images included slice-timing and distortion correction (FSL), followed by co-registration to T1-w and BCI-DNI atlas space. CVR was estimated using a coherence-weighted general linear model6, calculating least-squares linear fit between BOLD magnitude and CO2 signal in the frequency domain.
Statistical Analysis: We performed a global quantification of CVR as well as a voxel-wise analysis comparing FP and CTL groups, in the whole brain (excluding the ventricles).
Results
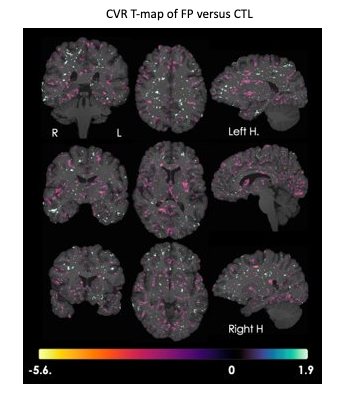
Comparison of global CVR between Fontan and control subjects did not achieve statistical significance in in gray/white matter (Figure 1), although qualitative inspection revealed a diminished CVR response in the Fontan cohort. Regional T-maps (Figure 2) showed significant local differences between these groups. Fontan patients had decreased CVR in peripheral cortical regions (purple regions), and higher CVR in deeper, predominantly white matter, structures (light blue).Discussion
Patients with Fontan palliation have a circulation that mimics right heart failure. The lack of a pulmonary pump limits flow through the lungs and reduces cardiac output, forcing the body to reduce brain vascular resistance (“brain sparing”) to preserve brain blood flow. Central venous pressures are typically increased, which can impede cerebral venous return. Our hypothesis included suspicion that long-term effects of Fontan physiology would contribute to observed differences in cerebral autoregulation, including globally depressed CVR7.Our data show that global CVR response is likely diminished in patients with Fontan physiology compared to healthy controls, although this difference does not achieve statistical significance. An examination of regional data (Fig. 2) provides potential explanation for these results, in which derangements/changes in autoregulation may occur on a highly specific local basis, with regions of decreased CVR (purple) located predominantly within the cortical grey matter, and scattered across all major arterial distributions. Unexpected regions of increased CVR (light blue) were observed in deep white matter, including arcuate fibers, superior orbitofrontal fasiculus, superior longitudinal fasiculus, and uncinate, with few areas of increased CVR in the cortex (limited example regions include orbitofrontal cortex and inferior temporal gyrus).
The changes observed in CVR may represent adaptive consequences of compensation, and may also represent derangements in autoregulation that result from prolonged exposure to Fontan physiology. Future work will include multimodal comparison including pairing with available neurocognitive testing, diffusion weighted imaging, resting state connectivity, arterial spin labeling, and morphometry data, in effect to explain the origin and functional significance of the observed phenomenon.
Conclusion
Global CVR impairment was observed (not reaching statistical significance) in patients with Fontan palliation, and significant changes (both positive and negative) were observed focally throughout the brain. Additional neurovascular and neurocognitive phenotyping is ongoing to provide additional context for these findings.Acknowledgements
This work was supported by Additional Ventures Single Ventricular Fund, the National Heart Lung and Blood Institute (1RO1HL136484-A1), and the National Center for Research Resources (UL1 TR001855-02) of the National Institutes of Health. Philips Healthcare provided support for protocol development and applications engineering on a support-in-kind basis.References
1. Feinstein J, Benson D, Dubin A, et al. Hypoplastic left heart syndrome: current considerations and expectations. J Am Coll Cardiol. 2012; 59.
2. Fruitman D. Hypoplastic left heart syndrome: Prognosis and management options. Paediatr Child Health. 2000; 5(4): 219-25.
3. Marelli A, Miller SP, Marino BS, et al. Brain in Congenital Heart Disease Across the Lifespan: The Cumulative Burden of Injury. Circulation. 2016; 133(20): 1951-62.
4. Verrall CE, Blue GM, Loughran-Fowlds A, et al. 'Big issues' in neurodevelopment for children and adults with congenital heart disease. Open Heart. 2019; 6(2).
5. Liu P, De Vis J, and Lu H. Cerebrovascular reactivity (CVR) MRI with CO2 challenge: A technical review. Neuroimage. 2019; 187: 104-115.
6. Xu B, Vu C, Borzage M, et al. Improved cerebrovascular reactivity mapping using coherence weighted general linear model in the frequency domain. Neuroimage. In press.
7. Binotto M, Maeda N, and Lopes A. Altered endothelial function following the Fontan procedure. Cardiology in the Young. 2008; 18(1), 70-74.
Figures