4380
Iron deposition of basal ganglia on 7 Tesla MRI for diagnosis of early-stage Parkinson’s disease1Center for Movement Disorders, Department of Neurology, Beijing Tiantan Hospital, Capital Medical University, Beijing, China, 2China National Clinical Research Center for Neurological Diseases, Beijing, China, 3Tiantan Neuroimaging Center of Excellence, Beijing Tiantan Hospital, Capital Medical University, Beijing, China, 4MR Research Collaboration Team, Siemens Healthineers, Beijing, China
Synopsis
Keywords: Parkinson's Disease, Parkinson's Disease
Motivation: Early diagnosis of Parkinson's disease (PD) remains challenging.
Goal(s): Aimed to identify new imaging features in the basal ganglia of PD by 7T iron-sensitive MRI, and to investigate the diagnostic performance of the new imaging features in distinguishing early-stage PD patients from healthy subjects.
Approach: 129 participants were prospectively recruited between May 2021 and September 2023. All participants were scanned at Tiantan Neuroimaging Center using 7-Tesla MRI. Two neuroradiologist separately evaluated the visual rating scale of iron deposition signs in basal ganglia.
Results: The newly developed basal ganglia sign scoring scale showed high sensitivity and excellent specificity for diagnosis of early-stage PD.
Impact: The distribution characteristics of iron deposition in basal ganglia might be a promising marker of the diagnosis of early-stage PD.
Introduction
Parkinson’s disease (PD) patients have a specific pattern of iron deposition in the brain, especially in the substantia nigra and basal ganglia [1], which provides significant value in the early diagnosis of PD. Seven-tesla (7T) iron-sensitive magnetic resonance imaging (MRI) has higher spatial resolution and sensitivity, allowing for more accurate observation of changes in brain microstructure and providing imaging support for visual analysis of iron deposition in subcortical nuclei [2]. Previous studies have mainly focused on quantitative detection of iron deposition in the brain of patients with PD [3], but few researches have been conducted to explore the imaging features of basal ganglia iron deposition in PD patients. We aimed to identify new imaging features in the basal ganglia of PD by 7T iron-sensitive MRI, and to investigate the diagnostic performance of the new imaging features in distinguishing early-stage PD patients from healthy subjects.Methos
67 early-stage PD patients, 16 idiopathic rapid eye movement sleep behavior disorder (RBD) patients, and 46 healthy controls (HC) were prospectively recruited in the movement disorder center of the Beijing Tiantan Hospital (Beijing, China), between May 2021 and September 2023. All participants were scanned at Tiantan Neuroimaging Center using 7-Tesla MRI (MAGNETOM Terra, Siemens Healthcare, Erlangen, Germany) with a 32-channel Rx/8Tx head coil (Nova Medical, Wilmington, Massachusetts, USA). The MRI protocol included the high-resolution SWI (transverse scan, acquisition voxel = 0.3×0.3×1.2 mm3, 104 slices, TE = 12 ms, TR = 19 ms, flip angle = 14°, acceleration factor = 3, scan time = 6:47), T1-weighted imaging (sagittal scan, acquisition voxel = 0.7×0.7×0.7 mm3, 256 slices, TI = 1050 ms, TR = 2200 ms, flip angle = 6°, acceleration factor = 2, scan time = 6:12), and T2-weighted imaging (transverse scan, acquisition voxel = 0.3×0.4×3 mm3, 42 slices, TE = 81 ms, TR = 3500 ms, acceleration factor = 3, scan time = 2:57). The visual rating scale of iron deposition signs in basal ganglia was evaluated separately by two neuroradiologist.Results
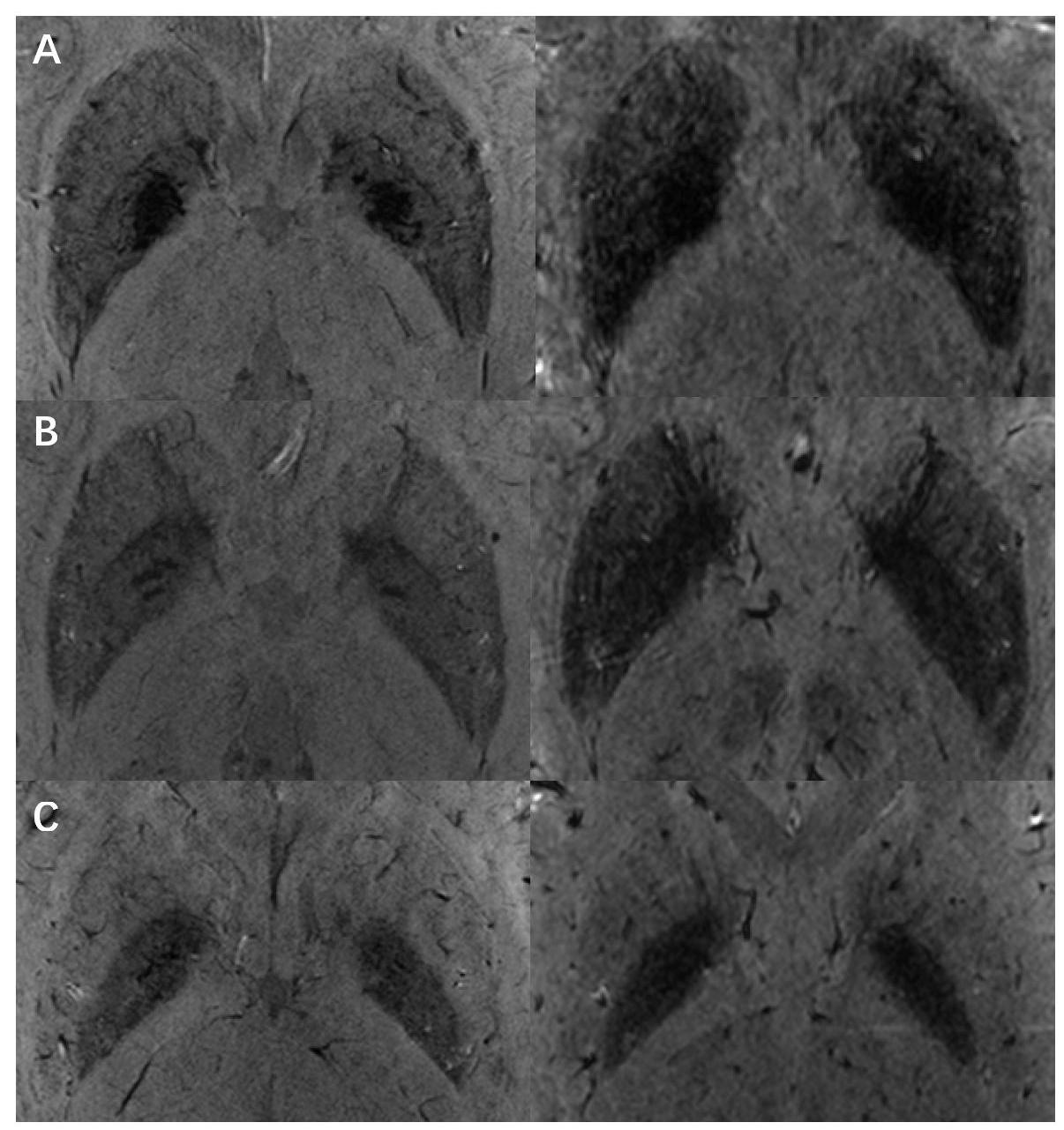
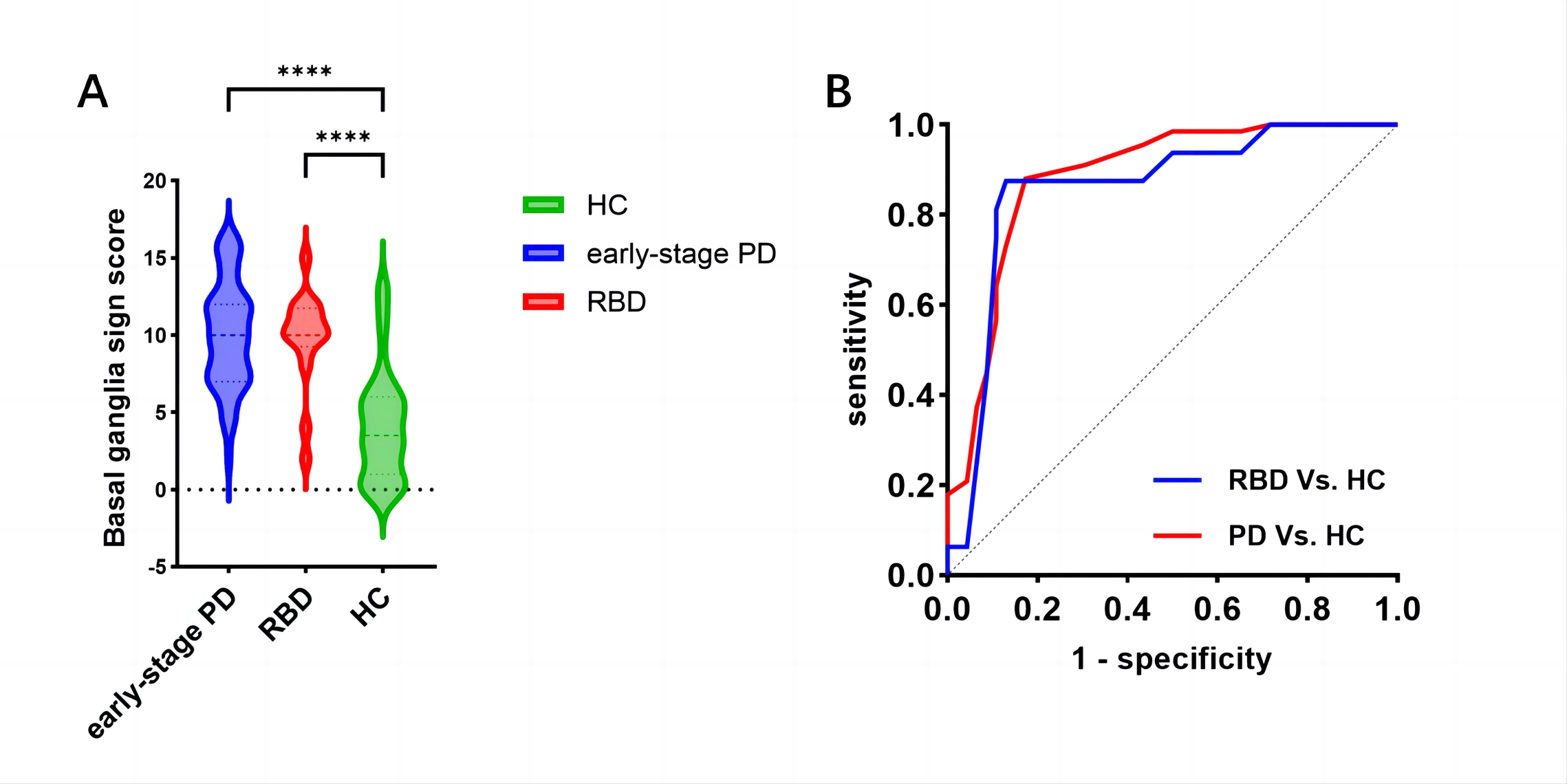
We identified three signs of iron deposition in the basal ganglia of PD patients on the SWI images (Figure 1): 1) the signal intensity of the posterior putamen and posterior globus pallidus tended to be consistent, termed “posterior putamen isointense sign”; 2) irregular patchy low-signal changes in the anterior globus pallidus, termed “hypointense anterior globus pallidus sign”; 3) linear low-signal changes in the anterior lateral margin of the globus pallidus, termed “hypointense globus pallidus rim sign”. In addition, we found that the putamen and globus pallidus signal intensities converged on T2* images in PD patients, termed as “putamen isointense sign” (Figure 1).A basal ganglia sign scoring scale was established based on the four imaging features described above. The basal ganglia sign score of early-stage PD patients was significantly higher than that of HC (10.09 ± 3.38 vs. 4.13 ± 3.53, P < 0.001, Figure 3A). The receiver operating characteristic (ROC) analysis showed that the optimal cut-off point was 6.5, the area under the curve (AUC) was 0.884, the diagnostic sensitivity and specificity was 88.1% and 82.6%, respectively (Figure 3B). Compared with the HC, elevated basal ganglia sign scores were investigate in RBD patients (9.81 ± 4.37 vs. 4.13 ± 3.53, P < 0.001, Figure 3A), with an optimal cut-off point of 6.5, AUC of 0.859, sensitivity of 87.5%, and specificity of 82.6% (Figure 3B). No significant difference was observed between early-stage PD and RBD patients (Figure 3A).
Discussion
Based on 7T iron-sensitive MRI, we found that PD patients and RBD patients exhibited different iron deposition distribution characteristics in the basal ganglia compared to HC, which was corresponded to previous neuropathological studies. And the newly developed scoring criteria of the imaging feature via visual assessment was demonstrated high sensitivity and specificity for distinguishing early-stage PD from HC, suggesting this rating scale can be potentially useful for diagnosis of early-stage PD. However, there was no significant difference between early-stage PD and RBD patients, which may be related to the longer disease course of RBD patients included in the study. Quantitative analysis of the signs in the basal ganglia is needed to further validate the diagnostic efficacy of the newly rating scale.Conclusion
The newly developed basal ganglia sign scoring scale showed high sensitivity and excellent specificity for diagnosis of early-stage PD. Future quantitative analysis will help to fully evaluate and understand these characteristics.Acknowledgements
No acknowledgement found.References
1.Dexter DT, Carayon A, Javoy-Agid F, Agid Y, Wells FR, Daniel SE, et al. Alterations in the levels of iron, ferritin and other trace metals in Parkinson's disease and other neurodegenerative diseases affecting the basal ganglia. Brain : a journal of neurology. 1991;114 ( Pt 4):1953-75. doi: 10.1093/brain/114.4.1953.
2. Cong F, Liu X, Liu CJ, Xu X, Shen Y, Wang B, et al. Improved depiction of subthalamic nucleus and globus pallidus internus with optimized high-resolution quantitative susceptibility mapping at 7 T. NMR Biomed. 2020;33(11):e4382. doi: 10.1002/nbm.4382.
3. Barbosa JH, Santos AC, Tumas V, Liu M, Zheng W, Haacke EM, et al. Quantifying brain iron deposition in patients with Parkinson's disease using quantitative susceptibility mapping, R2 and R2. Magnetic resonance imaging. 2015;33(5):559-65. doi: 10.1016/j.mri.2015.02.021.
Figures