4413
Blood supply may affect the prognosis of meningiomas: a retrospective study based on Territorial Arterial Spin Labelling1Huashan Hospital, Fudan University, Shanghai, China, 2Radiology, Huashan Hospital North, Fudan University, Shanghai, China
Synopsis
Keywords: fMRI Analysis, Brain
Motivation: To explore the relationship between blood supply and prognosis of meningioma.
Goal(s): Whether meningioma mainly supplied by the internal and external carotid artery (ICA and ECA) have different prognosis and symptoms, and the relationship between prognosis with blood supply and other clinical characteristics (including age, gender, tumor volume etc.).
Approach: Territorial Arterial Spin Labelling was used to identify the feeding arteries of meningioma and divide patients into different blood supply groups.
Results: Meningioma supplied by ICA had worse prognosis than ECA. Dizziness and headache were the most common symptoms in ICA and ECA groups, respectively. Age and pathological grading had effect on prognosis.
Impact: Blood supply of meningioma was a prognosis-related factor, which was related to clinical symptoms and pathological results of patients, making it more crucial for neurosurgeons in planning surgery as well as evaluating prognosis.
INTRODUCTION
Over past years, many studies have discussed the prognostic factors of meningioma such as gender, age, tumor location and volume, etc 1, 2. However, the impact of feeding arteries of meningioma have not been identified clearly, which are essential to targeted treatment options and postoperative recovery. Territorial Arterial Spin Labelling (t-ASL) is a technology that can visualize cerebral perfusion in certain regions and depict the regions of each feeding artery by labelling arteries selectively without contrast agents and invasive procedures 3, 4. This research was to retrospectively investigate whether meningioma mainly supplied by the internal carotid artery (ICA) and those supplied by the external carotid artery (ECA) by t-ASL have different prognosis and clinical symptoms. The effect of clinical factors on the prognosis of meningiomas were also investigated.METHODS
A total of 33 pathologically-confirmed meningioma patients were included. T-ASL was used to identify the original feeding arteries of meningioma before surgery. The clinical factors including age, gender, tumor location, tumor volume, Simpson grade, pathological grading and Ki67 were also collected. The Glasgow Coma Score (GCS) measured the level of activity and requirements of patients after surgery for short-term prognosis and the Karnofsky Perfomance Score (KPS) was used to evaluate the status of prognosis before patients discharged for long-term prognosis. Statistical analysis was performed with statistical software (R software, version 3.5.0) and one-way ANOVA was used to compare the prognostic difference among the different blood supply groups.RESULTS
Patients were divided into ICA-Group (exclusive ICA supply, n = 7), ECA-Group (exclusive ECA, n = 10), Co-supplied Group 1 and Group 2 (mixed supply with ICA or not, n = 10 and 6), with a significant prognostic difference (p<0.001) by t-ASL. The ECA-Group had the best prognosis (GCS = 14.67 ± 0.52, KPS = 90.00 ± 6.67) while ICA-Group had the worst (GCS = 13.43 ± 0.98, KPS = 61.43 ± 15.74). Co-supplied Group 1 had lower scores than Group 2. In ICA-Group, dizziness was the most common symptom (5/7, 71.43%), while ECA-Group mostly presented headache (8/10, 80%). Besides blood supply, age and pathological grading had effect on prognosis (both p<0.001).DISCUSSION
The ICA group had the lowest GCS and KPS value while those of the ECA group were the highest. Combined with our results and previous work 5-7, we proposed that the prognosis of meningioma was strongly related to blood supply. Therefore, if a meningioma patient has been clear about the sources of the tumor blood supply before operation, the prognosis can be preliminarily determined. In terms of the clinical symptoms, we found patients bearing ICA-supplied meningioma were more likely to complain of "dizziness" in this study, while patients with ECA were more likely to have headache. We proposed that the dizziness in ICA-supplied meningioma patients was possibly a symptom of ischemic changes caused by the "blood-stealing" from basilar arteries (BAs) system (especially the anterior-inferior cerebellar artery, AICA, which supplies the inner ear) to ICA supplied region including the meningioma 8, 9. Another explanation of the dizziness in ICA-supplied meningioma was related to the suppression of certain brain regions 10. In the ECA group, the main complaint was “headache”, closely connected with the anatomical structures of the endocranium, thus it is likely that the tumors pull and compress these structures. Moreover, the tumor is prone to grow, infiltrate, and adhere with the local dura mater, so it has direct stimulation to the dura mater and then cause headache 11. Based on these findings, we proposed that the blood supply of meningioma could be estimated based on the initial symptoms. We also analyzed the gender, age, tumor location, volume, surgical resection grade, Ki67 and pathological grade of these cases, which are often discussed as possible prognosis-related factors. Older age and higher pathological grade was found to be associated with worse results, while gender, tumor location and volume of meningioma patient had no correlation with prognosis, which was consistent with previous studies 1, 12-14.CONCLUSION
Blood supply is considered as an important prognosis-related factor. ICA-supplied meningioma demonstrate a worse prognosis than ECA-supplied ones, and clinical symptoms are also associated with blood supply. Also, age and pathological grade had an effect on outcome. Further studies should put more attention to the artery supply of meningioma, making it more crucial for neurosurgeons in planning surgery as well as evaluating prognosis.Acknowledgements
The authors would like to acknowledge the financial support from the Science and Technology Innovation Action Plan of Shanghai Science and Technology Commission No.22S31905900 (B.Y.) and the Youth Program of National Natural Science Foundation of China No.81901697 (Y.L.).References
1. Splavski B, Hadzic E, Bagic I, et al. Simple Tumor Localization Scale for Estimating Management Outcome of Intracranial Meningioma. World Neurosurg. 2017;104:876-882.
2. Islim AI, Mohan M, Moon RDC et al. Incidental intracranial meningiomas: a systematic review and meta-analysis of prognostic factors and outcomes. J Neurooncol. 2019;142(2):211-221.
3. van Laar PJ, van der Grond J, Hendrikse J. Brain perfusion territory imaging: methods and clinical applications of selective arterial spin-labeling MR imaging. Radiol. 2008;246(2):354-364.
4. Wong EC. Vessel-encoded arterial spin-labeling using pseudocontinuous tagging. Magn Reson Med. 2007;58(6):1086-1091.
5. Pistolesi S, Fontanini G, Camacci T et al. Meningioma-associated brain oedema: the role of angiogenic factors and pial blood supply. J Neurooncol. 2002;60(2):159-164.
6. Friconnet G, Espindola Ala VH, Janot K et al. MRI predictive score of pial vascularization of supratentorial intracranial meningioma. Eur Radiol. 2019;29(7):3516-3522.
7. Lu Y, Luan S, Liu L et al. Evaluation of the applicability of territorial arterial spin labeling in meningiomas for presurgical assessments compared with 3-dimensional time-of-flight magnetic resonance angiography. Eur Radiol. 2017;27(10):4072-4081.
8. Karatas M. Central vertigo and dizziness: epidemiology, differential diagnosis, and common causes. Neurologist. 2008;14(6):355-364.
9. Tan F, Bartels C, Walsh RM. Our experience with 500 patients with benign paroxysmal positional vertigo: Reexploring aetiology and reevaluating MRI investigation. Auris Nasus Larynx. 2018;45(2):248-253.
10. Dunniway HM, Welling DB. Intracranial tumors mimicking benign paroxysmal positional vertigo. Otolaryngol Head Neck Surg. 1998;118(4):429-436.
11. Taylor LP. Mechanism of brain tumor headache. Headache. 2014;54(4):772-775.
12. Domingues PH, Sousa P, Otero A et al. Proposal for a new risk stratification classification for meningioma based on patient age, WHO tumor grade, size, localization, and karyotype. Neuro Oncol. 2014;16(5):735-747.
13. Kallio M, Sankila R, Hakulinen T, et al. Factors affecting operative and excess long-term mortality in 935 patients with intracranial meningioma. Neurosurg. 1992;31(1): 2-12.
14. Pechlivanis I, Wawrzyniak S, Engelhardt M, et al. Evidence level in the treatment of meningioma with focus on the comparison between surgery versus radiotherapy. A review. J Neurosurg Sci. 2011;55(4):319-328.
Figures
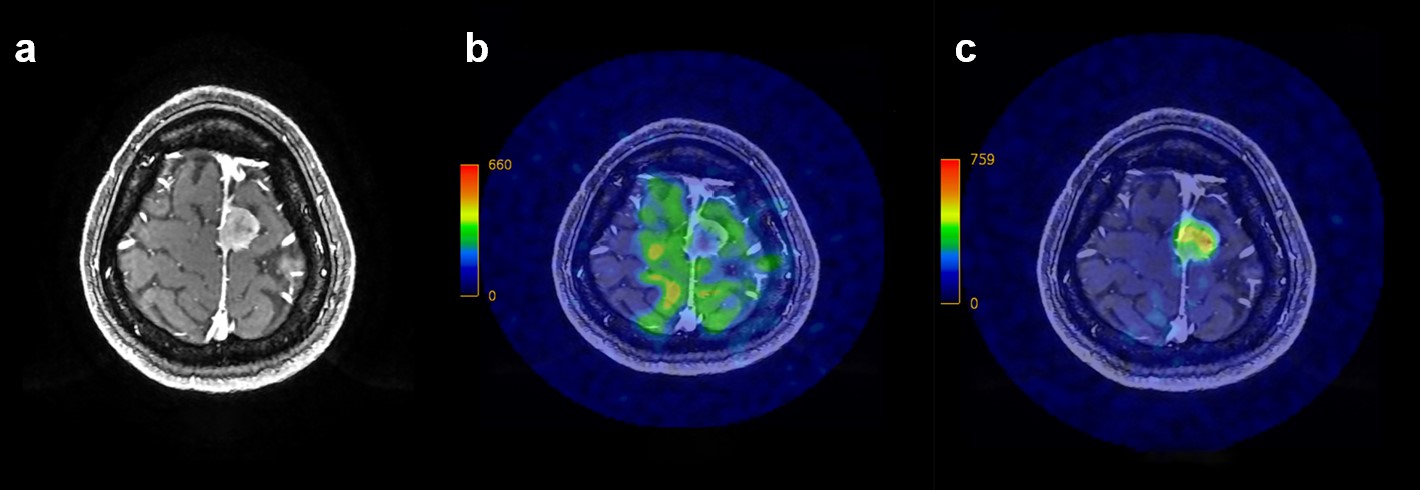
A 32-year-old woman was headache for 1 month. a. Axial contrast-enhanced T1WI imaging (CET1) showed an enhanced mass closed to the superior sagittal sinus. b. Axial territorial arterial spin labelling (t-ASL) of the left internal carotid artery (ICA) did not exhibit any perfusion in the tumor region. c. on the left external carotid artery (ECA) show hyper-perfusion in the whole region of the meningioma.
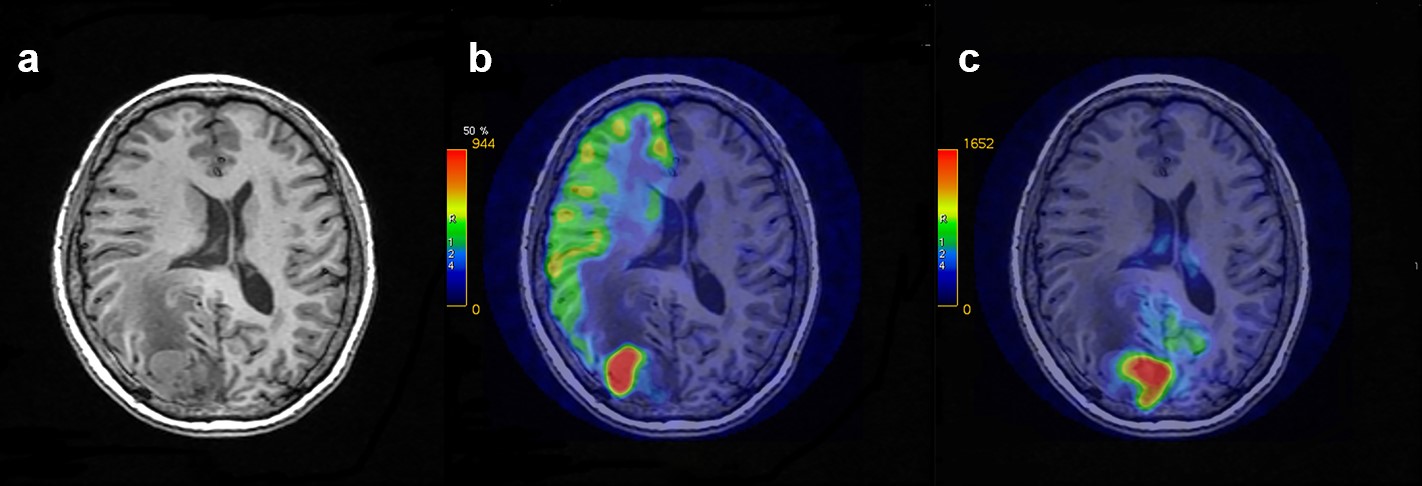
It showed a. CET1 imaging of a 64 year-old patient with meningioma in her right occipital region. Two representative slices of the associated perfusion territories showed the tumor was supplied by both right ICA (b. left-ICA images on tASL) and basilar artery (c. left-ECA images on t-ASL).
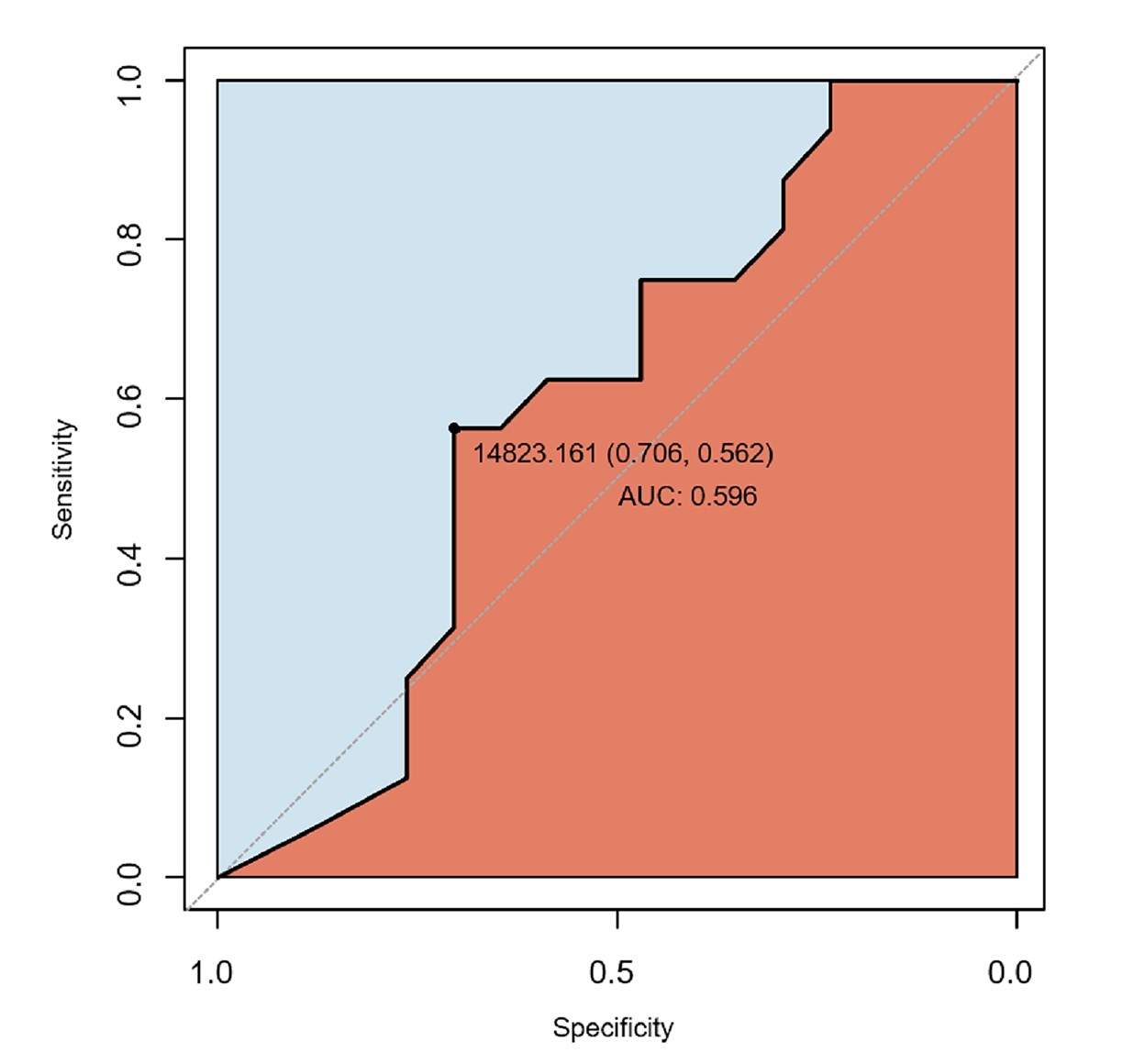
Receiver operating characteristic (ROC) analysis of meningioma volume of 33 patients. The area under the ROC curve (AUC) value from the ROC curve was 0.596. The sensitivity and specificity were highest relatively when the cutoff value was 14.82 cm3.
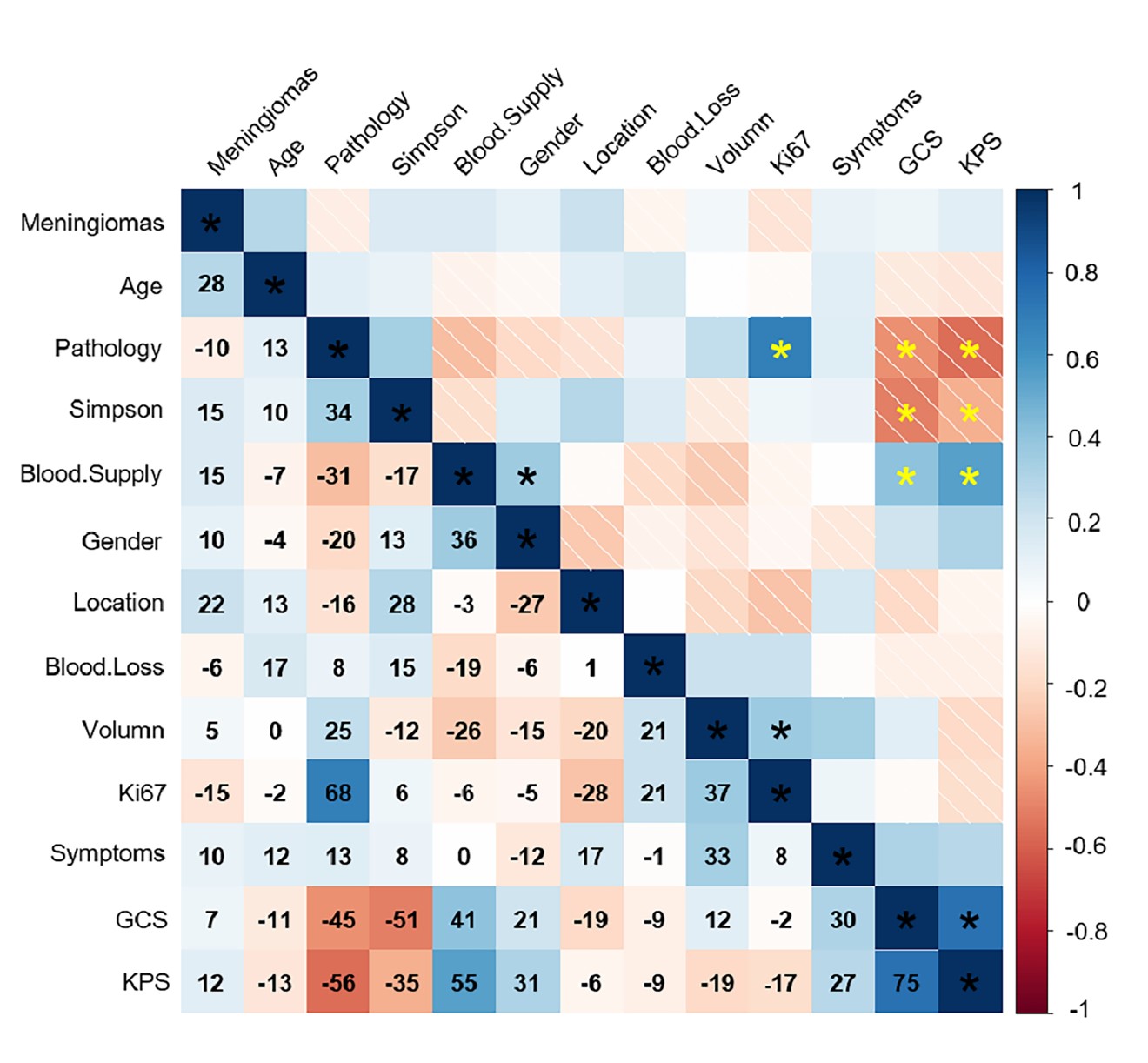
Matrix plot of correlations between morphological and clinical parameters. Correlation coefficients (CCs) range from -1 to 1. For clearly display, the numbers in the figure are CCs*100, and P < 0.05. All the clinical information with Glasgow Coma Score (GCS) and Karnofsky Perfomance Score (KPS) are shown in the matrix plot, and the highlight star was placed to show the stronger correlations between each other.