4388
Dorsal nigral hyperintensity abnormality in 7T MRI is a biomarker for diagnosis of Parkinson’s disease and atypical parkinsonisms1Department of Neurology, Beijing Tiantan Hospital, Capital Medical University, Beijing, China, 2Tiantan Neuroimaging Center of Excellence, Beijing Tiantan Hospital, Capital Medical University, Beijing, China, 3Hinda and Arthur Marcus Institute for Aging Research, Hebrew SeniorLife, Roslindale, MA, United States, 4Pacific Parkinson’s Research Centre, Djavad Mowafaghian Centre for Brain Health, University of British Columbia, Vancouver, BC, Canada, 5MR Research Collaboration Team, Siemens Healthineers, Beijing, China
Synopsis
Keywords: Parkinson's Disease, Parkinson's Disease, 7T MRI; dorsal nigral hyperintensity
Motivation: The dorsal nigral hyperintensity (DNH) abnormality is a characteristic feature of PD and 7T MRI has proved useful for its visualization.
Goal(s): To investigate the diagnostic efficiency of DNH abnormality at different stages of PD and in atypical parkinsonisms using 7T MRI.
Approach: PD, RBD, MSA-P, MSA-C, and PSP patients and controls underwent 7T T2* with DNH abnormality assessed for diagnostic performance. R2* mapping and principal component analysis were performed in substantia nigra.
Results: MSA-C and RBD demonstrated higher preservation rate of DNH than PD, MSA-P, and PSP. DNH scoring criteria proved an optimal diagnostic method of PD, RBD, MSA-P, MSA-C, and PSP.
Impact: MSA-C and RBD patients had higher dorsal nigral hyperintensity (DNH) preservation rate compared with PD, MSA-P, and PSP. The DNH scoring criteria proved an optimal diagnostic method of PD, RBD, MSA-P, MSA-C, and PSP.
Introduction
The dorsal nigral hyperintensity (DNH) abnormality is a characteristic feature of Parkinson’s disease (PD) and 7 Tesla (7T) MRI has proved a feasible tool for its high-resolution imaging. The purpose of this study was to investigate: (1) the diagnostic efficiency of the DNH abnormality at different stages of PD; (2) the utility of the DNH abnormality in differentiating PD from APs; (3) the candidate criteria of assessing the DNH abnormality that could improve clinical diagnosis; and (4) the pattern of metal deposition of the substantia nigra in PD and APs.Methods
A total of 155 PD, 12 rapid eye movement (REM) sleep behavior disorder (RBD), 40 multiple system atrophy (MSA)-parkinsonian type (MSA-P), 40 MSA-cerebellar type (MSA-C) and 25 progressive supranuclear palsy (PSP) patients as well as 83 healthy controls (HC) were included in the final analysis. MRI scans were performed on a 7T MRI scanner (MAGNETOM Terra, Siemens Healthineers, Germany). High resolution T2* MRI was obtained using a 3D fast-field echo sequence with TE = 8 ms/15 ms/22 ms/29 ms, TR = 42 ms, nominal flip angle α = 16°, spatial resolution 0.4 × 0.4 × 0.5 mm3, 88 axial slices, 8 minutes 24 seconds. The DNH abnormality was assessed based on the following criteria in previous studies: 1) bilaterally detected: the DNH being visible on both sides of the substantia nigra SN was defined as “normal”, and while its absence on any side of the substantia nigra SN was considered as “pathological”; 2) bilaterally normal: normally bright and present of the DNH on both sides of the substantia nigra SN was considered as “normal”, and its abnormality on any side of the SN was considered as “pathological”; 3) Evaluation by a 6-point visibility scale 16: 0 = darker than surrounding substantia nigraSN, 1 = not identifiable as is similar with surrounding low signal, 2 = parts of the outline possibly visible but not definitely identifiable, 3 = very difficult to detect but identifiable, 4 = reduced size or slightly more difficult to see than normal but definitely identifiable, 5 = normally bright and present; 4) Evaluation by the area of hyperintensity using a 2-point scale: 2 = normal, 1 = possibly abnormal (hypointensity in < 50% of the presumed DNH region), 0 = definitely abnormal (hypointensity in ≥ 50% of the presumed DNH region). The DNH abnormality was evaluated for their diagnostic and differential diagnostic performance to purpose the optimal assessment criteria. R2* mapping and principal component analysis were performed in the substantia nigra.Results
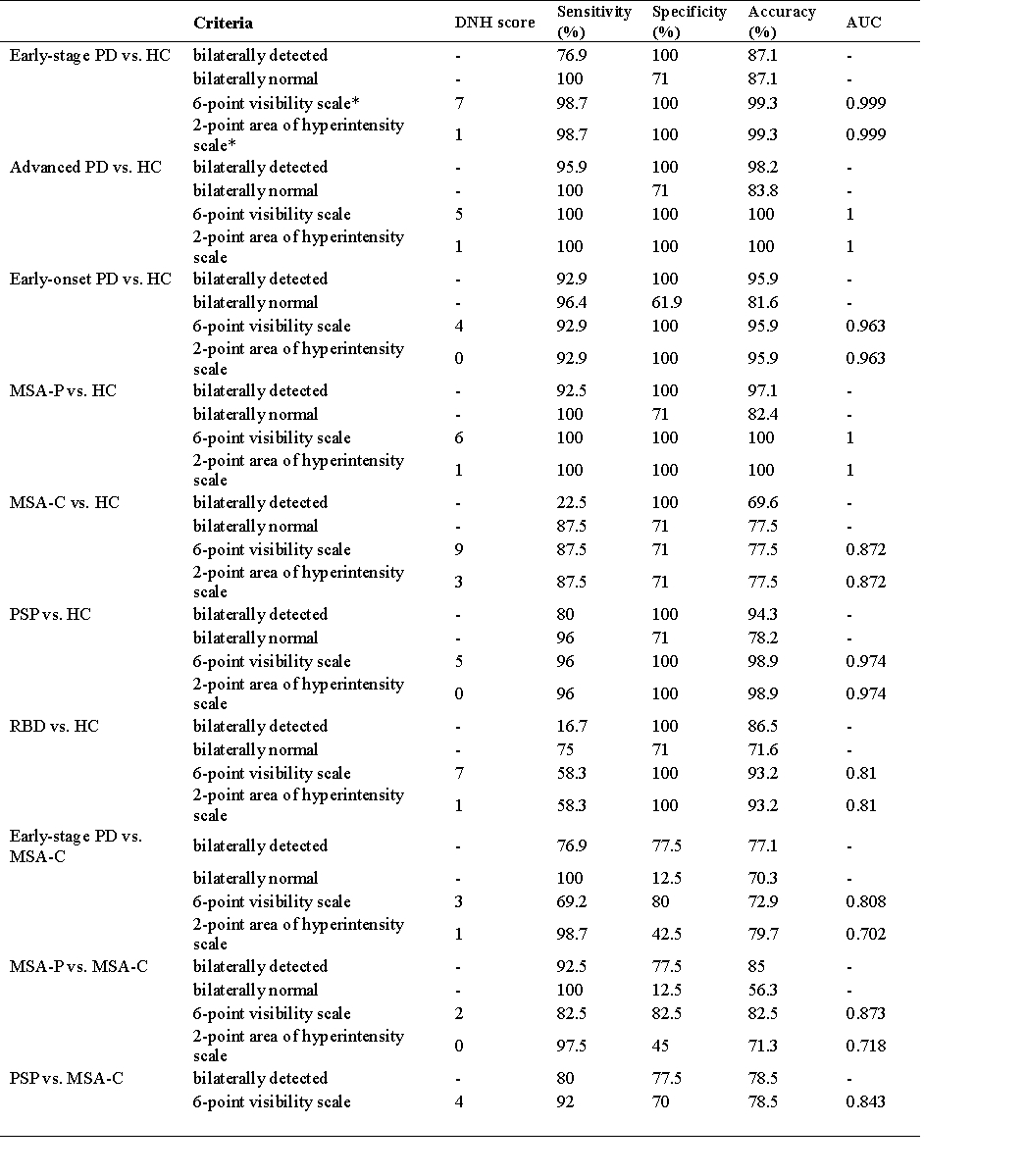
We identified bilateral presence of the DNH in 83 (100%) HC and 18 (23.1%) early-stage PD, 2 (4.1%) advanced PD, 2 (7.1%) early-onset PD, 10 (83.3%) RBD, 3 (7.5%) MSA-P, 31 (77.5%) MSA-C, and 5 (20.0%) PSP patients. The DNH scoring criteria exhibited high diagnostic performance in all disease groups while the dichotomously evaluation and scoring criteria of the DNH presented equal differential diagnostic performance for differential diagnosis of early-stage PD, MSA-P, and PSP from MSA-C. R2* mapping and principal component analysis of the substantia nigra demonstrated its different metal deposition patterns in PD of different stages and APs.Discussion
The current study aimed to investigate the diagnostic efficiency of the DNH abnormality at different stages of PD and APs. We found a higher bilateral perseverance rate of DNH in MSA-C (77.5%) and RBD (83.3%) compared with early-stage PD (23.1%), MSA-P (7.5%), and PSP (20.0%). A dopamine transporter SPECT study has demonstrated that MSA-C showing higher presynaptic nigrostriatal radiotracer uptake than PD and MSA-P. Combining with the evidence that loss of nigral hyperintensity is related to nigrostriatal dopaminergic degeneration indicated by another SPECT study, less dopaminergic neuron degeneration giving rise to distinctive iron deposition pattern in substantia nigra might explain the higher retaining rate of MSA-C. Further long-term prospective cohort studies are needed to follow the conversion of RBD to other neurodegenerative diseases and to evaluate the diagnosis accuracy of early-stage PD.Conclusion
MSA-C and RBD demonstrated significantly higher preservation rate of the DNH compared with PD, MSA-P, and PSP. The DNH scoring criteria could be considered an optimal diagnostic method of PD, RBD, MSA-P, MSA-C, and PSP. PD, MSA-P, MSA-C, and PSP patients showed different metal deposition patterns in the substantia nigra.Acknowledgements
This work was supported by the National Natural Science Foundation of China (No. 82271459 and No. 82071422) and Natural Science Foundation of Beijing Municipality (No. 7212031).
The authors report no competing interests.
References
1. Tolosa E, Garrido A, Scholz SW, Poewe W. Challenges in the diagnosis of Parkinson's disease. The Lancet Neurology 2021;20:385-397.
2. Weng YH, Yen TC, Chen MC, et al. Sensitivity and specificity of 99mTc-TRODAT-1 SPECT imaging in differentiating patients with idiopathic Parkinson's disease from healthy subjects. Journal of nuclear medicine : official publication, Society of Nuclear Medicine 2004;45:393-401.
3. Blazejewska AI, Schwarz ST, Pitiot A, et al. Visualization of nigrosome 1 and its loss in PD: pathoanatomical correlation and in vivo 7 T MRI. Neurology 2013;81:534-540.
4. Kwon DH, Kim JM, Oh SH, et al. Seven-Tesla magnetic resonance images of the substantia nigra in Parkinson disease. Ann Neurol 2012;71:267-277.
5. Kim EY, Sung YH, Shin HG, Noh Y, Nam Y, Lee J. Diagnosis of Early-Stage Idiopathic Parkinson's Disease Using High-Resolution Quantitative Susceptibility Mapping Combined with Histogram Analysis in the Substantia Nigra at 3 T. J Clin Neurol 2018;14:90-97.
6. Cheng Z, Zhang J, He N, et al. Radiomic Features of the Nigrosome-1 Region of the Substantia Nigra: Using Quantitative Susceptibility Mapping to Assist the Diagnosis of Idiopathic Parkinson's Disease. Front Aging Neurosci 2019;11:167.
7. Schwarz ST, Mougin O, Xing Y, et al. Parkinson's disease related signal change in the nigrosomes 1-5 and the substantia nigra using T2* weighted 7T MRI. Neuroimage Clin 2018;19:683-689.
8. Gupta R, Kumar G, Kumar S, Thakur B, Tiwari R, Verma AK. The Swallow Tail Sign of Substantia Nigra: A Case-Control Study to Establish Its Role in Diagnosis of Parkinson Disease on 3T MRI. J Neurosci Rural Pract 2022;13:181-185.
9. Noh Y, Sung YH, Lee J, Kim EY. Nigrosome 1 Detection at 3T MRI for the Diagnosis of Early-Stage Idiopathic Parkinson Disease: Assessment of Diagnostic Accuracy and Agreement on Imaging Asymmetry and Clinical Laterality. AJNR Am J Neuroradiol 2015;36:2010-2016.
10. Sung YH, Noh Y, Lee J, Kim EY. Drug-induced Parkinsonism versus Idiopathic Parkinson Disease: Utility of Nigrosome 1 with 3-T Imaging. Radiology 2016;279:849-858.
11. Wang N, Liu XL, Li L, et al. Screening for Early-Stage Parkinson's Disease: Swallow Tail Sign on MRI Susceptibility Map-Weighted Images Compared With PET. J Magn Reson Imaging 2021;53:722-730.
12. Bae YJ, Kim JM, Kim E, et al. Loss of Nigral Hyperintensity on 3 Tesla MRI of Parkinsonism: Comparison With (123) I-FP-CIT SPECT. Mov Disord 2016;31:684-692.
13. Poewe W, Stankovic I, Halliday G, et al. Multiple system atrophy. Nature reviews Disease primers 2022;8:56.
14. Jellinger KA, Seppi K, Wenning GK. Grading of neuropathology in multiple system atrophy: proposal for a novel scale. Mov Disord 2005;20 Suppl 12:S29-36.
15. Sakakibara S, Hashimoto R, Katayama T, et al. Longitudinal Change of DAT SPECT in Parkinson's Disease and Multiple System Atrophy. Journal of Parkinson's disease 2020;10:123-130.
Figures
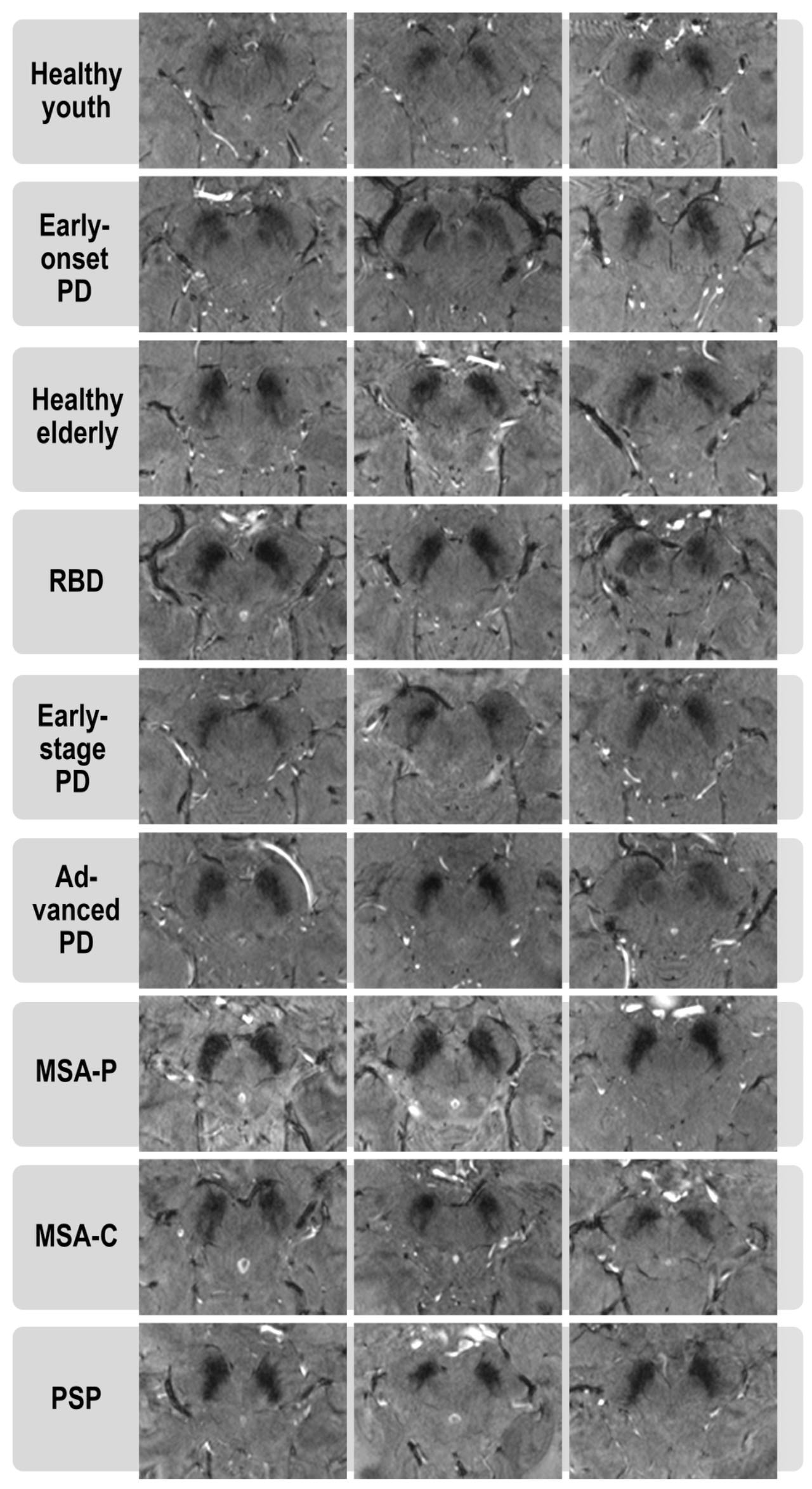
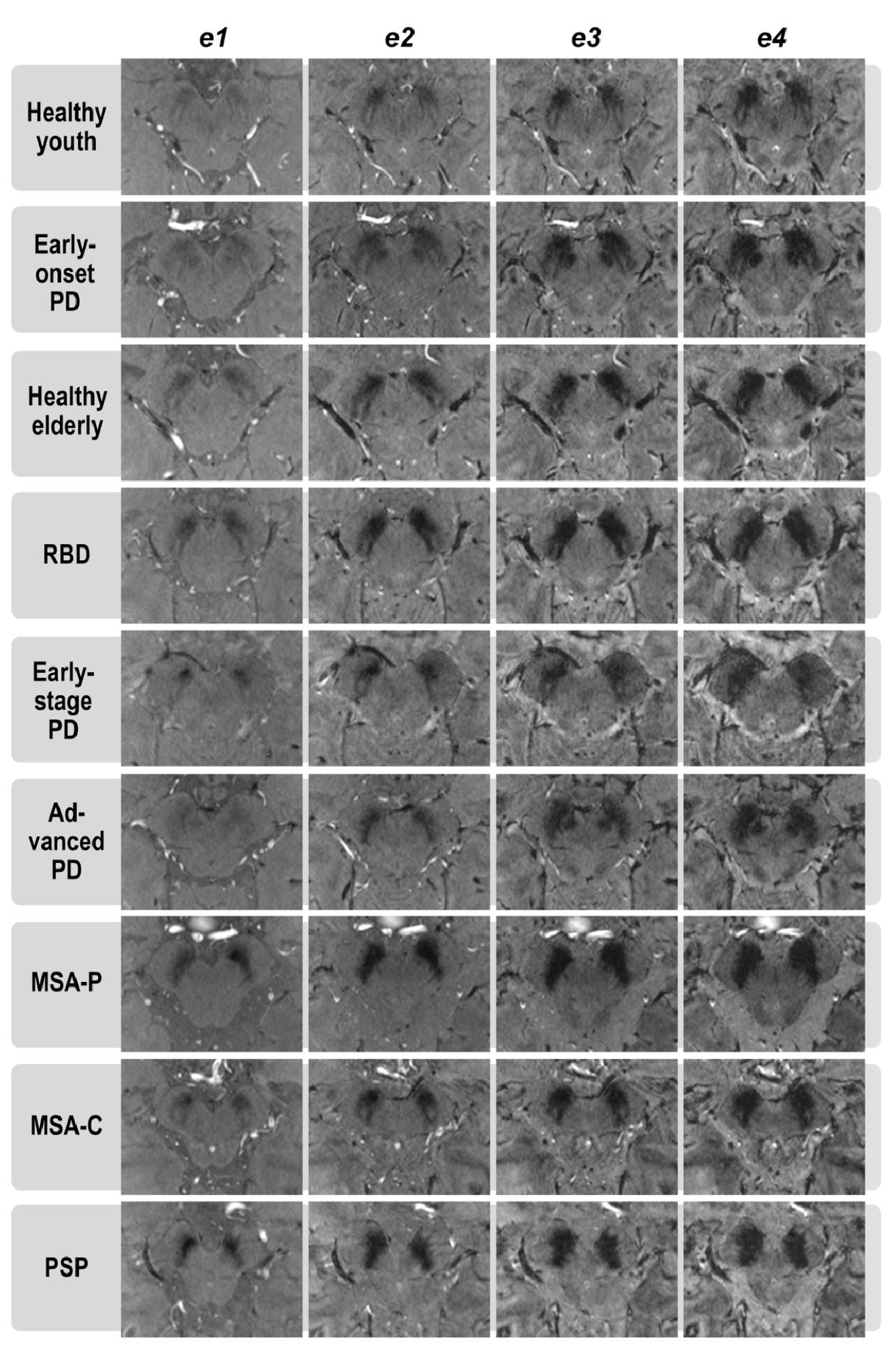
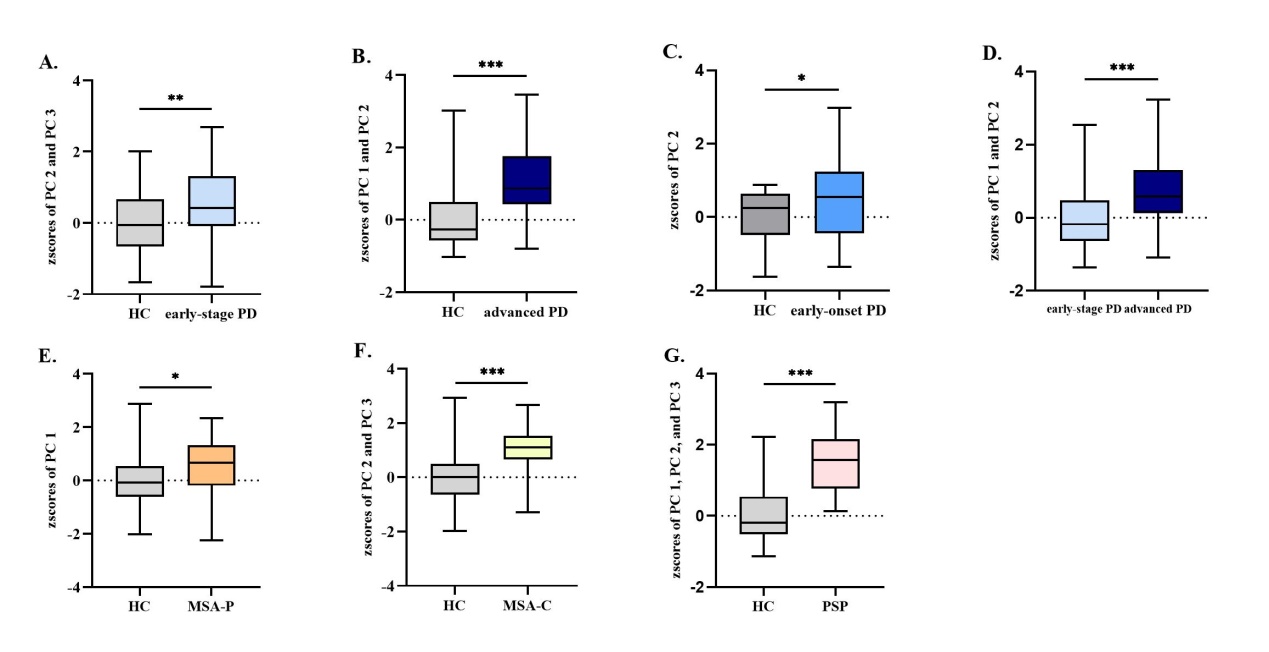
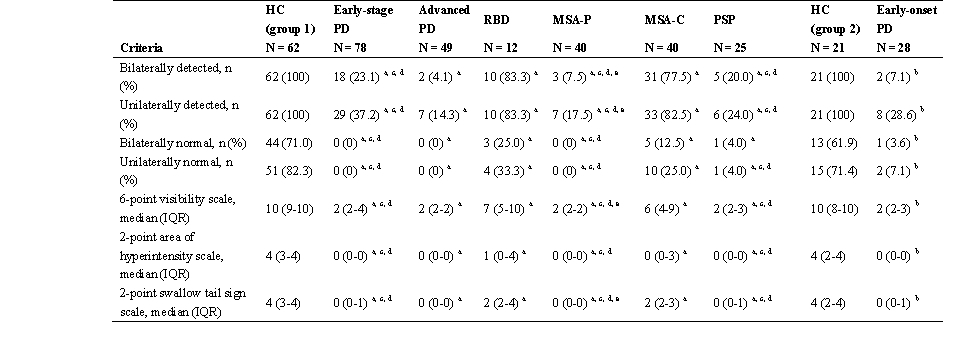
Table 1 Visual assessment of the DNH in patients and controls groups at echo 2
a p < 0.05 compared with HC.
b p < 0.05 compared with HC.
c p < 0.05 compared with RBD.
d p < 0.05 compared with MSA-C.
e p < 0.05 compared with early-stage PD.