4400
Radiomic analysis of quantitative T2-mapping and conventional MRI in predicting histologic grade of bladder cancer1West China Hospital, Sichuan University, Chengdu, China, ChengDu, China, 2Department of Clinical, Philips Healthcare, China, Chengdu, China, 3West China Hospital, Sichuan University, Chengdu, China, Chengdu, China
Synopsis
Keywords: fMRI Analysis, Bladder, pathological grade
Motivation: MpMRI has been extensively used for the local staging of bladder cancer (BCa), it is worth using mpMRI for the preoperative evaluation of the pathological grade.
Goal(s): We explored the added value of a radiomics based on quantitativeT2-mapping and conventional MRI to evaluate the histologic grade of BCa pre-operatively.
Approach: Pelvic MRI including T2-mapping and diffusion-weighted imaging before any treatment were analyzed. We constructed different prediction models using mean signal values and radiomic features from both T2-mapping and apparent diffusion coefficient (ADC) maps.
Results: Radiomics could provide more information than direct evaluation of T2 and ADC values in differentiating histological grades of BCa.
Impact: Our observation of significantly improved performance using the radiomics model suggests that it incorporates tumor appearance, margin, and texture features, making it more representative of tumor characteristics. The incorporation of this model provides valuable additional information for BCa management.
Introduction
Transurethral resection of the bladder tumor (TURBT) is the recommended approach for confirming the grade (high or low) and the depth of muscular invasion (that is, T stage), which are both the determinants of the prognosis and treatment strategies. [1,2] Given BCa is a frequently recurrent disease, it would be of great benefit for patients using a non-invasive method to predict the pathological grade and T stage, and thus prevent patients from repetitive operations. Multiparametric magnetic resonance imaging (mpMRI) has been widely utilized for the BC local staging and could accurately predict about 85% of MIBC. [3]However, to accurately and invasively evaluate the pathological grade of the BCa remains as a challenge. T2-weighted parametric mapping is increasingly applied in the other organs, such as the brain, liver, and kidney. [4–6]In the context of these research, it was widely reported that tumors with higher cellularity demonstrated a corresponding lower signal in T2-maping as a result of reduction in the extracellular fluid space. While low-grade bladder cancers (BCa) are characterized with relatively ordered tumor cells and slightly larger nuclei, and thus a stable nuclear-to-cytoplasmic ratio, high-grade bladder cancers are associated with marked variations on both nuclear size and nuclear-to-cytoplasmic ratio, whereby it can be assumed that there are obvious differences on the extracellular fluid between cancers with different grade.[7] considering previous reports that low-grade BCa presented as obviously high signal intensity in T2WI, we assumed the quantitative T2 values of BCa may be helpful for distinguishing histologic grade. Besides, considering the distinctively cytologic features of different grade cancers, radiomics features extracted from medical images were regarded to be of more discrimination capacity than the investigator's eye. Therefore, this study aimed to investigate the potential of quantitative T2 mapping MRI in evaluating the histologic grade of BCa, and to evaluate whether radiomics features based on T2-mapping can add diagnostic value to conventional MRI of bladder.Methods
Patients were eligible when suspected of BCa by ultrasound, and underwent pelvic MRI including T2-mapping and diffusion weighted imaging (DWI) before any treatment. Imaging was performed with a 3.0T system (Elition, Philips) with a 32-channel phased array surface coil. All study participants were acquired to urinate 2 hours before the MRI examination. All patients underwent surgery after scanning, and histological-proved urothelial BCa would be finally included. Mean signal values and 104 radiomic features were extracted from both T2-mapping and apparent diffusion coefficient (ADC) map. The diagnostic performance of each model or parameter was assessed by receiver operating characteristic curves (ROC).Results
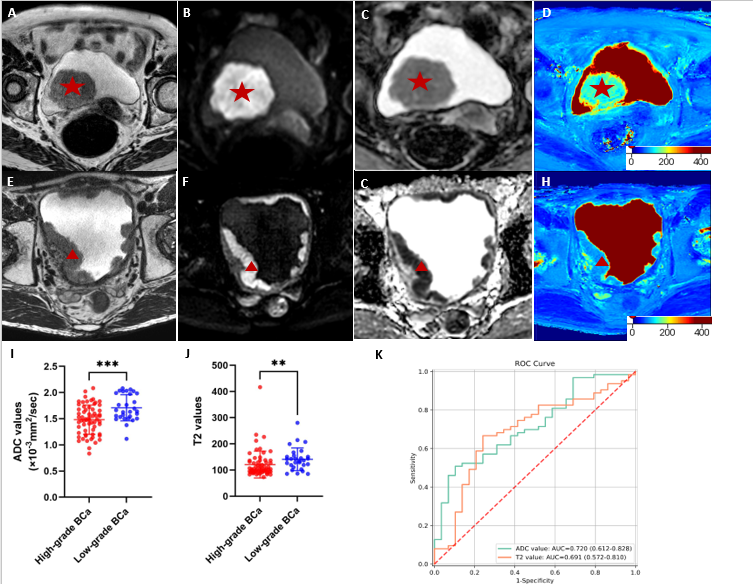
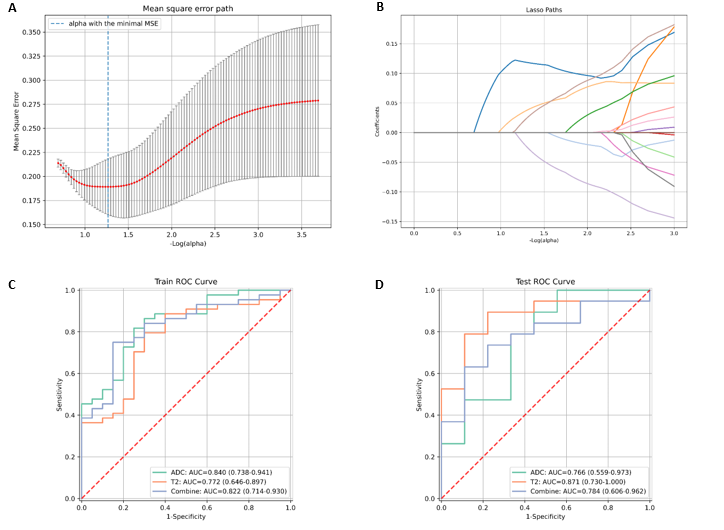
A total of 104 patients were included in this study (training cohort, n=64; testing cohort, n=40), of which 71 were high-grade BCa. Compared with patients with high-grade BCa as showed in Figure 1, patients with low-grade BCa had significantly higher T2 values (p=0.003), and higher ADC values (p<0.001). When using T2 values and ADC values to predict the pathological grade, the AUC values were 0.69 and 0.71 separately, which was moderate. We further used the most significant features from T2-mapping and ADC map to construct radiomics-based models. In the testing cohort, the T2-mapping model achieved the highest prediction performance with AUC values of 0.87 (95%CI 0.73-1.0), compared with the ADC model of 0.77 (95%CI 0.56-0.97), and the joint model of 0.78 (95%CI 0.61-0.96), as showed in Figure 2.Discussion
Our results showed that T2 values demonstrated moderate performance in differentiating histologic grade of BCa, while the radiomics model based on T2-mapping had significantly higher diagnostic performance. The plausible reason could be that radiomic model was an incorporation of tumor appearance, margin, and texture features, and therefore was more representative of tumor feature. Besides, our results showed that T2-mapping model performed better than both ADC and joint model. Our results could be explained by the fact that conventional T2WI only allows for a qualitative image interpretation based on the signal intensity with arbitrary unit, and therefore is more applicable in detecting lesions and differentiating lesions form peritumoral tissue. While T2 mapping technique is based on voxel-wise evaluation of proton spin-spin relaxation times, and therefore allows for a standard and reproducible visualization and quantification of tissue composition and, in particular, interstitial edema and extracellular space expansion.Conclusions
Our results demonstrated that radiomics could provide more information than direct evaluation of T2 and ADC value in differentiating histologic grade. Besides, T2-mapping-based radiomics model outperformed ADC-based and joint models for predicting the pathological grade of BCa preoperatively and non-invasively.Acknowledgements
noneReferences
1. Flaig, T.W.; Spiess, P.E.; Agarwal, N.; Bangs, R.; Boorjian, S.A.; Buyyounouski, M.K.; Chang, S.; Downs, T.M.; Efstathiou, J.A.; Friedlander, T.; et al. Bladder Cancer, Version 3.2020, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw 2020, 18, 329–354, doi:10.6004/jnccn.2020.0011.
2. Taylor, J.; Becher, E.; Steinberg, G.D. Update on the Guideline of Guidelines: Non-Muscle-Invasive Bladder Cancer. BJU Int 2020, 125, 197–205, doi:10.1111/bju.14915.
3. Ye, L.; Chen, Y.; Xu, H.; Xie, H.; Yao, J.; Liu, J.; Song, B. Biparametric Magnetic Resonance Imaging Assessment for Detection of Muscle-Invasive Bladder Cancer: A Systematic Review and Meta-Analysis. Eur Radiol 2022, 32, 6480–6492, doi:10.1007/s00330-022-08696-5.
4. Luetkens, J.A.; Klein, S.; Träber, F.; Schmeel, F.C.; Sprinkart, A.M.; Kuetting, D.L.R.; Block, W.; Uschner, F.E.; Schierwagen, R.; Hittatiya, K.; et al. Quantification of Liver Fibrosis at T1 and T2 Mapping with Extracellular Volume Fraction MRI: Preclinical Results. Radiology 2018, 288, 748–754, doi:10.1148/radiol.2018180051.
5. Wolf, M.; de Boer, A.; Sharma, K.; Boor, P.; Leiner, T.; Sunder-Plassmann, G.; Moser, E.; Caroli, A.; Jerome, N.P. Magnetic Resonance Imaging T1- and T2-Mapping to Assess Renal Structure and Function: A Systematic Review and Statement Paper. Nephrol Dial Transplant 2018, 33, ii41–ii50, doi:10.1093/ndt/gfy198.
6. Wang, Y.; Liu, X.; Wang, J.; Wang, Y.; Qi, H.; Kong, X.; Liu, D.; Liu, J.; Zheng, H.; Xiong, F.; et al. Simultaneous T1, T2, and T2* Mapping of Carotid Plaque: The SIMPLE* Technique. Radiology 2023, 307, e222061, doi:10.1148/radiol.222061.
7. Compérat, E.M.; Burger, M.; Gontero, P.; Mostafid, A.H.; Palou, J.; Rouprêt, M.; van Rhijn, B.W.G.; Shariat, S.F.; Sylvester, R.J.; Zigeuner, R.; et al. Grading of Urothelial Carcinoma and The New “World Health Organisation Classification of Tumours of the Urinary System and Male Genital Organs 2016.” Eur Urol Focus 2019, 5, 457–466, doi:10.1016/j.euf.2018.01.003.
Figures