4384
Accuracy of AI-driven susceptibility map-weighted MRI analyses to differentiate neurodegenerative from non-neurodegenerative parkinsonism1Department of Radiology and Nuclear medicine, Amsterdam UMC, University of Amsterdam, Amsterdam, Netherlands, 2Department of Radiology and Nuclear medicine, Amsterdam UMC, Vrije Universiteit Amsterdam, Amsterdam, Netherlands, 3Department of Neurology, Amsterdam UMC, University of Amsterdam, Amsterdam, Netherlands, 4'Heuron Co., Ltd., Seoul, Korea, Republic of, 5Department of Neurology, Gachon University College of Medicine, Incheon, Korea, Republic of, 6Department of Neurology, Spaarne Gasthuis, Haarlem, Netherlands, 7Department of Neurology, Flevoziekenhuis, Almere, Netherlands, 8Department of Neurology, Amsterdam UMC, Vrije Universiteit Amsterdam, Amsterdam, Netherlands
Synopsis
Keywords: Parkinson's Disease, Parkinson's Disease
Motivation: Susceptibility map-weighted imaging (SMWI) of the substantia nigra is a novel MRI sequence that has the potential to aid the diagnosis of patients with clinically uncertain parkinsonian syndromes (CUPS).
Goal(s): To investigate the accuracy of AI-driven automated SMWI software in a clinically relevant population.
Approach: We acquired SMWI in patients who received a dopamine transporter (DAT)-SPECT because of CUPS. The diagnostic software (Heuron IPD) results were compared with the DAT-SPECT results as a reference.
Results: Preliminary analysis of 120 patients demonstrated an accuracy of 88% for the diagnostic software to differentiate neurodegenerative from non-neurodegenerative parkinsonism in patients who presented with CUPS.
Impact: Susceptibility map-weighted imaging (SMWI) demonstrates a diagnostic accuracy of 88% in patients with clinically uncertain parkinsonian syndromes (CUPS). These findings are promising for the use of SWMI as diagnostic marker and warrant prospective studies in CUPS patients.
Introduction
Parkinson’s disease (PD) is characterized by degeneration of the dopaminergic cells in the substantia nigra (SN), particularly in the cell dense nigrosome-1 area, and is associated with locally increased iron deposition.1 In general, PD is diagnosed based on clinical symptoms. The accuracy of an initial clinical diagnosis by an expert is estimated at 81.5%.2 In patients with a clinically uncertain parkinsonian syndrome (CUPS) molecular imaging may be a helpful tool to aid in achieving an accurate diagnosis.MRI is currently used in the diagnostic trajectory to image structural abnormalities (e.g., stroke) as a cause for the symptoms, but not for the assessment of nigrostriatal degeneration in PD. Susceptibility map-weighted imaging (SMWI) is a novel MRI sequence that combines magnitude images with quantitative susceptibility mapping to enhance the contrast of nigrosome-1 and loss of its signal in neurodegenerative parkinsonian patients due to iron deposition and has the potential to aid in the diagnosis of patients with CUPS.3 Previous studies show a high diagnostic accuracy. 4,5 However, visual assessment can be challenging and these studies included patients with parkinsonism in general, and were not focused on patients with CUPS, who are referred for dopamine transporter (DAT) imaging in routine clinical practice. In this study, we aimed to assess the diagnostic accuracy of AI-driven diagnostic SMWI software in patients who presented with CUPS.
Methods
A diagnostic accuracy study was performed. Patients with parkinsonism who visited a neurologist and had a dopamine transporter (DAT) SPECT scan because of CUPS between January 2019 and July 2023 were approached to participate in the study.The index test was the result (normal or abnormal) of AI-driven diagnostic software (Heuron IPD, formerly known as mPDia) analysis of the nigrosome-1 area on the SMWI sequence. The reference standard was the result of the DAT-SPECT scan as reported by a nuclear medicine physician.
MRI scans were acquired on a 3T Philips MRI system between May 2022 and September 2023, including a SMWI. The SMWI was scanned with a FOV=192x192x32mm, voxel size=0.5x0.5x1.0mm, FA=20°, TR=49.1ms, TE=14ms, echo spacing=13ms. The quality of the MRI scans were visually inspected. SMWI scans with severe artifacts were excluded.
Clinical assessments and questionnaires were acquired after the MRI scan and obtained by a single observer. Motor symptoms were assessed with the MDS Unified Parkinson's Disease Rating Scale III (MDS-UPDRS III), depressive symptoms with the Beck Depression Inventory (BDI), and cognition with the Montreal cognitive assessment (MoCA).
Results
A total of 132 patients are currently enrolled in this study, 53 with an abnormal and 67 with a normal DAT-SPECT scan. Twelve were excluded for analysis, four because no final diagnosis could be established, and eight because of severe artifacts on MRI. The study population consisted of 45 females and 75 males with a mean age of 67.5 years (SD ± 10.6) with no significant age differences between groups. Mean time between DAT-SPECT scan and MRI scan was 1.56 years (SD ± 1.15). A list of the final diagnoses of the patients is presented in table 1.Preliminary analysis demonstrated a diagnostic accuracy of 88% of the AI-driven software analysis of SMWI compared to DAT-SPECT scan results to differentiate neurodegenerative from non-neurodegenerative parkinsonism, with a sensitivity of 87% and specificity of 89% in patients who presented with CUPS.
The mean MDS-UPDRS III scores were 27.3 and 27.1, mean BDI scores were 10.4 and 10.0 and mean MoCA scores were 23.8 and 23.1 for patients with an abnormal and normal DAT-SPECT scan result respectively, none of these scores were significantly different between groups.
Discussion
The diagnostic accuracy was 88% in this study. Although this is slightly lower than previous research, it might offer a more realistic representation of clinical practice.4,5 Since the population of this study solely consisted of patients who presented with CUPS and did not exclude patients based on diagnosis or comorbidity.A limitation of this study is the average delay between index test and reference test of 1.6 years. Future prospective studies performing both tests at the same time could contribute to further investigate the diagnostic accuracy of CUPS patients in clinical practice. In this study DAT-SPECT scans are used as a reference test as it is considered to be widely acknowledged in clinical practice with a high diagnostic accuracy for nigrostriatal degeneration, however, four participants (3.2%) had inconclusive DAT-SPECT results. A longer follow-up or pathological confirmation could aid the reference test.
Conclusion
The diagnostic accuracy of novel SMWI based diagnostic software is promising in a clinically relevant population of patients who presented with CUPS.Acknowledgements
-References
1. Griffiths PD, Dobson BR, Jones GR, Clarke DT. Iron in the basal ganglia in Parkinson's disease: An in vitro study using extended X-ray absorption fine structure and cryo-electron microscopy. Brain 1999; 122(4): 667-73.
2. Rizzo G, Copetti M, Arcuti S, Martino D, Fontana A, Logroscino G. Accuracy of clinical diagnosis of Parkinson disease: A systematic review and meta-analysis. Neurology 2016; 86(6): 566-76.
3. Gho SM, Liu C, Li W, Jang U, Kim EY, Hwang D, Kim DH. Susceptibility map-weighted imaging (SMWI) for neuroimaging. Magn Reson Med 2014; 72(2): 337-46.
4. Shin DH, Heo H, Song S, et al. Automated assessment of the substantia nigra on susceptibility map-weighted imaging using deep convolutional neural networks for diagnosis of Idiopathic Parkinson's disease. Parkinsonism & Related Disorders 2021; 85: 84-90.
5. Sung YH, Kim J-S, Yoo S-W, et al. A prospective multi-centre study of susceptibility map-weighted MRI for the diagnosis of neurodegenerative parkinsonism. European Radiology 2022; 32(5): 3597-608.
Figures
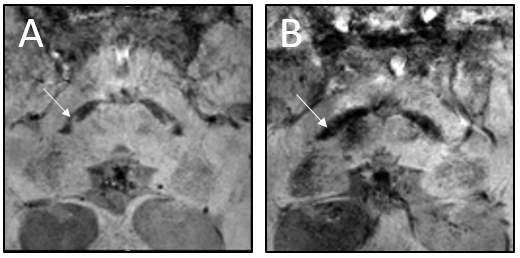
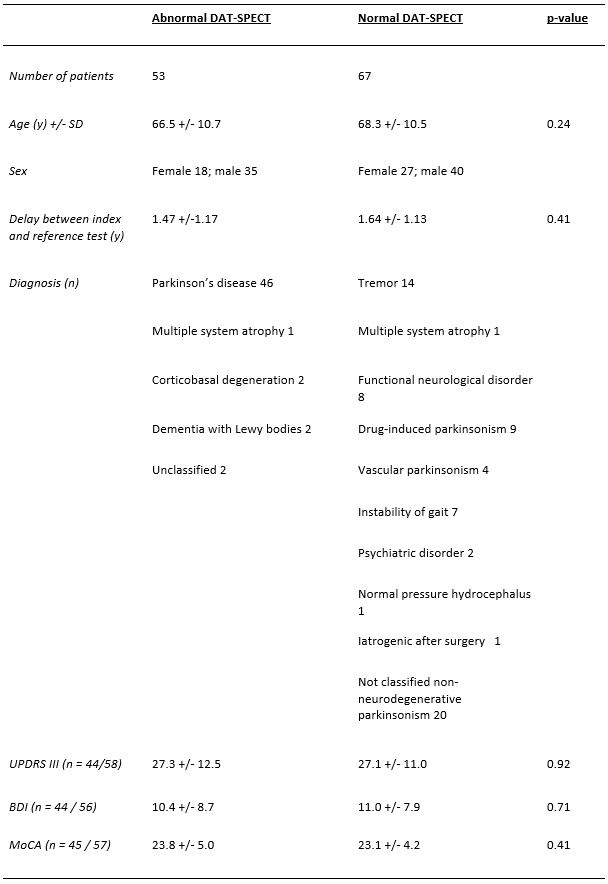
Table 1, patient characteristics. (y) = years, SD = standard deviation, UPDRS = unified Parkinson's disease rating scale, BDI = Beck depression Inventory, MoCA = Montreal Cognitive Assessment.
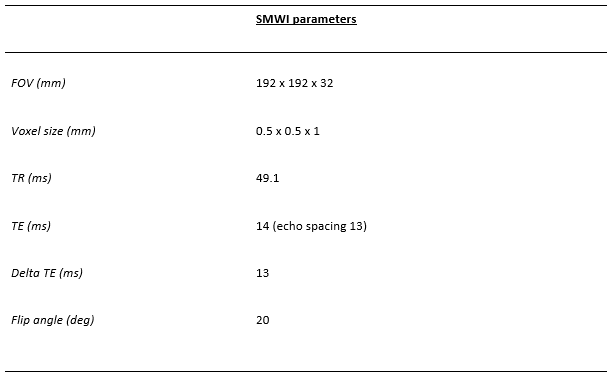
Table 2, SMWI parameters. FOV = field of view, TR = repetition time, TE = Time to Echo
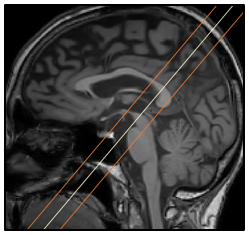
Figure 3, planning of the field of view of the SMWI sequence, midline from the posterior commissure to the top of the pons.