4371
Microscopic diffusion anisotropy as a predictor of cognitive decline in asymptomatic adults1F.M. Kirby Research Center for Functional Brain Imaging, Kennedy Krieger Research Institute, Baltimore, MD, United States, 2Russell H. Morgan Department of Radiology and Radiological Science, Johns Hopkins University School of Medicine, Baltimore, MD, United States, 3Department of Neurology, Johns Hopkins University School of Medicine, Baltimore, MD, United States, 4Department of Biomedical Engineering, Johns Hopkins University School of Medicine, Baltimore, MD, United States, 5Department of Electrical and Computer Engineering, Johns Hopkins University, Baltimore, MD, United States, 6Department of Medical Radiation Physics, Lund University, Lund, Sweden
Synopsis
Keywords: Dementia, Dementia
Motivation: Conventional diffusion MRI metrics like FA have limitations in assessing WMH lesions due to fiber orientation dispersion.
Goal(s): To improve MRI sensitivity to white matter integrity in WMH and assess its clinical relevance in predicting preclinical cognitive decline using advanced diffusion MRI.
Approach: FA and μFA maps were acquired in 54 adults using tensor-valued diffusion MRI and their quantitative correlation with cognitive decline were evaluated in WMH lesion and penumbra.
Results: While both μFA and FA differentiated WMH from other white matter regions, μFA demonstrated greater sensitivity to predict cognitive decline, suggesting its added specificity to probe white matter integrity in WMH.
Impact: Enhanced sensitivity of μFA to subtle white matter integrity and clinical aspect may offer better understanding of underlying histopathological alterations in white WMH, helping earlier detection of cerebrovascular pathology and aiding efforts to identify at-risk individuals and guide timely interventions.
Introduction
Cognitive decline can precede clinical detection of cognitive impairment, rendering early detection of disease symptoms essential for timely intervention to slow risk of progression1-3.Cerebrovascular small-vessel disease (cSVD), known to be associated with cognitive decline and dementia4,5, has emerged as an etiology of cognitive decline and is a target of disease modifying treatment6-8.In neuroimaging studies, white matter hyperintensities (WMHs), typically visible in deep or periventricular white matter in T2-weighted FLAIR, are indicative of white matter pathologies related to cSVD, such as axonal loss and demyelination7,9,10, demonstrating its association with cognitive decline and cardiovascular risk factors11-13. However, WMH may represent the final visible stage of the continuous course of microstructural WM degeneration14. To understand the underlying WM alterations, conventional diffusion MRI parameters, such as fractional anisotropy (FA), have been studied to probe white matter integrity within WMH14. Despite its usefulness, the interpretation of FA is confounded by intra-voxel fiber orientation dispersion, which is prevalent across brain WM. Recent developments in diffusion MRI introduced the concept of microscopic FA (μFA), capable of capturing microscale-level diffusion anisotropy and offering a more specific characterization of white matter microstructure integrity15, independent of fiber orientation dispersion16,17.
In this study, we hypothesized that μFA will provide a stronger sensitivity to white matter degeneration compared to FA, given its superior specificity to subtle WM alterations, and compared the clinical relevance of μFA within WMH to that of FA for detecting preclinical cognitive decline. Our results demonstrated that μFA had superior sensitivity to clinical aspects over FA.
Methods
[Participants] Local IRB authorization was obtained, and all volunteers signed informed consent. This perspective study included 54 participants (age = 61.2 ± 9.8 y/o, 39 female) who are healthy family members or relatives with known early-onset coronary disease.[Data acquisition] 54 participants underwent 3T brain MRI (Philips Ingenia-Elition-RX), including MPRAGE, T2-weighted FLAIR, and T2-weighted images for WMH lesion assessment and tensor-valued diffusion MRI (tdMRI) for μFA estimation. tdMRI was acquired using linear, planar, and spherical b-tensors generated by optimized gradient waveforms17,18, using the following scan parameters: resolution=1.8 mm-isotropic, max b-value = 2000 s/mm2.
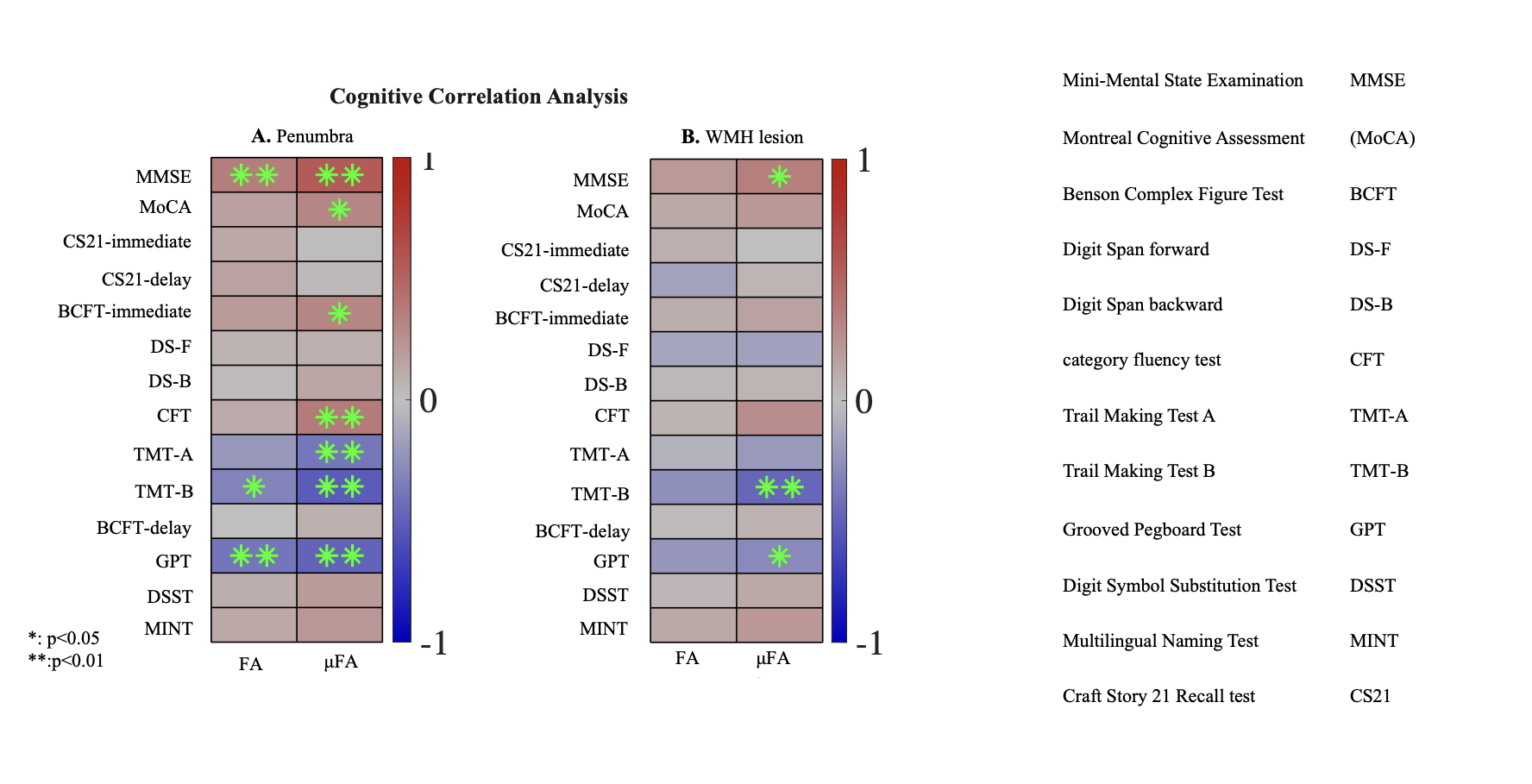
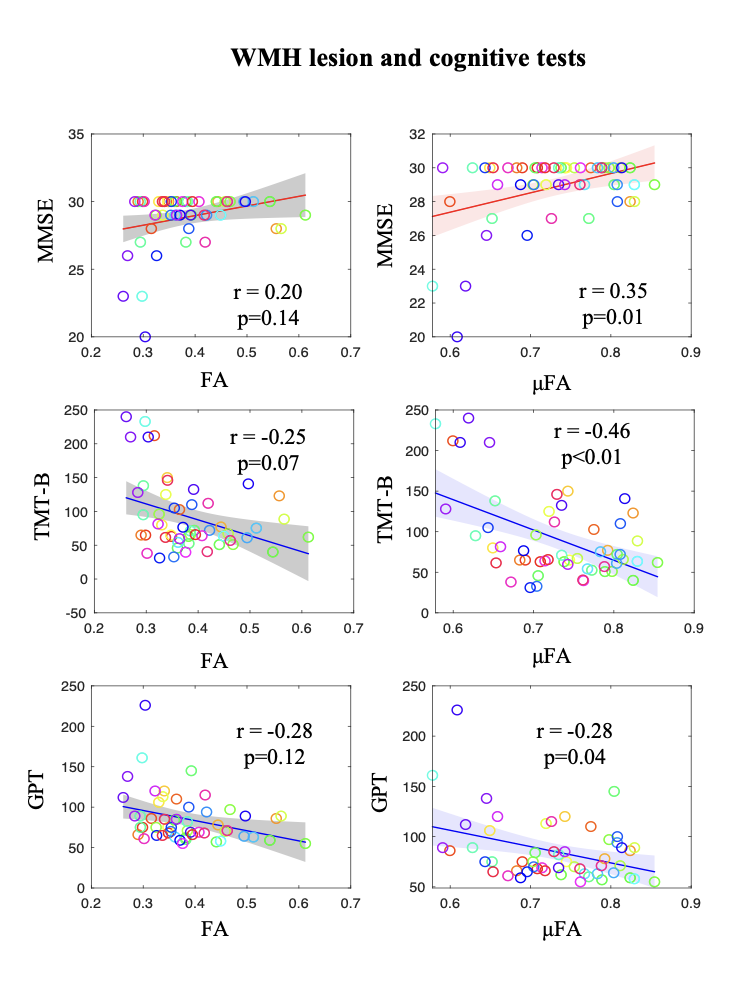
[Clinical assessment] Neuropsychological tests to assess cognitive function and impairment included 14 assessments (MMSE/MoCA/CS21-immediate/CS21-delay/BCFT-immediate/ BCFT -delay/DS-F/DS-B/CFT/TMT-A/TMT-B/GPT/DSST/MINT; Fig.4). TMT and GPT are timed test, positively correlated with cognitive decline (others negative correlated).
[Postprocessing] Diffusion-weighted images from tdMRI were corrected for noise, signal drift, Gibbs-ringing, motion, and distortion19-23, before calculating FA and μFA maps using the open-source analysis framework (https://github.com/markus-nilsson/md-dmri).
[ROI analysis] For WMH lesion segmentation, MPRAGE, FLAIR, T2-weighted images were sequentially bias-corrected24, interpolated for 2D scans 25, co-registered to standard space, and then contrast-harmonized 26. The preprocessed contrast was segmented for WMH lesion using domain-adaptable segmentation model 27. Surrounding penumbra was defined as white matter tissue surrounding the lesions (2-voxel thickness). The remaining white matter, other than WMH and penumbra, was considered normal appearing white matter (NAWM). Pearson partial correlation with neuropsychological test outcomes were assessed for the averaged FA and μFA values in each ROI (WMH, penumbra, and NAWM), adjusting age and sex.
Results
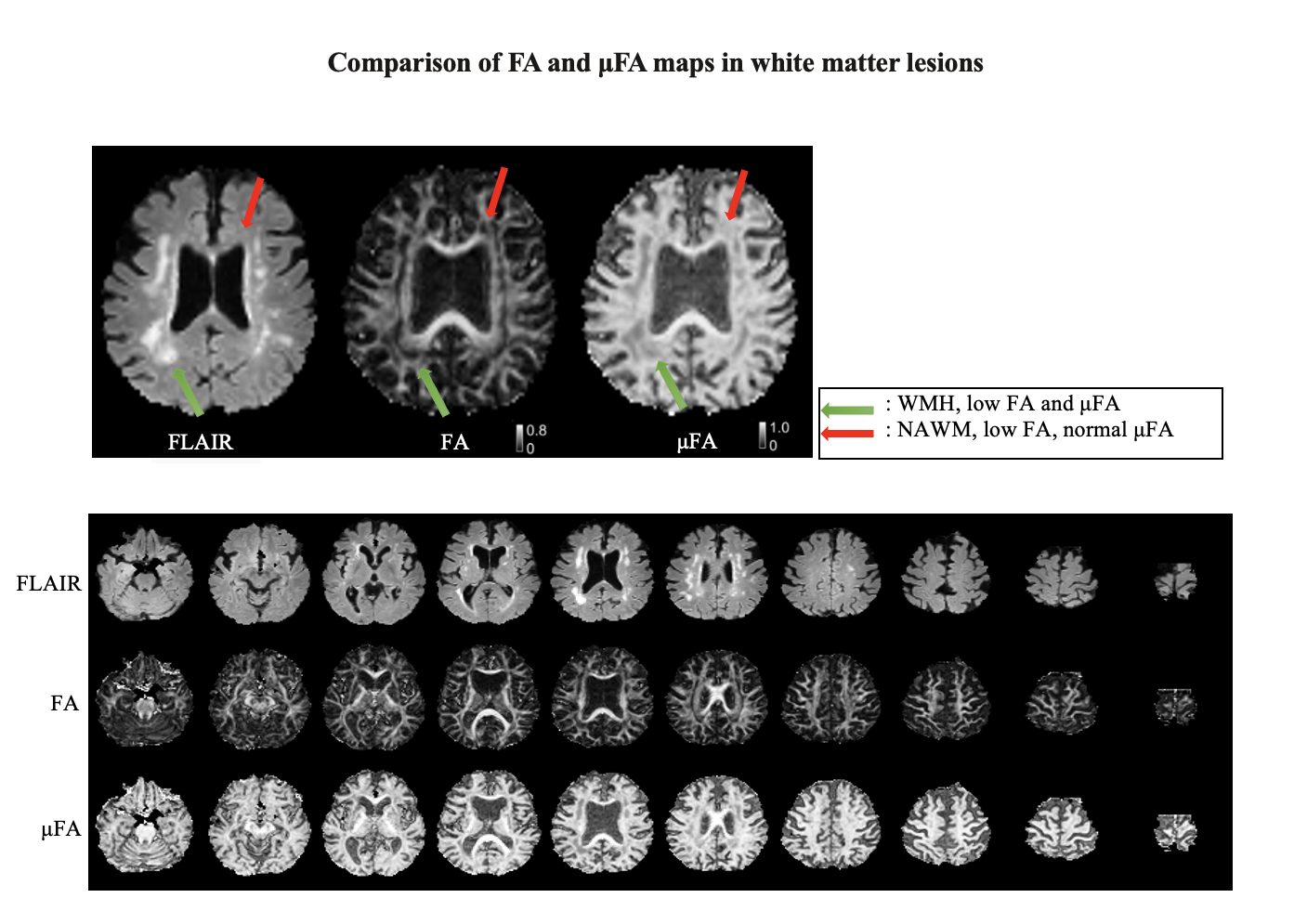
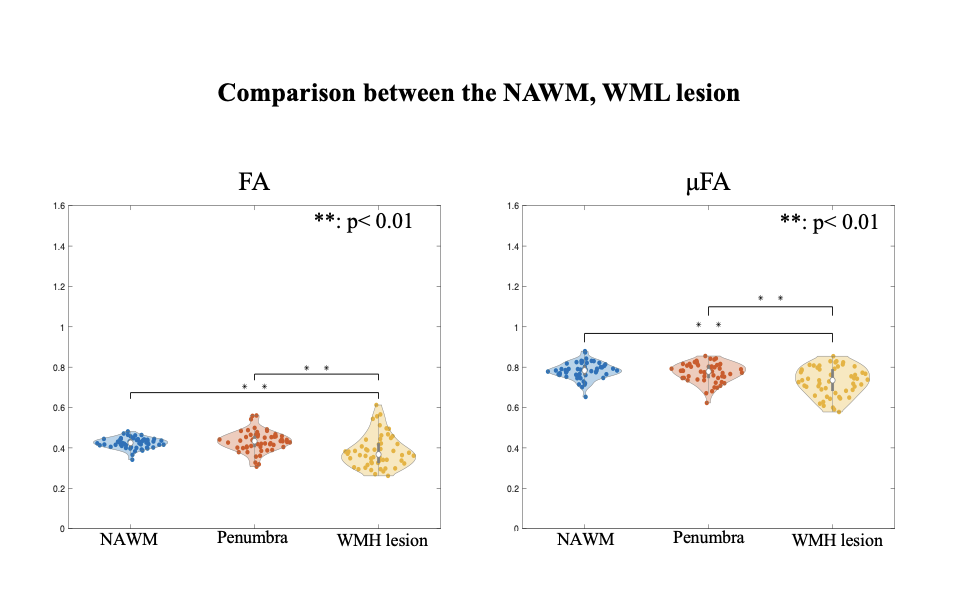
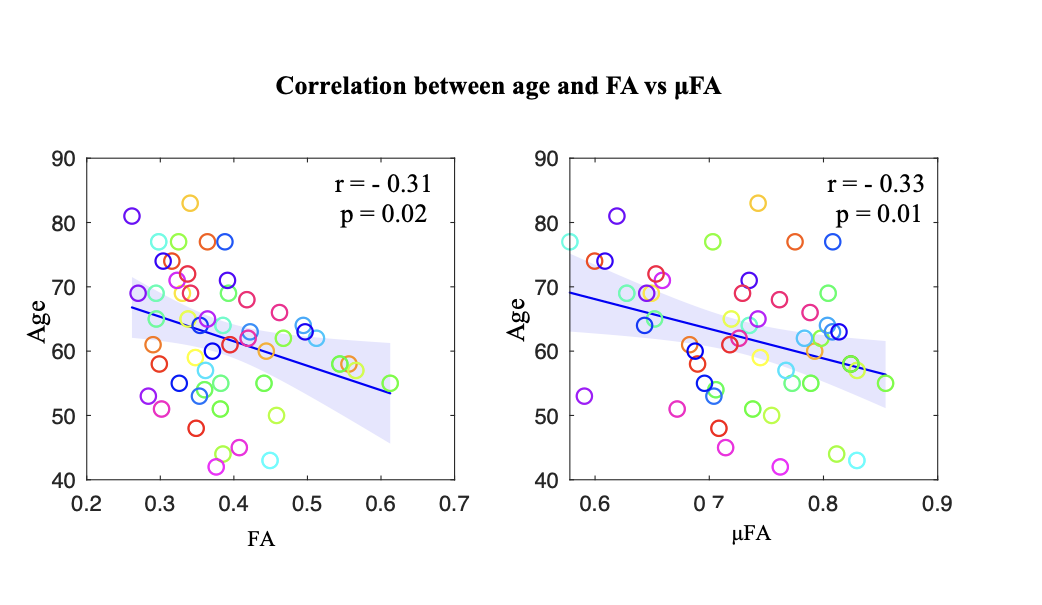
Fig.1 shows the appearance of FA and μFA in WMH lesions. FA maps show the detrimental effects of intra-voxel orientation dispersion in crossing fiber areas (red arrows in Fig. 1), hampering the identification of changes in microstructure in WMH lesions. Conversely, μFA shows hypointensities localized in WMH lesion sites, regardless of crossing fiber. When combining all WMH lesions, FA and μFA show similar sensitivity to differentiate WMH with penumbra or NAWM, reporting significant (p<0.01) decrease of μFA and FA in WMH (Fig.2)Both FA and μFA in WMH lesions show significant decrease with age (Fig.3), highlighting the potential of diffusion MRI metrics, particularly μFA, to serve as biomarkers of age-related WMH.
Despite the similar performance of both parameters (FA and μFA) in terms of quantitative differentiation of WMH from other WM, μFA in WMH demonstrated superior clinical sensitivity to detect cognitive decline over FA (Figs. 4,5). In WMH lesions and their penumbra, changes in μFA and FA were quantitatively associated with multiple cognitive impairment metrics (p<0.05), with higher sensitivity in μFA. This may indicate that the enhanced specificity of μFA to white matter integrity can provide better insight into understanding white matter alterations in cSVD. Fig.5 displays scatter plots for FA and μFA in WMH, with unique correlation for μFA across multiple domains.
Conclusion/discussion:
This study found a more sensitive characterization of clinical outcome with μFA compared to conventional FA measurement. These results suggest μFA may be a valuable predictor of future cognitive decline in adults even before symptoms appear, potentially enabling earlier interventions.Acknowledgements
COI*
Peter van Zijl has research support from and technology licensed to Philips Healthcare and has also been a paid speaker. Linda Knutsson is conflicted by affiliation. Filip Szczepankiewicz is an inventor on patents related to the study, and he has financial interests in the company Random Walk Imaging AB
Funding:
National Institutes of Health grants: NINDS/NIA award RF1NS128135 and NIBIB award P41 EB031771.
References
1. Sperling RA, Aisen PS, Beckett LA, Bennett DA, Craft S, Fagan AM, et al. Toward defining the preclinical stages of Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimer's & dementia. 2011;7(3):280-92.
2. Jack CR, Knopman DS, Jagust WJ, Petersen RC, Weiner MW, Aisen PS, et al. Tracking pathophysiological processes in Alzheimer's disease: an updated hypothetical model of dynamic biomarkers. The lancet neurology. 2013;12(2):207-16.
3. Bateman RJ, Xiong C, Benzinger TL, Fagan AM, Goate A, Fox NC, et al. Clinical and biomarker changes in dominantly inherited Alzheimer's disease. New England Journal of Medicine. 2012;367(9):795-804.
4. Corriveau RA, Bosetti F, Emr M, Gladman JT, Koenig JI, Moy CS, et al. The Science of Vascular Contributions to Cognitive Impairment and Dementia (VCID): A Framework for Advancing Research Priorities in the Cerebrovascular Biology of Cognitive Decline. Cellular and molecular neurobiology. 2016;36(2):281-8.
5. Corriveau RA, Koroshetz WJ, Gladman JT, Jeon S, Babcock D, Bennett DA, et al. Alzheimer's disease–related dementias summit 2016: National research priorities. Neurology. 2017;89(23):2381-91.
6. Bath PM, Wardlaw JM. Pharmacological treatment and prevention of cerebral small vessel disease: a review of potential interventions. International Journal of Stroke. 2015;10(4):469-78.
7. Wardlaw JM, Smith C, Dichgans M. Mechanisms of sporadic cerebral small vessel disease: insights from neuroimaging. The Lancet Neurology. 2013;12(5):483-97.
8. Edrissi H, Schock SC, Cadonic R, Hakim AM, Thompson CS. Cilostazol reduces blood brain barrier dysfunction, white matter lesion formation and motor deficits following chronic cerebral hypoperfusion. Brain Research. 2016;1646:494-503.
9. Debette S, Markus H. The clinical importance of white matter hyperintensities on brain magnetic resonance imaging: systematic review and meta-analysis. Bmj. 2010;341.
10. Wardlaw JM, Smith EE, Biessels GJ, Cordonnier C, Fazekas F, Frayne R, et al. Neuroimaging standards for research into small vessel disease and its contribution to ageing and neurodegeneration. The Lancet Neurology. 2013;12(8):822-38.
11. DeCarli C, Miller BL, Swan GE, Reed T, Wolf PA, Carmelli D. Cerebrovascular and brain morphologic correlates of mild cognitive impairment in the National Heart, Lung, and Blood Institute Twin Study. Archives of neurology. 2001;58(4):643-7.
12. Nordahl CW, Ranganath C, Yonelinas AP, DeCarli C, Fletcher E, Jagust WJ. White matter changes compromise prefrontal cortex function in healthy elderly individuals. Journal of cognitive neuroscience. 2006;18(3):418-29.
13. Nordahl CW, Ranganath C, Yonelinas AP, DeCarli C, Reed BR, Jagust WJ. Different mechanisms of episodic memory failure in mild cognitive impairment. Neuropsychologia. 2005;43(11):1688-97.
14. Maillard P, Carmichael O, Harvey D, Fletcher E, Reed B, Mungas D, et al. FLAIR and diffusion MRI signals are independent predictors of white matter hyperintensities. American Journal of Neuroradiology. 2013;34(1):54-61.
15. Yang G, Tian Q, Leuze C, Wintermark M, McNab JA. Double diffusion encoding MRI for the clinic. Magnetic Resonance in Medicine. 2018;80(2):507-20.
16. Westin C-F, Szczepankiewicz F, Pasternak O, Özarslan E, Topgaard D, Knutsson H, et al., editors. Measurement tensors in diffusion MRI: generalizing the concept of diffusion encoding. Medical Image Computing and Computer-Assisted Intervention–MICCAI 2014: 17th International Conference, Boston, MA, USA, September 14-18, 2014, Proceedings, Part III 17; 2014: Springer.
17. Szczepankiewicz F, Lasič S, van Westen D, Sundgren PC, Englund E, Westin C-F, et al. Quantification of microscopic diffusion anisotropy disentangles effects of orientation dispersion from microstructure: applications in healthy volunteers and in brain tumors. Neuroimage. 2015;104:241-52.
18. Szczepankiewicz F, Westin CF, Nilsson M. Maxwell‐compensated design of asymmetric gradient waveforms for tensor‐valued diffusion encoding. Magnetic resonance in medicine. 2019;82(4):1424-37.
19. Tournier J-D, Smith R, Raffelt D, Tabbara R, Dhollander T, Pietsch M, et al. MRtrix3: A fast, flexible and open software framework for medical image processing and visualisation. Neuroimage. 2019;202:116137.
20. Veraart J, Novikov DS, Christiaens D, Ades-Aron B, Sijbers J, Fieremans E. Denoising of diffusion MRI using random matrix theory. Neuroimage. 2016;142:394-406.
21. Veraart J, Fieremans E, Novikov DS. Diffusion MRI noise mapping using random matrix theory. Magnetic resonance in medicine. 2016;76(5):1582-93.
22. Smith SM, Jenkinson M, Woolrich MW, Beckmann CF, Behrens TE, Johansen-Berg H, et al. Advances in functional and structural MR image analysis and implementation as FSL. Neuroimage. 2004;23:S208-S19.
23. Andersson JL, Skare S, Ashburner J. How to correct susceptibility distortions in spin-echo echo-planar images: application to diffusion tensor imaging. Neuroimage. 2003;20(2):870-88.
24. Tustison NJ, Avants BB, Cook PA, Zheng Y, Egan A, Yushkevich PA, et al. N4ITK: Improved N3 Bias Correction. IEEE Transactions on Medical Imaging. 2010;29(6):1310-20.
25. Zhao C, Dewey BE, Pham DL, Calabresi PA, Reich DS, Prince JL. SMORE: A Self-Supervised Anti-Aliasing and Super-Resolution Algorithm for MRI Using Deep Learning. IEEE Trans Med Imaging. 2021;40(3):805-17.
26. Zuo L, Liu Y, Xue Y, Dewey BE, Remedios SW, Hays SP, et al. HACA3: A unified approach for multi-site MR image harmonization. Computerized Medical Imaging and Graphics. 2023;109:102285.
27. Zhang J, Zuo L, Dewey BE, Remedios SW, Hays SP, Pham DL, et al. Harmonization-enriched domain adaptation with light fine-tuning for multiple sclerosis lesion segmentation. arXiv preprint arXiv:231020586. 2023.
28. Galluzzi S, Lanni C, Pantoni L, Filippi M, Frisoni GB. White matter lesions in the elderly: pathophysiological hypothesis on the effect on brain plasticity and reserve. Journal of the neurological sciences. 2008;273(1-2):3-9.
29. Lockhart SN, DeCarli C. Structural imaging measures of brain aging. Neuropsychology review. 2014;24:271-89.
30. Maillard P, Fletcher E, Harvey D, Carmichael O, Reed B, Mungas D, et al. White matter hyperintensity penumbra. Stroke. 2011;42(7):1917-22.
31. Kern KC, Zagzoug MS, Gottesman RF, Wright CB, Leigh R. Diffusion tensor free water MRI predicts progression of FLAIR white matter hyperintensities after ischemic stroke. Frontiers in Neurology. 2023;14.
Figures