4417
Location matters: Altered interhemispheric homotopic connectivity in post-stroke dyskinesia1Department of Radiology, Zhongnan Hospital of Wuhan University, Wuhan, China, 2Department of Radiology, The First College of Clinical Medical Science of China Three Gorges University, Yichang, China, 3Philips Healthcare, Shanghai, China
Synopsis
Keywords: Functional Connectivity, Stroke, functional connectivity
Motivation: How stroke at different locations affects homotopic connectivity remains incompletely understood.
Goal(s): This study aimed to examine how motor deficits resulting from acute stroke in different brain regions impact homotopic connectivity.
Approach: Patients with dyskinesia were included and divided into 4 demographically matched subgroups by stroke location: frontoparietal, radiation coronal, basal ganglia, and brain stem. Additional 37 matched healthy controls were also recruited. Interhemispheric homotopic functional and structural connectivity was obtained by resting-state functional MRI and diffusion tensor imaging.
Results: Our results suggest that post-stroke motor deficits in different regions implicate different links from cortical to subcortical areas.
Impact: Alterations in lesion topography and regional functional homotopy provide new insights into the understanding of neural basis of motor disorders and also inform potential individualized precisive targets.
Introduction
Motor impairment is the most common consequence after a stroke1,2. Interhemispheric homotopic connectivity varies regionally and hierarchically along the somatomotor-association cortex axis and is particularly important for maintaining normal motor function3. However, our understanding of how stroke at different locations affects homotopic connectivity remains incomplete. This study aimed to examine how motor deficits resulting from acute stroke in different brain regions impact homotopic connectivity.Methods
84 acute ischemic stroke patients with dyskinesia were included and divided into 4 demographically matched subgroups by stroke location: frontoparietal (15), radiation coronal (16), basal ganglia (30), and brain stem (23). Additional 37 matched healthy controls were also recruited. Multimodal MRI data, and motor function assessments were collected. Interhemispheric homotopic functional and structural connectivity was obtained by resting-state functional MRI and diffusion tensor imaging, respectively, and correlated with motor function scores.Results
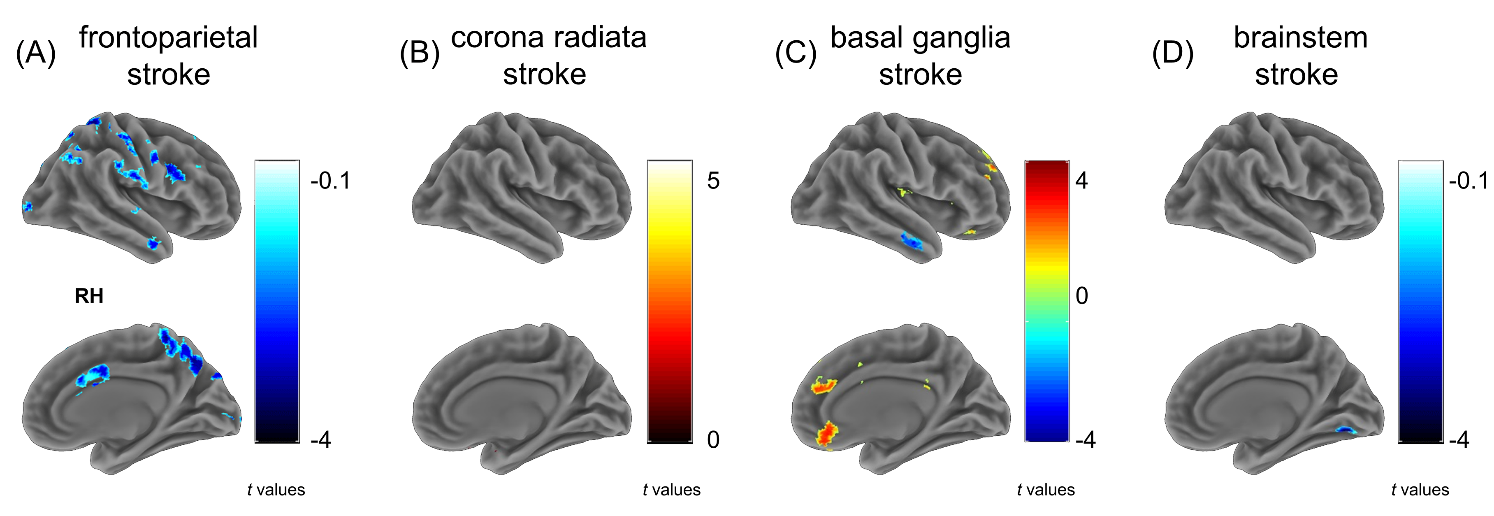
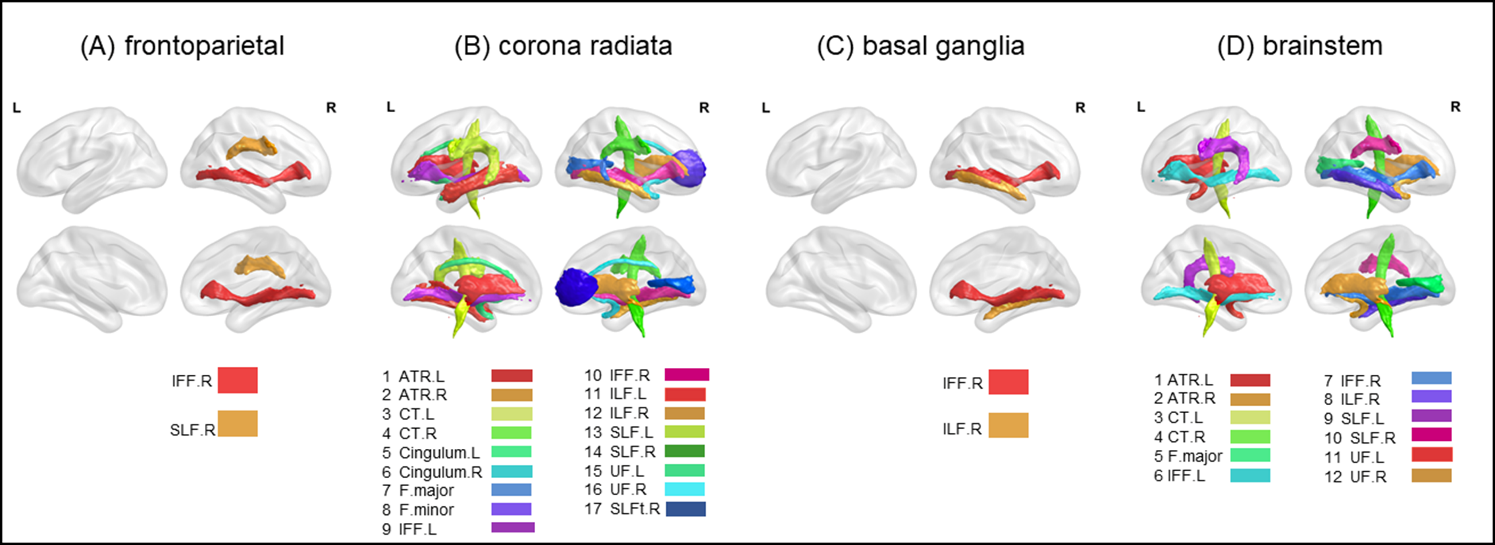
VMHC-based results showed that frontoparietal and basal ganglia strokes resulted in reduced homotopic connectivity in somatosensory/motor cortex, whereas radiation coronal and brainstem strokes were associated with altered interhemispheric connectivity in subcortical motor circuits (Fig. 1). Diffusion tensor imaging based structural connectivity suggested that frontal-parietal and basal ganglia strokes primarily affected cortical association fibers, whereas radiation coronal and brainstem strokes involved extensive cortical-cortical and cortical-subcortical disruption of the integrity of white matter fibers (Fig. 2).Discussion
In the present study, we examined changes in homotopic functional and structural connectivity in patients with acute cerebral infarction at different sites (frontal-parietal, radial-coronal, basal ganglia, and brainstem) to provide information about interhemispheric structural and functional involvement and the potential relationship between these changes. Our main findings are as follows: VMHC was reduced in the somatosensory-motor cortex in the frontal-parietal lesion group compared with healthy controls, suggesting that functional connectivity between sensory-motor networks is reduced in patients with acute cortical infarction. This change may be related to post-stroke motor dysfunction, which is in line with previous studies4-6. When compared to acute cortical infarction, patients with acute subcortical stroke showed significantly different VMHC changes. The results showed a decrease in VMHC in the visual cortex but a significant increase in VMHC in the frontoparietal network. The orbital prefrontal cortex mainly processes sensory experiences generated by convergent information related to emotions (e.g., disgust or uneasiness)7. This pattern of increase and decrease may reflect the reorganization of emotional control, memory, cognitive function, higher cognitive function, and visual function after acute cerebral infarction.Conclusion
Our results suggest that post-stroke motor deficits in different regions implicate different links from cortical to subcortical areas. Alterations in lesion topography and regional functional homotopy provide new insights into the understanding of neural basis of motor disorders and also inform potential individualized precisive targets.Acknowledgements
The authors would like to thank the patients and volunteers for participating in this study, and to the team of Dr. Yong Qin from the Department of Rehabilitation and Dr. Jinghua Zhou from the Department of Neurology for their help at all stages of the project.References
1. Feigin VL, Stark BA, Johnson CO, et al. Global, regional, and national burden of stroke and its risk factors, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. The Lancet Neurology 2021; 20:795-820.
2. Hankey GJ. Potential new risk factors for ischemic stroke: what is their potential? Stroke 2006; 37:2181-2188.
3. Feigin VL, Forouzanfar MH, Krishnamurthi R, et al. Global and regional burden of stroke during 1990–2010: findings from the Global Burden of Disease Study 2010. The lancet 2014; 383:245-255.
4. Zhang Y, Liu N, Wang Z, et al. Impaired inter-hemispheric functional connectivity during resting state in female patients with migraine. Brain Sciences 2022; 12:1505.
5. Van Meer MP, Van Der Marel K, Wang K, et al. Recovery of sensorimotor function after experimental stroke correlates with restoration of resting-state interhemispheric functional connectivity. J Neurosci 2010; 30:3964-3972.
6. Van Meer MP, Van der Marel K, Otte WM, Berkelbach Van Der Sprenkel JW, Dijkhuizen RM. Correspondence between altered functional and structural connectivity in the contralesional sensorimotor cortex after unilateral stroke in rats: a combined resting-state functional MRI and manganese-enhanced MRI study. Journal of Cerebral Blood Flow & Metabolism 2010; 30:1707-1711.
7. Burgdorf J, Panksepp J. The neurobiology of positive emotions. Neuroscience & Biobehavioral Reviews 2006; 30:173-187.
Figures