4395
Altered functional brain networks in coronary heart disease: Independent component analysis and graph theoretical analysis1Radiology, Xiamen Cardiovascular Hospital of Xiamen University, Xiamen, China, 2GE Healthcare, Beijing, China
Synopsis
Keywords: Functional Connectivity, Brain Connectivity
Motivation: Coronary heart disease (CHD) confers a high risk of cognitive and mental impairments in patients.
Goal(s): To explore the association of CHD with functional connectivity and topological properties of brain networks.
Approach: We collected rs-fMRI data to assess brain functional connectivity and topological properties in CHD patients.
Results: Compared to HCs, CHD patients exhibited increased functional connectivity between the default mode network and visual network, as well as decreased functional connectivity between the left frontoparietal network and auditory network. Small-world network topology was identified in both CHD patients and HCs. Furthermore, the nodal local efficiency of left putamen was decreased in CHD patients.
Impact: Abnormal brain functional connectivity and topological properties in CHD patients might extend current understanding of CHD-related brain dysfunction from the perspective of functional network organization, which expanded the knowledge of the brain function changes and potential neurological mechanism of CHD.
Introduction
Coronary heart disease (CHD) is one of the leading causes of death worldwide, resulting in approximately 7.4 million deaths per year 1. Studies have demonstrated that risk factors associated with CHD, such as hypertension, diabetes, overweight and smoking, also contributed to cognitive dysfunction 2,3. Rosebud et al. revealed that CHD patients exhibited poorer performance in neuropsychological tests 4. Additionally, Eggermont et al. highlighted that CHD could lead to the development of cerebral small vessel disease, which potentially affects brain function 5. These findings indicate a hypothetical yet unexplored connection between CHD and higher-order cognitive processing. Resting-state functional MRI (rs-fMRI) has been widely applied in research on neuropsychiatric disorders 6,7. Employing a network-based statistics approach, Bernard et al. observed a significant increase in connectivity strength in the middle orbitofrontal regions in patients with acute coronary syndrome, which was related to executive dysfunction 8. CHD impacts functional network connectivity and further affects brain function, aspects that motivate further exploration. Analyses of rs-fMRI data, such as independent component analysis (ICA) and graph theoretical analysis (GTA) can characterize abnormal brain networks associated with various brain disorders 9. ICA allows examination of whole-brain connectivity without predefined seed regions, making it highly valuable in brain researches 6. Several chronic inflammatory conditions have revealed alterations in internetwork FC related to cognitive function 10-12. In contrast, GTA considers the entire brain to be a complex network composed of nodes and edges 9. In GTA, a 'small world' topology has been observed in complex human brain networks, supporting efficient communication at a low cost 13,14. Topological abnormalities in the network might lead to various neuropsychiatric disorders 15-17. ICA and GTA methods are involved here for the first to investigate the characteristics of FC and topological features of brain networks in CHD patients. In this study, we hypothesized that 1) there would be discernible differences in FC between the brain networks of CHD patients and healthy controls (HCs), and 2) CHD would disrupt the topological features of intrinsic brain networks.Methods
The Ethics Committee of Xiamen Cardiovascular Hospital of Xiamen University approved the study. A total of 27 CHD patients and 44 volunteers matched in age, sex, and level of education were included in this study. All MRI data were obtained on a 3.0T MRI scanner (SIGNA Pioneer, GE Healthcare, Milwaukee, USA). fMRI data were preprocessed using SPM12 and DPABI. ICA was performed to parcellate the preprocessed data with the GIFT toolbox. Thirty-six independent components were identified automatically, and then time courses and spatial maps of independent components for each individual subject were acquired. Finally, 12 functional networks were identified from the 36 independent components (Figure 1): anterior and posterior default mode networks (aDMN and pDMN); left and right frontoparietal networks (lFPN and rFPN); dorsal and ventral sensorimotor networks (dSMN and vSMN); dorsal attention network (DAN); ventral attention network (VAN); salience network (SN); auditory network (AN); medial and posterior visual networks (mVN and pVN). The whole-brain functional network was constructed using the GRETNA toolbox. We selected a specific sparsity threshold ranging from 0.05 to 0.17 with an interval of 0.01 and calculated global and regional network measures at each sparsity threshold. The area under the curve (AUC) was calculated for each network metric to provide a summarized scalar. For internetwork FC and GTA analysis, a two-sample t test was applied to detect differences between the CHD and HC groups with age as a nuisance covariate. A significance threshold of P < 0.05 was utilized. For the regional metrics, the cluster-level False Discovery Rate (FDR) method was applied for multiple comparisons.Results
Twenty-seven CHD patients and 44 HC were included in the analysis. Details are summarized in Table 1. Compared to HCs, CHD patients exhibited increased FC between pDMN and mVN and decreased FC between lFPN and AN and between DAN and pVN (Figure 2A, 2B). In this study, both CHD and HC groups exhibited small-world topological networks (γ ≈ 1 and σ > 1.1) (Figure 3A, 3B). The AUC of nodal local efficiency of the left putamen was lower in the CHD group (Figure 4).Discussion and Conclusion
The present study demonstrated that patients with CHD showed altered functional brain networks, especially involved in higher-order cognition. Abnormal FC and topological properties in the brains of CHD patients under rest statement might extend the current understanding of CHD-related brain dysfunction from the perspective of functional network organization, which expanded the knowledge of the brain function changes and potential neurological mechanism of CHD.Acknowledgements
We thank all participants in this study, and this work was supported by grants from the Natural Science Foundation of Fujian Province, China (Grant No. J01535).References
1. Deckers K, Schievink SHJ, Rodriquez MMF, et al. Coronary heart disease and risk for cognitive impairment or dementia: Systematic review and meta-analysis. Plos One. 2017;12(9).
2. Grodstein F. Cardiovascular risk factors and cognitive function. Alzheimers & Dementia. 2007;3(2):S16-S22.
3. Arntzen KA, Schirmer H, Wilsgaard T, Mathiesen EB. Impact of cardiovascular risk factors on cognitive function: The Troms circle divide study. European Journal of Neurology. 2011;18(5):737-743.
4. Roberts RO, Knopman DS, Geda YE, Cha RH, Roger VL, Petersen RC. Coronary heart disease is associated with non-amnestic mild cognitive impairment. Neurobiology of Aging. 2010;31(11):1894-1902.
5. Eggermont LHP, de Boer K, Muller M, Jaschke AC, Kamp O, Scherder EJA. Cardiac disease and cognitive impairment: a systematic review. Heart. 2012;98(18):1334-1340.
6. Wang CL, Cai HH, Sun XT, et al. Large-Scale Internetwork Functional Connectivity Mediates the Relationship between Serum Triglyceride and Working Memory in Young Adulthood. Neural Plasticity. 2020;2020.
7. Lin SM, Nie MM, Wang BS, et al. Intrinsic brain abnormalities in chronic rhinosinusitis associated with mood and cognitive function. Frontiers in Neuroscience. 2023;17.
8. Bernard C, Catheline G, Dilharreguy B, et al. Cerebral changes and cognitive impairment after an ischemic heart disease: a multimodal MRI study. Brain Imaging and Behavior. 2016;10(3):893-900.
9. Xiao FL, Spruyt K, Lu C, Zhao DJ, Zhang J, Han F. Resting-state brain network topological properties and the correlation with neuropsychological assessment in adolescent narcolepsy. Sleep. 2020;43(8).
10. Jafari A, Xavier LD, Bernstein JD, Simonyan K, Bleier BS. Association of Sinonasal Inflammation With Functional Brain Connectivity. Jama Otolaryngology-Head & Neck Surgery. 2021;147(6):534-543. 11. Hou JC, Mohanty R, Nair VA, et al. Alterations in resting-state functional connectivity in patients with Crohn's disease in remission. Scientific Reports. 2019;9.
12. Kornelsen J, Wilson A, Labus JS, Witges K, Mayer EA, Bernstein CN. Brain Resting-State Network Alterations Associated With Crohn's Disease. Frontiers in Neurology. 2020;11.
13. Zhu JJ, Zhuo CJ, Liu F, Qin W, Xu LX, Yu CS. Distinct disruptions of resting-state functional brain networks in familial and sporadic schizophrenia. Scientific Reports. 2016;6.
14. Bassett DS, Bullmore ET. Small-world brain networks. Neuroscientist. 2006;12(6):512-523.
15. Zhu JJ, Qian YF, Zhang B, et al. Abnormal synchronization of functional and structural networks in schizophrenia. Brain Imaging and Behavior. 2020;14(6):2232-2241.
16. Stam CJ, de Haan W, Daffertshofer A, et al. Graph theoretical analysis of magnetoencephalographic functional connectivity in Alzheimers disease. Brain. 2009;132:213-224.
17. Zhang JR, Wang JH, Wu QZ, et al. Disrupted Brain Connectivity Networks in Drug-Naive, First-Episode Major Depressive Disorder. Biological Psychiatry. 2011;70(4):334-342.
Figures
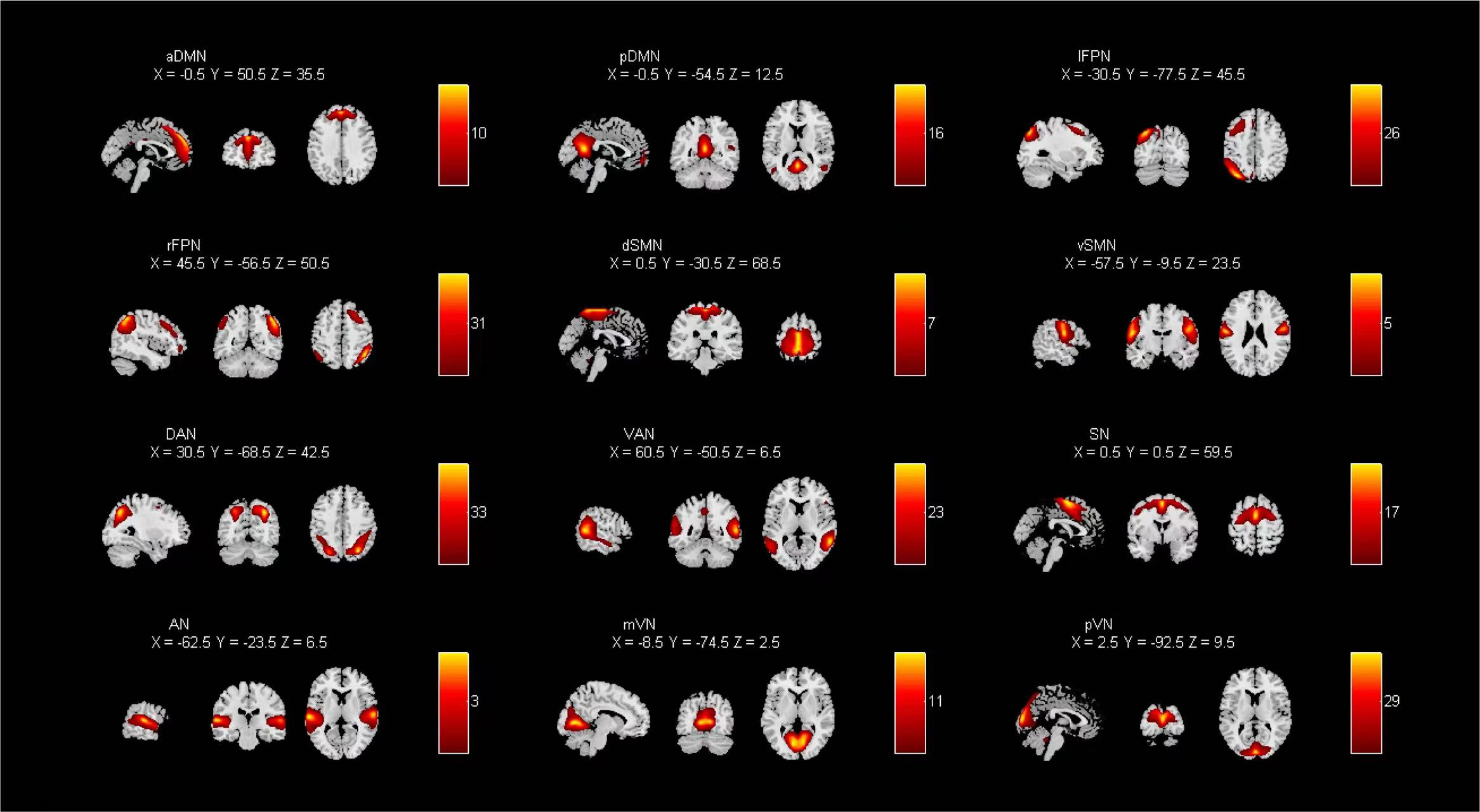
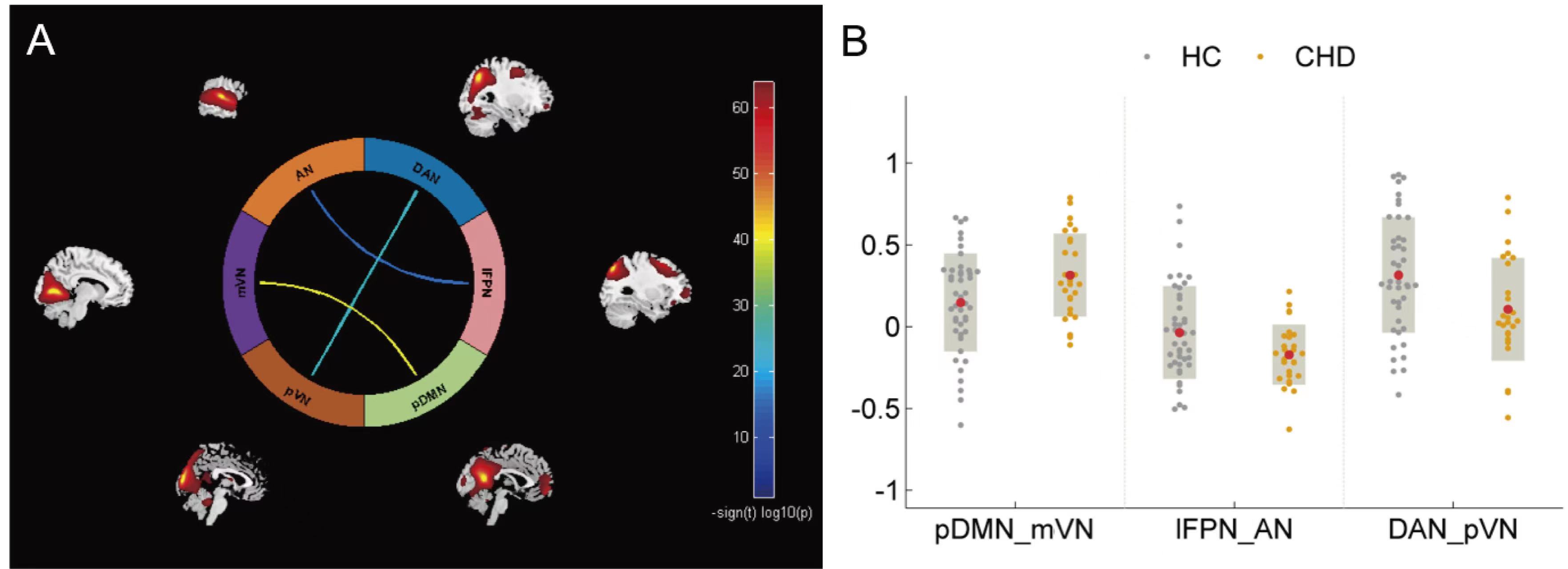
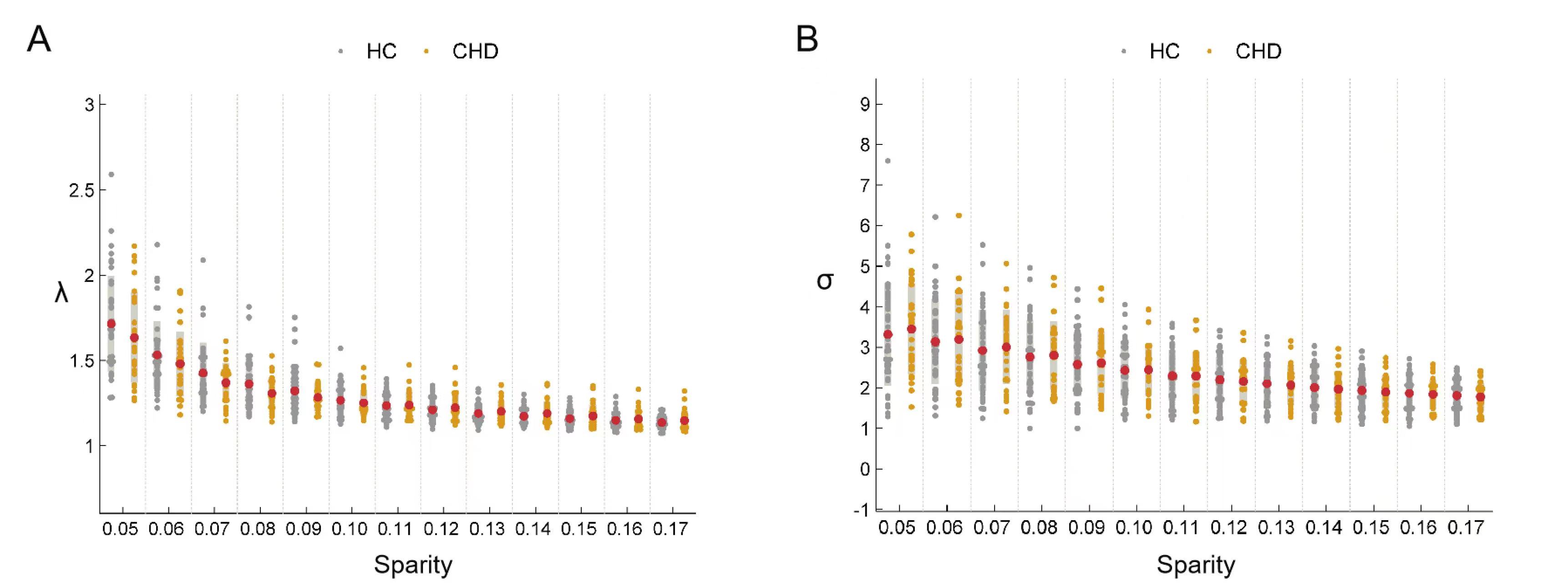
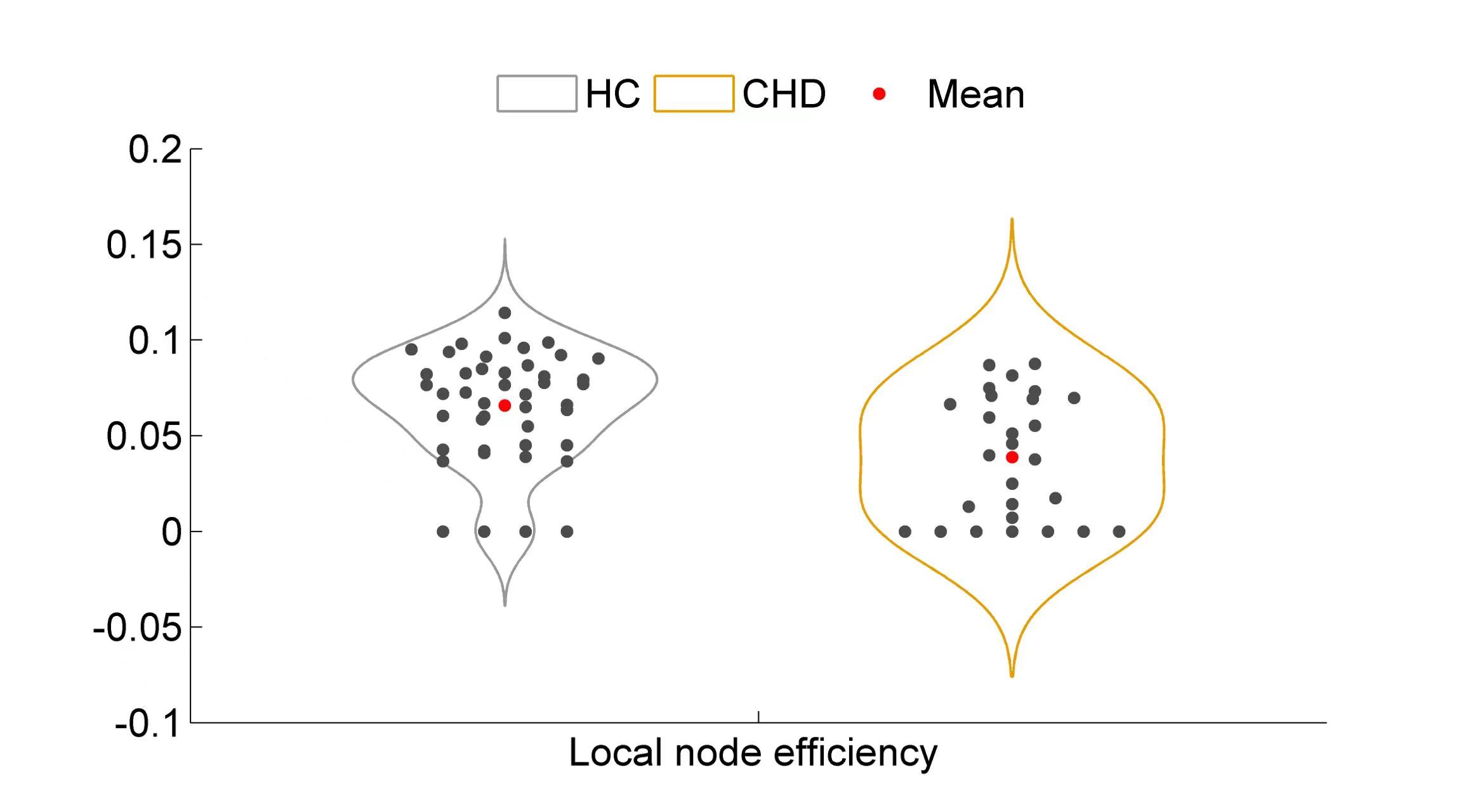
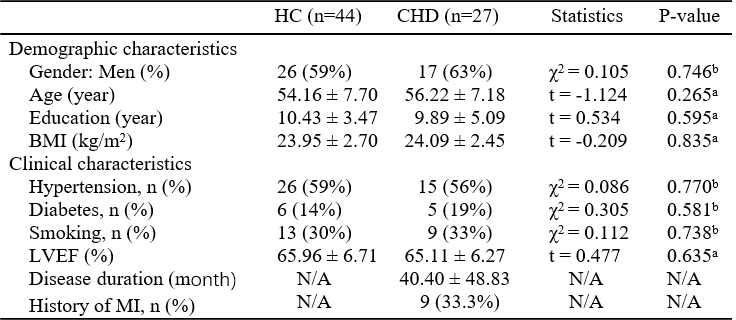
Table 1 Demographic and clinical characteristics. The data are shown as the mean values ± standard deviations. aThe P-value was obtained by the two-sample t-test. bThe P-value was obtained by the Chi-square test. N/A = not applicable; BMI = body mass index; LVEF = left ventricular ejection fraction; MI = myocardial infarction.